

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Trauma is the fourth most common cause of death in Korea, following cancer, cardiovascular disease, and cerebrovascular disease. It is the most common cause of death in individuals aged < 40 years (1). In addition, trauma is believed to be the leading cause of death among individuals between the ages of 10 and 40 years in developed countries, according to the World Health Organization (2). Moreover, mortality from trauma is not the only problem; Trunkey (3) reported that for every death, 2 patients remain permanently disabled. However, over the past several years, significant improvements have been achieved in survival after trauma. One of the reasons for this progress has been the improvements in emergency medical services (EMS) and life-saving transport of trauma patients to a center capable of providing definitive care. The rapid and timely transport of trauma patients to an appropriate trauma institution, that is, “getting the right patient to the right place at the right time,” is important in increasing the survival rate in trauma patients (4).
Helicopter emergency medical services (HEMS) has its origins in military evacuation by air transport during the Korean War. Its use in civilian situations was initiated in the 1960s in the United States. Since then, it has played an important role in prehospital emergency medical systems (56). Rapid transport of major trauma patients to a definitive care center is a cornerstone of modern trauma systems, and delay in this element of care is a widely known cause of mortality (7). Thus, HEMS in this context has become an important component of trauma care. The advantages of helicopter transport are believed to be related to the ability of helicopters to reach patients in remote areas, to facilitate expeditious transport to a definitive trauma care center, and to deliver trained medical experts to the scene of injury (8910). Some investigators have raised controversial issues regarding the outcomes of air transport, and the use of aeromedical transport, which must be justified in view of its growing safety and economic considerations, has been the subject of increasing investigation (111213). However, recent evidence has demonstrated the survival benefits and cost-effectiveness of air transport of trauma patients (14151617).
The Korean government has recently launched the hospital-based HEMS (H-HEMS), known as an exclusive emergency medical helicopter dedicated solely to the transport of patients with medical emergencies. H-HEMS was initiated in September 2011 and has been actively used as a direct mode of transportation and interhospital transportation for critically ill patients. Medical crew experts on board provide specialized primary emergency care during the daytime, 7 days per week. Currently, the service is operated by 6 different hospitals nationwide. In our institution, in Gangwon province, H-HEMS was introduced in 2013, and has been in continuous operation since that time. The purpose of the present study was to evaluate the effectiveness of H-HEMS in improving mortality outcomes in major trauma patients transported by helicopter in comparison with those transported by ground ambulance.
MATERIALS AND METHODS
Patient data
The subjects included all adult patients who experienced major traumas with injury severity scores (ISSs) of ≥ 15 points and were transferred directly or transferred from other hospitals. According to the Korean Triage and Acuity Scale (KTAS), used as a patient severity/urgency classification tool in the emergency department (ED) in Korea, patients aged 15 years or older are regarded as adults; thus, adults aged 15 years or older were included in the study. Furthermore, the study included all injuries by both blunt and penetrating mechanisms. Participants were divided into 2 groups according to the type of transport to the trauma center; that is, either via ground emergency medical services (GEMS) or via H-HEMS. According to the standard protocols for 119 EMS providers published by the fire department, when selecting a transport mode for emergency patients, it is required to consider air transportation if the distance from the site to the hospital is greater than 30 km. Therefore, our research was performed on patients who were transferred to our hospital (level 1 trauma center in a tertiary hospital with 851 hospital beds) via H-HEMS and GEMS from a distance of over 30 km. Outcomes in the patients transported by helicopter were compared with outcomes in the patients transported by ground ambulance. The research period was 22 months, from October 1, 2013 to July 31, 2015. Data were collected from 3 databases, medical records in emergency medical helicopters, the National Emergency Department Information System (NEDIS), and the Korean Trauma Data Bank (KTDB) in our hospital. The NEDIS and KTDB were created and managed by the National Emergency Medical Center to serve as central national data repositories. It is mandatory for a regional emergency medical center and regional trauma center such as our institution to participate in the NEDIS and KTDB registry.
