

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Distal radius fractures (DRFs) are one of the most common types of fractures in the adult population, with high prevalence rates reported worldwide (123). DRFs account for approximately 17.5% of all adult fractures (4), with an incidence of greater than 640,000 annually in the United States alone (5). Although DRF is a major public health problem because of its high prevalence and economic burdens, there is no uniform treatment for DRFs. The choice of treatment is likely to be influenced by several factors, such as patient age, fracture pattern, displacement, fracture instability, availability of resources, and the surgeon's preference (678).
Treatment options for DRFs includes cast immobilization, percutaneous pinning, external fixation, and open reduction with internal fixation (ORIF) using a plate (9). The proportion of cases with DRF undergoing surgical treatment has been growing over recent years (1011). Of these surgical options, ORIF has been performed with increasing frequency since the introduction of the volar locking plate system (112), and younger surgeons are more likely to perform ORIF (13). However, most previous epidemiological studies on surgical trends in DRFs have been confined to European countries and North America (112). The epidemiological features of DRFs may vary among populations and are associated with race, socio-economic status, culture, and degree of urbanization (14). To the best of our knowledge, no epidemiologic studies have assessed surgical trends for DRFs in Asian countries.
Thus, the first aim of the present study was to examine national surgical trends for the management of DRFs in Korea based on an analysis of nationwide data acquired from the Korean Health Insurance Review and Assessment Service (HIRA). Since it is expected that a preference for certain surgical options may vary according to the healthcare institution type (7), the secondary aim was to examine the surgical trends according to the healthcare institution type.
MATERIALS AND METHODS
Data source
The authors analyzed a nationwide database obtained from the HIRA from 2011 to 2015. In Korea, 97% of the entire population are legally obligated to enroll in the National Health Insurance (NHI) program. Patients only pay about 30% of the total medical cost to health care institutions, and all healthcare providers submit claims data for inpatient and outpatient management, including diagnostic codes which classified according to the International Classification of Diseases, 10th revision (ICD-10), procedure codes, prescription records, demographic information, and direct medical costs, to the HIRA to request reimbursement for the remaining 70% of the medical cost from the NHI service. Of the remaining 3% of the population not registered in the NHI program, excluding illegal residents, most receive healthcare coverage through the Medical Aid Program. The claim data for patients covered by the Medical Aid Program are also reviewed by the HIRA. Hence, medical records of almost all newly admitted or hospitalized patients at health care institutions in Korea are prospectively recorded in the HIRA data.
Data collection
We conducted a survey of patients aged ≥ 20 years with newly diagnosed DRFs in Korea between 2011 and 2015. Although HIRA data provide patient identifiers, if a patient with DRF makes multiple visits to a healthcare institution, claims data for the number of visits are generated. We avoided the risk of multiple counting as follows. First, patients with DRFs who received surgical treatment were identified with the ICD-10 codes (S52.5 and S52.6) and the operation codes (N0603, N0613, N0607, N0617, N0993, N0994, and N0983) (Table 1). Each operation code was counted as a single case. A patient who received surgical treatment for DRF was considered as one case. A patient who underwent 2 surgical treatments for DRFs was considered as 2 cases, on the assumption that the second surgery was performed on the opposite side. Subsequently, in order to identify patients with DRFs who received conservative treatment, those who underwent surgical treatment were excluded from the HIRA data by using patient identifiers, and those who had splint or cast codes (T6020, T6030, T6151, and T6152) for DRF ICD-10 codes (S52.5 and S52.6) were included (Table 1). For conservative treatment, multiple splint or cast codes are commonly entered for a single case of DRF, because an initially applied splint can be substituted by a cast at a later stage, or a long arm cast can be changed to a short arm cast, etc. For this reason, additional codes entered over a period of 6 months after the initial entry of splint or cast codes were recounted (3). For instance, if a splint or cast code was entered for patient with a DRF at one point, the patient was still considered to be a single case even if an additional code was entered after a month. On the other hand, if a splint or cast code was entered 6 months after the initial entry, it was assumed that a fresh fracture unrelated to the previous one had occurred; therefore, such a patient was counted as 2 cases.
Table 1
ICD-10 diagnosis codes and procedure codes of DRFs
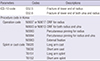
ICD-10 = International Classification of Diseases, 10th revision, DRF = distal radius fracture, ORIF = open reduction with internal fixation.
![]()
We examined patient data to identify the year of the fracture occurrence, the age at which it occurred, the patient's sex, whether surgery was performed, the operation code, and the health care institution type at which the treatment was administered. The types of surgical treatment were classified into 3 main categories: ORIF using plates (N0603, N0613, N0607, and N0617), percutaneous pinning (N0993 and N0994), and external fixation (N0983) (2). In case in which percutaneous pinning and external fixation were performed concurrently, external fixation was considered to be the main procedure and the case was categorized as such. If ORIF and external fixation were performed concurrently, ORIF was considered to be the main procedure. In Korea, health care institutions are classified as clinics, hospitals, general hospitals, and tertiary hospitals. The classification criteria were based on inpatient bed size for clinics (< 30 beds), hospitals (30 to 99 beds), and general hospitals (≥ 100 beds), and tertiary hospitals were defined as general hospitals that are approved to provide most types of advanced medical care and to treat severely ill patients with a minimum of 20 departments. In order to examine the surgical trend in DRFs according to the healthcare institution type, we investigated the proportion of surgical treatment and the types of surgery by healthcare institution type.
