

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disorder mainly affecting synovial joints. In addition to articular symptoms, extra-articular manifestations can be seen in approximately 40% of patients at some point during the course of their disease (1). The most serious extra-articular manifestation of RA is rheumatoid vasculitis, which encompasses high rates of morbidity and mortality. Rheumatoid vasculitis can affect small to medium-sized vessels of any organ system, thus is extremely heterogeneous in clinical presentation (2). Skin and the peripheral nervous system are the most commonly involved organ systems, followed by the eyes and pericardium. Involvement of other major organ systems such as lung, gastrointestinal (GI) tract, kidney, and central nervous system are rare but when occurs, can be organ or life threatening. Rheumatoid vasculitis is usually associated with seropositivity and represents a complication of long standing, erosive, and deforming RA (3). Although few cases have been reported, development of rheumatoid vasculitis within the first 5 years of RA diagnosis is extremely unusual. We report an unusual case of rheumatoid vasculitis involving hepatic artery which occurred in very early course of the disease.
CASE DESCRIPTION
A 72-year-old woman was referred to our rheumatology clinic on December 2, 2014 due to painful swelling of her hand joints and edema and purplish discoloration of both of her legs, which insidiously developed over the past 2 months. She had 3 kg of weight loss during the 2 months period. She had a past history of pulmonary tuberculosis which was diagnosed and treated 30 years ago, and an epileptic event as a consequence of obstetric complication. Her medications include phenytoin and phenobarbital. She had never smoked and did not drink. On examination, she was afebrile and her blood pressure was normal. Joint exam revealed tender joint count of 15 and swollen joint count of 15 involving metacarpophalangeal, proximal interphalangeal, metatarsal, and ankle joints. Skin examination revealed livedo reticularis on lower extremities, but subcutaneous nodule was not noted. There was 2+ peripheral edema on lower extremities. Chest, heart, and abdominal examinations were not remarkable. Laboratory examinations revealed white blood cell count of 9,800/μL, hemoglobin 10.0 g/dL, and platelet count 411 × 103/μL. Serum creatinine and urinalysis was within normal limits. Her hepatic function panel was abnormal with markedly elevated alkaline phosphatase (ALP, 738 IU/L) and serum γ-glutamyl transpeptidase (GGT, 389 IU/L). Aspartate transaminase (AST) and alanine transaminase (ALT) levels were mildly elevated with values of 44 IU/L and 37 IU/L, respectively. Creatine kinase was normal. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) was markedly elevated at 80 mm/hr and 13.29 mg/dL (reference range, < 0.3 mg/dL). Antinuclear antibody (ANA) was positive at 1:320 titer with nucleolar pattern. Antiphospholipid antibodies and the extractable nuclear antigen antibodies were negative. Rheumatoid factor (RF) was elevated at 206.9 IU/mL. The anti-citrullinated protein antibody (ACPA; including anti-cyclic citrullinated peptide [anti-CCP]), antineutrophil cytoplasmic antibodies (ANCA) against myeloperoxidase and proteinase 3, anti-mitochondrial antibody, anti-smooth muscle antibody, and cryoglobulin were all negative. Tests for hepatitis were all negative. Immunologic studies revealed polyclonal gammopathy with elevated immunoglobulin G (IgG) level at 2,010 mg/dL (reference range, 700–1,600 mg/dL). On serum electrophoresis, no monoclonal band was found. Complement levels were within normal limit.
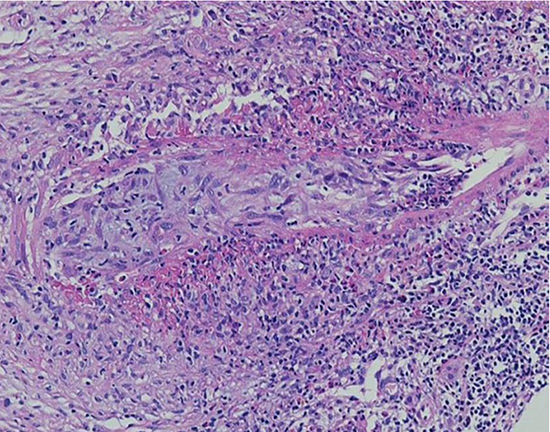
Ultrasound examination of the liver showed no biliary tract obstruction. Doppler ultrasonography of lower extremities showed no evidence of deep vein thrombosis. A percutaneous needle liver biopsy revealed arteritis of a medium-sized hepatic artery of a portal tract with no significant lobular and porto-periportal inflammatory activity (Fig. 1). The arterial wall showed necrosis with inflammatory cell infiltration consisting of lymphocytes, histiocytes, neurophils, and eosinophils. The vascular lumen is almost entirely occluded by reactive intimal tissue. The patient was diagnosed with rheumatoid vasculitis involving hepatic arteries based on Bacon and Scott criteria for rheumatoid vasculitis (4). The patient fulfilled a criterion of biopsy evidence of acute necrotizing arteritis plus systemic illness (weight loss) in a patient with RA. The patient was treated with high dose methylprednisolone (40 mg/day) and cyclophosphamide 500 mg IV pulse every 2 weeks for 6 cycles. Ten months after treatment initiation, the patient's liver function normalized, ESR, and CRP decreased to normal level, and her RA was in remission state. She has been maintained on deflazacort 12 mg, methotrexate 10 mg weekly, tacrolimus 1.5 mg, and aspirin 100 mg. Her only complaint at present is lower leg swelling and livedoid rash.
 | Fig. 1Features of liver biopsy. Liver biopsy revealed necrotizing vasculitis of medium-sized hepatic artery of a large portal tract. The vascular wall showed necrosis with inflammatory cell infiltration and fibrin deposition forming granulomatous vasculitis. The vascular lumen is occluded due to intimal hyperplasia with inflammatory cell infiltration (H & E stain, × 200).