Outline of H-HEMS
H-HEMS is operated in each hospital and sponsored by the Ministry of Health and Welfare and the local government in the location of the hospital. The hospital provides the human resources such as the medical staff and the company in charge of the general operation and maintenance of the helicopter. The decision regarding helicopter transportation in major trauma patients is determined via hotline communication between the hospital and the fire department or between the hospital and the referring hospital. When a request for patient transport is received by the hospital, the medical and aviation mission acceptance processes proceed simultaneously. All missions must be approved by the attending emergency physician to be cleared for acceptance from a medical perspective. The mission request must also meet the approval of the helicopter pilot and aviation operator, who consider the aviation risks. The decision regarding acceptance has to be made within 1 minute, and the mission should be initiated within 10 minutes. Primary care for major trauma is provided at the scene of the injury and en route to the trauma center by the emergency physician, as well as a nurse or emergency medical technician (EMT). All patients transported via H-HEMS receive advanced care directly from the medical staff dispatched to the field in accordance with the Advanced Trauma Life Support (ATLS) guidelines. In our institution, > 300 missions are performed per year, and about 28% of all mission requests are rejected in consideration of either medical or aviation-related factors, such as weather.
Analytical strategy
The variables used in this study included age, sex, transport type, ISS, injury type, injury to hospital time, and death. We also included crew configuration (1 physician, 1 nurse or 1 EMT, and 2 pilots) and transportation distance data. Patient death was defined as all deaths during hospitalization (excluding death on arrival) as reported in the NEDIS and KTDB. Initial vital signs such as systolic blood pressure (SBP), respiratory rate (RR), and Glasgow Coma Scale (GCS) score were recorded for all patients on arrival at the ED of a level 1 trauma center and used to calculate the revised trauma score (RTS). Furthermore, abbreviated injury scale (AIS) coding was performed by the dedicated trauma physician on duty, and the results were reviewed by a trauma coordinator and the dedicated trauma physician again. These values were used to calculate the probability of survival (POS) using the Trauma and Injury Severity Score (TRISS) equation.
The primary outcome of this study was the mortality of the transferred major trauma patients. TRISS is an instrument used for predicting the outcome of trauma patients, and it is globally accepted for determination of the effect of HEMS on trauma-related mortality (1819). In 1982, the American College of Surgeons Committee on Trauma (ACSCOT) coordinated the Major Trauma Outcome Study (MTOS), which became a standard reference database of major trauma patients in the United States, and was the basis for the development of the TRISS method that has become familiar to trauma experts (20). Furthermore, POS norms using the TRISS index are the basis for the MTOS analyses supporting quality assurance actions and outcome evaluations. TRISS analysis is used to calculate the POS of a trauma patient on the basis of the patient's ISS, RTS, and age. Using the TRISS method, the POS can be estimated from the following formula:
The coefficients b0 − b3 are derived from Walker-Duncan regression (multiple regression) analysis from numerous trauma patients analyzed in the MTOS. The constant e−b is equal to 2.718282 (the Napierian logarithms). A refers to patient's age. If the age is under 54 years, A is equal to 0. A is equal to 1 if the age is over 55 years. b0 − b3 are coefficients that are different for penetrating and blunt trauma. If the patient's age is less than 15, the blunt coefficients are used regardless of the injury mechanism (21).
Z and W statistics were calculated in the present study to compare predicted and actual patient mortality (20). The Z statistic was used to compare the mortality of the sample population with the MTOS-predicted mortality to determine whether the outcomes in the sample population were significantly better, the same, or worse than the predicted mortality. The W statistic was used to measure the number of unexpected survivals or deaths per 100 patients.
Statistical analysis
We used SPSS version 20 (IBM Corp., Armonk, NY, USA) for all statistical analyses. Continuous data were summarized in terms of proportions, means, and medians with their interquartile ranges (IQRs). We compared the patients' demographic characteristics and mortality using the Mann-Whitney U test or χ2 test analysis, as appropriate. Predicted mortality and actual patient mortality were compared using the Z and W statistics. The W statistic was used to calculate the number of survivors more or less than the MTOS norm per 100 patients analyzed, and provides more accurate comparisons between different institutions or systems.
RESULTS
During the study period, 699 patients met the inclusion criteria and were thus included in the analysis. Of these patients, 312 were finally included in the study. Sixty-three missions for adult major trauma patients used H-HEMS during the 22 months of interest. The adult trauma GEMS group consisted of 249 patients (Fig. 1). The median patient age was 55 (40.3–67.0) years, and 226 (72.4%) patients were men. No statistically significant differences in mean age, sex, SBP at ED visit, or ISS were found between patients in the H-HEMS and GEMS groups. The GCS scores on arrival at the ED were lower in the patients transported via H-HEMS (Table 1). A significant difference was found in the percentage of scene calls (P = 0.004) between the 2 groups (12.7% in the H-HEMS group vs. 30.5% in the GEMS group). No significant difference in transportation distance was observed between the 2 groups, but transportation time was much shorter in the H-HEMS group. Air transport had a longer event-to-emergency room (ER) time (defined as period from injury to arrival at the ED in a level 1 trauma center) than ground transportation in direct transport (P = 0.006). In contrast, ground transportation had a longer event-to-ER time than air transport in interhospital transport (P = 0.008). Of all patients, 47.6% were involved in traffic accidents, which were the most common cause of injuries (Table 2). ISS did not significantly differ between the 2 groups, but RTS was lower in the H-HEMS group than in the GEMS group (H-HEMS, 6.98; GEMS, 7.30). Thus, the injury severity was greater in the H-HEMS group (P = 0.039; Table 2).