Statistical analysis
We calculated age-adjusted and sex-specific incidence rates per 100,000 persons of DRFs, and the 2013 Organization for Economic Cooperation and Development (OECD) population (http://stats.oecd.org) as the standard population. Estimated year-specific, age-specific, and sex-specific populations were obtained from the “Statistics Korea” website (http://www.kosis.kr). Variation in the proportion of surgical treatment and conservative treatment over the years was analyzed with the Cochran-Armitage trend test using SAS statistical software version 9.13 (SAS Institute, Cary, NC, USA). Values of P < 0.05 were considered significant.
RESULTS
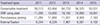
A total of 459,388 DRFs (440,127 patients) occurred from 2011 to 2015. Of these, 111,628 cases (107,664 patients) involved men patients, and 347,760 cases (332,463 patients) involved women patients, with a men to women ratio of 3.12. The mean age of patients with DRFs was 59.5 years (standard deviation [SD] ± 14.2). The mean age of men was 51.7 years (SD ± 16.1), and that of women was higher at 62.0 years (SD ± 12.6). The total number of DRFs increased from 2011 to 2013 (88,336 in 2011 and 101,883 in 2013), and then it decreased after 2013 (90,330 in 2014 and 81,877 in 2015) (Table 2). The age-adjusted incidence rate per 100,000 population also increased between 2011 and 2013 (269.45 in 2011 and 290.12 in 2013), and then began to decrease (250.08 in 2014 and 220.23 in 2015) (Table 2).
Table 2
Number of cases and age-adjusted rates of DRFs from 2011 to 2015
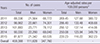
DRF = distal radius fracture, OECD = Organization for Economic Cooperation and Development.
*Use of the OECD population in 2013 as the control.
![]()
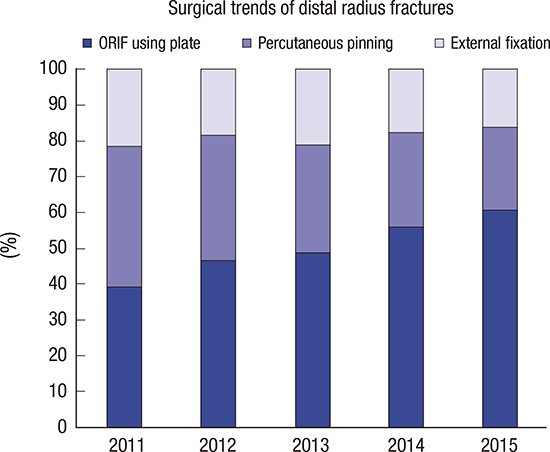
Of the overall 459,388 DRF cases, 164,602 cases (35.8%) were managed using surgical treatment. The proportion of DRF cases treated by surgery increased from 32.6% in 2011 to 38.3% in 2015, showing a steadily increasing trend over the years, which was found to be significant using the Cochran-Armitage trend test (Fig. 1, P < 0.001). In terms of the type of surgery, the proportion of cases treated with ORIF using a plate tended to increase each year, from 39.2% of the overall surgeries in 2011 to 60.9% in 2015, while the proportion of percutaneous pinning and external fixation tended to decrease (Fig. 2, Table 3).
 | Fig. 1Proportion of surgical treatment in patients with DRFs, by year.
DRF = distal radius fracture.
|
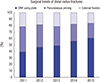 | Fig. 2Proportion of operation type in patients with DRFs, by year.
DRF = distal radius fracture, ORIF = open reduction with internal fixation.
|
Table 3
Treatment trend of DRFs from 2011 to 2015
![]()
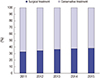
The proportion of overall patients with DRFs was divided according to the healthcare institution type at which the treatment was given; the greatest number of patients with DRFs were treated in clinics (45%, 206,900 cases), followed by hospitals with 30–100 beds (28%, 128,543 cases), general hospitals (22%, 102,964 cases), and tertiary hospitals (5%, 20,981 cases). In terms of the proportion of surgical treatment for DRFs by healthcare institution type, the proportion of surgical treatment in general hospitals was highest at 60%, followed by hospitals with 30–100 beds (55%), tertiary hospitals (54%), and clinics (10%) (Fig. 3). In terms of the type of surgery performed according to the healthcare institution type, ORIF (91%) was the most popular procedure in tertiary hospitals, while percutaneous pinning (58%) was most popular in clinics. In addition, general hospitals and hospitals with 30–100 beds had a higher proportion of external fixation than tertiary hospitals and clinics (Fig. 4, Table 4). While external fixation comprised only 10% or less among overall surgeries performed by tertiary hospitals and clinics, it comprised more than 20% of surgeries performed by general hospitals and hospitals with 30–100 beds.