H & E = hematoxylin and eosin.
|
DISCUSSION
Rheumatoid vasculitis typically occurs in patients with long-standing seropositive RA with destructive joints. The onset of rheumatoid vasculitis is usually 10–14 years after the diagnosis of RA (3). In addition, autoantibodies (RF, anti-CCP, and ANA) and immune complexes are invariably detected in rheumatoid vasculitis patients (1). Interestingly, our patient presented with rheumatoid vasculitis within 2 months of RA onset. Our patient fulfilled the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria for RA (5) with a score of 10 with high titers of RF and ANA. Extensive investigations did not reveal evidences of other systemic causes such as malignancy or systemic vasculitis. This occurrence of rheumatoid vasculitis at early stages of disease is unusual with only 2 previously reported cases which occurred within 1 week and 12 months of onset (67). Vasculitis usually develops in established disease with burnt out synovial inflammation implying that inflammatory burden over long period of time is important in the pathogenesis of rheumatoid vasculitis (3). Our case may reflect unusual widespread impact of intense systemic inflammation in a RA patient with early aggressive disease.
Rheumatoid vasculitis is a clinicopathologic condition. Definitive diagnosis of rheumatoid vasculitis usually requires histologic evidence of systemic necrotizing vasculitis involving small to medium-sized vessels. Histopathologic examination reveals fibrinoid necrosis and mononuclear and neutrophil infiltration of the vessel walls (8). Rheumatoid vasculitis can involve any organ systems and clinical manifestations depend on size and types of the involved blood vessels. In a case control study, the skin or peripheral nerves were involved in more than 80% of the cases, and these organ involvements were shown to have a favorable prognosis (3). Involvement of major organs such as lung, kidney, heart, central nervous system, and GI tracts are less common but often associated with poor prognosis (9). GI involvements have been reported in 10% of the patients with rheumatoid vasculitis with mesenteric vasculitis as the most common manifestation (9). Although commonly reported in polyarteritis nodosa (PAN), hepatic arteritis as a manifestation of rheumatoid vasculitis is extremely rare. The incidence of hepatic arteritis in 120 autopsy patients with collagen diseases revealed 100% in PAN whereas 8.7% in RA (10). Pathologically, hepatic arteritis associated with rheumatoid vasculitis can be differentiated from that of PAN by absence of microaneurysm (11). Our patient presented with liver cholestasis with high levels of ALP and GGT in association with active rheumatoid joint inflammation. Common liver pathologies associated with systemic connective tissue diseases such as primary biliary cirrhosis, autoimmune cholangitis, or autoimmune hepatitis were considered before the histologic assessment, but biopsy findings revealed necrotizing vasculitis of hepatic arteritis without portal inflammatory activity or microaneurysm. Our case strongly supports the importance of histologic assessment in the diagnosis of liver diseases associated with systemic connective tissue diseases.
Management of rheumatoid vasculitis is largely empirical due to lack of randomized control trials. Corticosteroids and cyclophosphamide have been historically used for severe forms of rheumatoid vasculitis (12). Despite treatment with high dose glucocorticoids and cyclophosphamide, mortality rates are reported to be high with 12% at 1 year and 60% at 5 years (13). The major cause of death was infection followed by organ damage from active vasculitis. The availability of biologic drugs for RA treatment has broadened treatment options for rheumatoid vasculitis. However, the role of these drugs in rheumatoid vasculitis management needs to be further investigated. There are case reports illustrating efficacy of biologic drugs, especially rituximab in severe refractory rheumatoid vasculitis patients, as efficacy of rituximab was proved in ANCA associated systemic vasculitis (14). Anti-tumor necrosis factor (TNF) therapy seems to be a logical option for rheumatoid vasculitis treatment with their known efficacy in RA, but concerns were raised that these drugs may induce vasculitis (15). Our patient responded well to the high dose corticosteroid and cyclophosphamide induction and methotrexate and tacrolimus maintenance treatment. However, considering high rates of infectious complications from aggressive immunosuppression, we need to develop a better and safer approach for managing rheumatoid vasculitis.
Our case is rare, but we believe that this case includes several important clinical implications. First is that rheumatoid vasculitis can complicate early RA. In such cases with early aggressive disease, vascular inflammation may not be limited to the synovium, but can occur systemically during the immune pathogenesis of RA. Second, the case reminds the medical society of the importance of histopathologic evaluation in the diagnosis of rheumatoid vasculitis. Especially in patients with liver abnormalities associated with systemic connective tissue diseases, histopathology can be crucial in defining the underlying cause. Finally, early aggressive treatment can halt organ damage from active vasculitis as well as increase chance of achieving remission of RA.
 XML Download
XML Download