 | Fig. 1Study flow diagram detailing the selection of patients from the KTDB in our hospital.
KTDB = Korean Trauma Data Bank, H-HEMS = hospital-based helicopter emergency medical services, GEMS = ground emergency medical services, ISS = injury severity score.
|
Table 1
Comparison of general characteristics between H-HEMS and GEMS groups
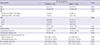
Values are presented as median (IQR) or number (%).
H-HEMS = hospital-based helicopter emergency medical services, GEMS = ground emergency medical services, SBP = systolic blood pressure, GCS = Glasgow Coma Scale, ISS = injury severity score, ED = emergency department, ICU = intensive care unit, IQR = interquartile range.
![]()
Table 2
Comparison of injury mechanism, ISS, and RTS
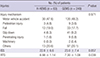
Data are shown as mean ± SD or number (%).
ISS = Injury Severity Score, RTS = revised trauma score, H-HEMS = hospital-based helicopter emergency medical services, GEMS = ground ambulance emergency medical services, SD = standard deviation.
![]()
The survival rate of trauma patients at hospital discharge was 90.0% in the H-HEMS group and 88.9% in the GEMS group. Z and W statistics were also compared for patients in the H-HEMS and GEMS groups (Table 3). TRISS analysis revealed that 6.32 more lives per 100 patients transported were saved in the H-HEMS group (Z statistic = 1.56), and the Z statistic in the GEMS group was 0.84, but the difference was not statistically significant in either group (P values, 0.119 vs. 0.400). The patients transported and treated with H-HEMS showed a survival potential of 4.74 more patients per 100 patients than those transported and treated using GEMS.
Table 3
Comparison of clinical outcomes between H-HEMS and GEMS groups
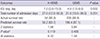
Values are presented as median (IQR) or number (%).
H-HEMS = hospital-based helicopter emergency medical services, GEMS = ground ambulance emergency medical services, ICU = intensive care unit, IQR = interquartile range.
*Significance level for Z statistical values.
![]()
We performed a subgroup analysis, however, as the number of cases of on-scene transport by H-HEMS in our data set was small, we only showed the results using data reclassified by interhospital transfer mode (Table 4). In the H-HEMS group, 87.3% (n = 55) of the patients were selected. The H-HEMS and GEMS groups classified based on interhospital transport were compared in terms of survival rate using TRISS. The Z and W statistics revealed significantly higher scores in the H-HEMS group than in the GEMS group (Z statistic, 2.02 vs. 1.16; P value, 0.043 vs. 0.246; W statistic, 8.87 vs. 2.85); furthermore, 6.02 more patients could be saved per 100 patients when H-HEMS was used for interhospital transportation (Table 4).
Table 4
Analysis of clinical outcomes in interhospital transportation of major trauma patients between H-HEMS and GEMS groups
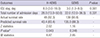
Values are presented as median (IQR) or number (%).
H-HEMS, hospital-based helicopter emergency medical services; GEMS, ground ambulance emergency medical services, ICU = intensive care unit, IQR = interquartile range.
*Significance level for Z statistical values.
![]()
DISCUSSION
The preventable death rate of trauma patients in Korea was 35.2% in 2010 (22). This high mortality can be attributed to the insufficiency of prehospital trauma care, absence of an appropriate trauma system, and relative shortage of level 1 trauma centers in comparison with other developed countries. Hence, the use of hospital-based aeromedical transportation, the so-called physician-loaded exclusive emergency medical helicopter, for trauma patients has increased in Korea. Not only patients with trauma but also those with medical diseases who have difficult access to regional emergency medical centers owing to geographical situations such as a mountainous or islet region can use the air ambulance services. Several researchers have used the retrospective TRISS methodology to evaluate the usefulness of air ambulances in transporting trauma patients. The results have been varied, but most studies have shown good outcomes (5623). However, although air ambulances have demonstrated survival benefits for major trauma patients, concerns about cost, safety, and over-triage remain significant problems, acknowledged even in studies supporting helicopter transport (2425). Moreover, the effectiveness of this form of transport in the Korean trauma system is not clear.