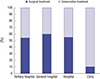 | Fig. 3Proportion of DRFs patients who underwent surgical treatment, by health care institution type.
DRF = distal radius fracture.
|
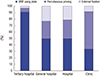 | Fig. 4Proportion of operation type in patients with DRFs, by health care institution type.
DRF = distal radius fracture, ORIF = open reduction with internal fixation.
|
Table 4
Treatment type of DRFs according to the healthcare institution type
![]()
DISCUSSION
The present study indicated that the proportion of surgical treatment for DRFs was found to be increasing steadily over time in Korea, with ORIF becoming more popular. Ninety percent of overall patients with DRFs in small clinics was managed with conservative treatment; however, the proportion of patients treated with surgical treatment was higher than that of patients given conservative treatment in other types of healthcare institutions. The type of surgery used for DRFs varied according to the healthcare institution types, with ORIF (91%) being the most popular procedure in tertiary hospitals, and percutaneous pinning (58%) the most popular in clinics. In addition, general hospitals and hospitals with 30–100 beds used external fixation more frequently than tertiary hospitals and clinics did.
In the U.S. and European countries, surgical treatment as a management of DRF is on the increase, and the proportion of treatments by means of ORIF using a plate, in particular, is increasing (1101112). Some studies have not provided sufficient evidence supporting that internal fixation produces a better clinical outcome than external fixation (1516). However, other studies demonstrated that patients managed with plate fixation had significantly better outcomes than patients managed with external fixation in cases of intra-articular or unstable DRFs (171819). Furthermore, a loss of reduction may occur for a period up to 6 months after external fixation (20). ORIF using a plate has advantages for the restoration of anatomy, as it allows superior visualization, better mechanical stability, and a shortened immobilization period than cast immobilization or external fixation do (21222324). Our study confirms the increasing popularity of this surgical method. Waljee et al. (13) reported that more younger surgeons than older surgeons preferred ORIF for treatment of DRFs and suggested that the training environment may be the cause for the discrepancy. The present study found that ORIF accounted for 91% of surgery for DRFs in tertiary hospitals, which play an important role in orthopaedic training. It is therefore to be expected that younger surgeons in Korea will be more likely to be familiar with ORIF, and that its popularity will continue to increase in the future.
Clinics (45%) were found to account for largest proportion of the management for DRFs in Korea. Approximately 90% of treatment in clinics was conservative, which may be due to differences in fracture severity or the availability for surgical treatment. Many small clinics are not equipped to perform surgical procedures, and cases with intra-articular or unstable DRFs are transferred to larger healthcare institutions. As such, these clinics are likely to treat more patients with DRFs for whom conservative treatment is possible. The available equipment is also thought to have an impact on the type of surgery being performed for DRFs. More specifically, the high proportion of percutaneous pinning used in clinics may be because the procedure requires relatively simple instruments. On the other hand, in other types of healthcare institutions, which typically have a better environment for providing surgical care, the proportion of surgical treatment was higher than that of conservative treatment, and ORIF accounted for the majority of surgeries.
However, hospitals with 30–100 beds and general hospitals had a higher rate of external fixation than tertiary hospitals. External fixation is indicated for severe comminuted intra-articular DRFs or combined complex carpal dislocation (25). Although patients with severe injury are more likely to be transferred to advanced healthcare institutions, interestingly, tertiary hospitals (3.1%) had a lower rate of external fixation than hospitals with 30–100 beds (21.3%) and general hospitals (23.3%) did. The proportion of external fixation among all surgeries in the U.S. during 1996–2005 was 7.9% (12). Even compared to this, hospitals with 30–100 beds and general hospitals in Korea had a higher rate of external fixation among surgeries overall. It is difficult to pinpoint the exact reason for this phenomenon. It is possible that it may be ascribed to medical environment. The fee of operation in Korean medical insurance system is set low, so this may have influenced the decision in choosing the surgical method. As of 2017, the price of external fixation is valued higher than that of the plates in Korea, making the former more profitable for the hospital management, taking into account the reimbursements. Along with these economic aspects, it is highly likely that a surgeon's preference is related to the high usage of external fixation (7).
Even though this study employed a large sample size, based on a nationwide database, it also has some limitations. First, HIRA data provided no information on outcomes, the popularity of this mode of treatment does not necessarily indicate its superiority. Second, primary surgery and reoperations could not be distinguished in the coding system. As such, when 2 operation codes were entered for a single patient, it was assumed that the second operation code was entered for the opposite side, rather than for reoperation. With this method, reoperation cases may have been categorized as primary surgery cases, and thus the number of primary surgery cases may have been overestimated. Finally, there is a possibility of some code errors in a large database.
The present study indicated that the proportion of DRF cases receiving surgical treatment is steadily increasing in Korea, and the proportion undergoing ORIF, in particular, is rapidly increasing. There was a difference in the component ratio of the operation codes according to healthcare institution type. ORIF was the most popular procedure in tertiary hospitals, while percutaneous pinning was most popular in clinics. In addition, general hospitals and hospitals with 30–100 beds had a higher proportion of external fixation than tertiary hospitals and clinics did.
 XML Download
XML Download