The actual survival rate of trauma patients in our study seems to be similar in the 2 groups (Table 4). However, absolute unadjusted mortality, such as the above result, is a crude value because it did not consider measured confounders. TRISS analysis could provide for adjustment of these confounders. By comparing both the H-HEMS and GEMS groups with matched trauma patients from the MTOS data set, we could use the TRISS method to explain survivors who were predicted to die and patients who died but were predicted to survive. A direct comparison between the 2 groups does not explain this. When we compared the 2 groups with TRISS analysis, the Z and W statistics revealed significantly higher scores in the H-HEMS group than in the GEMS group in interhospital transport; furthermore, 6.02 more patients could be saved per 100 patients with the use of air transport (Table 4). To our knowledge, this study is the first to report that interhospital transport via H-HEMS is associated with an improved survival rate for major trauma patients in Korea. Among patients transported to level 1 trauma centers via H-HEMS, 100 would need to be transported to save 8.9 lives (Table 4). This result is consistent with the findings of Mitchell et al. (26), who reported the results of the first large Canadian TRISS analysis of adult blunt trauma patients, showing the benefit of H-HEMS and reporting that patients with an ISS of > 12 had a W score of 6.4, indicating 6.4 more survivors per 100 patients transported via air ambulance than via ground ambulance. Frankema et al. (15) also found that blunt trauma patients transported via helicopter had a statistically significant improvement in survival rate, and they investigated the effect of helicopter delivery by a highly trained medical crew. Our study also included 98.4% of blunt trauma patients transported via air transport with medical experts (Table 2). Contrary to the findings of our research, Kang et al. (27) reported earlier that H-HEMS was not able to decrease the mortality rate of trauma patients in Korea. However, their study had several limitations. First, the calculation of ISS was inaccurate because the ISS of their study population was calculated based on the International Classification of Diseases (ICD) diagnosis rather than on the actual diagnosis with detailed description. Therefore, many diagnoses were unclear or omitted. Moreover, some major trauma patients did not receive treatment according to ATLS guidelines and a team approach, because at that time, the hospital was not a level 1 trauma center. In the present study, the research was conducted after a level 1 trauma center and National Trauma Data Bank had been established. Therefore, our study results are more reliable than those of the previous study.
The event-to-ER time in both groups appeared greatly prolonged, especially in interhospital transportation compared to direct transport (Table 1). However, this is expected and may reflect several factors. This time potentially includes hours spent at a local hospital for initial work-up and stabilization, and a failure to follow ATLS guidelines. In addition, our province is a rural area with a geographically widespread population that may require long transports. The mean RTS of the air transport patients was 6.98, which was lower than the 7.30 (mean value) of the patients in the GEMS group (Table 2). Moreover, among the trauma patients transported via H-HEMS, the number with a GCS < 8 was 20 (31.7%) (Table 1), which was a significantly higher frequency than that among the patients transported via GEMS (P = 0.003). Thus, the trauma severity of the patients transported via air transportation was higher. Nevertheless, the survival rate in the H-HEMS group was higher than that in the GEMS group in interhospital transport. Similarly, in the study by Ryb et al. (28), when patients were stratified according to hospital RTS, the patients with an RTS of < 6 at the hospital setting (n = 16,867) exhibited a positive adjusted survival effect linked to air transport. Moreover, the study by Brown et al. (29) also confirmed that patients with GCS scores of < 14 had improved survival when transported via helicopter.
Any beneficial effect of helicopter transport to a designated level 1 trauma center is the result of the combination of rapidity, medical expertise, and disposition of the transport (8). In the present study, the mean transportation time via H-HEMS was much shorter than that via GEMS. Moreover, in interhospital transport, the time from the event to arrival at the level 1 trauma center demonstrated a greater decrease in H-HEMS than in GEMS (Table 1). This is 1 of the reasons for the increased survival rate of trauma patients in interhospital transport. Another cause of the improvement in survival rate with H-HEMS might be the appropriate treatment administered by the medical experts during the transportation. This is in keeping with the findings of other helicopter transport research studies that suggested that the important benefit conferred by helicopter transport was the advanced skills provided by the air medical crew, as opposed to expedited transport times (18303132). Helicopter medical personnel may be trained to perform potentially life-saving procedures such as rapid sequence intubation, surgical airway, or transfusion, which ground EMTs cannot perform (33). Moreover, members of the helicopter crew have exposure to a larger volume of injury patients, affording them more experience with management of severe injuries. In Korea, study of Jung et al. (34) also confirmed the positive effects of physician-staffed helicopter transport, although the comparison was between physician- and non-physician-staffed helicopter transport.
Kim et al. (35) reported the advantage of helicopter transportation based on the fire department system over ground transportation. However, the median helicopter transport time in that study was 60 minutes. In the present study, the median transport time by H-HEMS was shorter, at 30 minutes. The longer median transport time by helicopter transportation based on the fire department system may be attributable to the time required to prepare for helicopter takeoff, landing, and boarding the medical staff. Meanwhile, H-HEMS is based on the hospital system, which means that medical personnel can be transferred to trauma patients with a much shorter takeoff time. The mean takeoff time by H-HEMS is about 9 minutes. In the present study, the median transport time by GEMS was 65 minutes, exceeding the so-called golden hour, which is the time from the accident to the definitive treatment. Although Kim et al. (35) reported that the mean transport time by GEMS was 57 minutes, they did not report any information on patient transfer distance contrary to our study, and whether the study population was comparable with the population transported via H-HEMS was unclear. Diaz et al. (36) showed that helicopter transport was faster than ground transport when requested by scene personnel for a patient who was 45 miles from the trauma center, making patients in this distance range the most likely to benefit from more rapid transport to definitive care centers by helicopter. Nicholl et al. (37) compared the performance of helicopter transport with that of ground transport in a rural area and concluded that the transport time to the hospital was 10 minutes faster by helicopter than that predicted for ground transport of trauma patients. This result supports our findings of a faster transport time by air transport.
This study has a few limitations. First, it was subject to the difficulties associated with retrospective database reviews, such incomplete or missing data and the absence of prehospital physiological data. Second, we used the vital signs and GCS scores initially measured at level 1 trauma centers, not those measured at the prehospital stage or at the accident scene. This is because precise values for physiological parameters were difficult to obtain before arrival at the trauma center and were consequently inaccurate. However, our other prehospital and hospital information was very reliable. This is because the NEDIS, H-HEMS registry, and KTDB in our hospital are managed strictly by the government, and the trauma coordinator and researcher checked the integrity of a large volume of data to minimize the unreliable values. Third, this was not a population-based study, and the sample size was small. Thus, the sample from a single level 1 trauma center in a mostly suburban area may not be representative of the patient population transported via H-HEMS in Korea. But, since our hospital is the only definitive care institution and also our province operates the only single H-HEMS system and single EMS system, our study may be representative of the local trauma system in our province. However, our results require careful application in individual transport systems for trauma patients. Another limitation of this study was that there were fewer scene calls in the H-HEMS group. This likely reflects the fact that the fire department system in our country lacks recognition of the use of H-HEMS for transportation of trauma patients. Therefore, we could not analyze the on-scene transportation of trauma patients. Lastly, although mortality is an important measure of quality improvement, our study does not incorporate other important patient outcomes such as functional capacity at discharge. Moreover, the TRISS method has some limitations for measurement of survival rate. TRISS relies on physiological parameters and is associated with several problems such as missing data from data sets and the fact that the use of the GCS score in trauma patients has poor interobserver agreement and requires adjustment of scores for intubated patients. It has been poorly predictive of outcomes in the elderly. Comparison of outcomes in the Korean population with those in the MTOS population from the 1980s may also be considered a limitation. Despite these limitations, TRISS is commonly used as the gold standard method for evaluating mortality outcomes in trauma patients (38). While reliable and widely acceptable methods are warranted to compare the results of severe trauma patients, many authors suggest that “TRISS is the most practical and widely used mortality prediction model” (39). Furthermore, there were relatively few potential confounders in this study, because it was conducted within the same patient settings, such as a homogeneous ground and helicopter transport system, homogeneous cooperative dispatch system, and a single level 1 trauma center.
TRISS analysis revealed that interhospital transportation of major trauma patients via H-HEMS was associated with an improved survival rate when compared with GEMS. In Korea, the use of emergent patient transportation via H-HEMS is increasing and is expected to play an important role in the domestic trauma system. This is the first study to show the effectiveness of H-HEMS, and further research on the participation of all exclusive emergency medical helicopter operation institutions is needed.
 XML Download
XML Download