

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Guillain-Barré syndrome (GBS) is an acute or subacute peripheral polyneuropathy, which is accompanied by symmetric flaccid paralysis of the extremities, sensory abnormalities, and cranial nerve palsy. Although the pathogenesis of the GBS has not been clearly elucidated, recent immunological evidence has supported a mechanism of autoimmune damage (1). Interest in the risk of GBS after vaccination increased after approximately 500 cases of GBS were reported after the mass administration of the A/New Jersey/76 vaccine during the swine flu epidemic in the United States in 1976 (23). In Korea, there have been a few reports of GBS cases after influenza vaccination (4) and large-scale influenza vaccination was performed as reports of a new strain of the influenza virus (H1N1v) began emerging worldwide. This renewed the focus on adverse events following immunizations (AEFIs) (56).
Although GBS is the most common severe AEFI in adults (78), it is difficult to accurately diagnose at an early stage because of its diverse causes and clinical presentations. Despite the usefulness of supporting tests, such as cerebrospinal fluid (CSF) analysis and electrophysiology, there are currently no specific testing methods for diagnosing GBS. In an effort to produce a standardized reporting format, the Brighton criteria are currently being used worldwide to assess GBS cases following immunization. Based on these criteria, a multicenter cohort study investigating the clinical symptoms and laboratory findings required for diagnosis has recently been published (9).
Although there have also been similar local studies (10), additional research focused on the specific clinical and laboratory characteristics of patients with post-vaccination GBS are still necessary. Therefore, this study aimed to evaluate the results of clinical and laboratory features of cases of GBS that developed following immunization.
MATERIALS AND METHODS
Data source
As a part of the National Immunization Program (NIP), the Advisory Committee Vaccination Injury Compensation (ACVIC) has been operating since 1995 to provide compensation for AEFI (11) in Korea. The present study was a retrospective review of additional epidemiological investigations for the expert committee between 2002 and 2014. Among the 590 requests for evaluation of vaccination-related compensation during this period, 68 cases were related to GBS. From these cases, we analyzed the 48 cases that were ultimately approved for compensation.
Evaluation
Demographic characteristics such as age and sex, underlying diseases, previous infection status, as well as CSF, nerve conduction studies (NCSs), and magnetic resonance imaging (MRI) test results, treatment methods, and prognosis, were verified using the epidemiological data collected for the vaccination compensation committee. Neurological test findings included motor weakness, sensory symptoms, cranial nerve involvement, ataxia, deep tendon reflex (DTR), autonomic dysfunction, and mechanical ventilation were analyzed at the first hospital visit (entry) and when clinical symptoms were most severe (nadir). Motor weakness was assessed based on the GBS disability score (GDS), and the time of the highest score on GDS was defined as the nadir.
The date of symptom presentation was defined as the time at which motor weakness in the extremities or cranial-nerve-innervated muscle occurred, or sensory abnormalities presented bilaterally. On this basis, the time from vaccination to the onset of symptoms, time from the onset of symptoms to nadir, the time from nadir to the start of recovery, and the time from the onset of symptoms to the first CSF and NCS, were all measured in days. The time of start of recovery refers to the time when motor weakness improvement or GDS score changes were first detected. Cases were divided into 2 groups according to age; young age group (≤ 19 years) and adult group (≥ 20 years). Outcome at discharge was classified into 3 status: full recovery, recovered with neurologic sequelae, and death according to whether accompanied by neurological symptoms.
Results of the NCS were classified as normal and abnormal. And abnormal NCS parameters were analyzed. Cases where CSF and NCS results could not be verified were treated as cases with missing values. All cases were classified for certainty of diagnosis from level 1 to 4, according to the Brighton criteria (9).
Definition of various parameters
A definition of various parameters was presented. 1) Brighton criteria: patients were classified between level 1 (highest certainty of diagnosis) and 4 (lowest certainty of diagnosis) according to 7 criteria; bilateral flaccid paralysis of the extremities, abnormal DTR in extremities with paralysis, monophasic progression within 12 hours to 28 days of symptoms, < 50 cells/µL on CSF analysis, abnormally high protein concentration in CSF, subtype consistent with GBS on NCS, and a lack of other causes for weakness (9). We regarded Brighton criteria level 1–3 as high diagnostic certainty of GBS. 2) Autonomic dysfunction: cases with autonomic dysfunction presented with cardiac arrhythmia, fluctuation in blood pressure, urinary retention, sexual dysfunction, impaired sweating, abnormal pupillary reflex, and gastrointestinal dysfunctions such as diarrhea, constipation, and intestinal obstruction (1). 3) Respiratory or cranial-nerve-innervated muscle weakness: patients with findings of facial paralysis, oropharyngeal paralysis, extraocular muscle palsy, or breathing impairments were classified as having cranial nerve abnormalities (12). 4) Albuminocytologic dissociation: albuminocytologic dissociation refers to increased protein concentration (> 50 mg/dL) in the CSF without pleocytosis (< 50 cells/µL) (9), and is a useful CSF finding for the diagnosis of GBS. This is known to reflect widespread inflammation of the nerve roots.
Statistical analysis
Statistical analysis was performed using SPSS statistics software, version 19.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were presented as percentages, and continuous variables were presented as the mean and standard deviation (SD), or as the median and interquartile range (IQR) when they did not follow a normal distribution. The Mann-Whitney test and the χ2 test or Fisher's exact test for non-normal distributions were used to compare the size of continuous variables and the distribution of categorical variables between groups, respectively. A logistic regression analysis was used to verify the odds ratios (ORs) for categorical variables. Two-tailed tests were used and a P value < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
Basic characteristics are displayed in Table 1. All the GBS cases had a history of influenza vaccination with either monovalent (n = 35) or trivalent (n = 13) and no other vaccination was the cause of GBS. Among the 48 cases, 30 (62.5%) fulfilled Brighton criteria level 1–3.
Table 1
Description of GBS cases following vaccination in Korea (n = 48)

GBS = Guillain-Barré syndrome, IQR = interquartile range, GI = gastrointestinal, CSF = cerebrospinal fluid, NCS = nerve conduction study, MRI = magnetic resonance imaging, IVIG = intravenous immunoglobulin, PE = plasma exchange.
*Includes asthma, tuberculosis, and angina.
![]()
Clinical progress
The times from vaccination to onset of symptoms are shown in Fig. 1. Of the total 48 cases, 47 (97.9%) developed symptoms within 3 weeks, and in particular, more than half (54.2%) within 2 days.
 | Fig. 1The relationship between the number of GBS cases and the interval between vaccination and the onset of symptoms. Majority (97.9%) of cases developed symptoms within 3 weeks after vaccination. Particularly, more than half of cases (54.2%) occurred were within 2 days after vaccination.
GBS = Guillain-Barré syndrome.
|
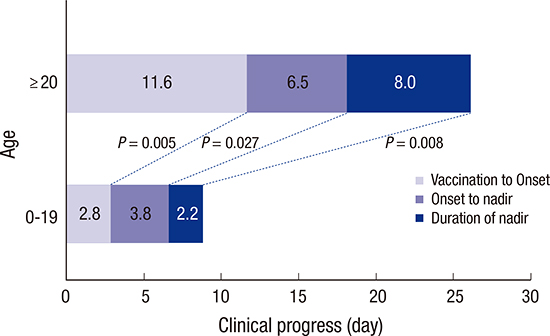
The time from onset of symptoms to nadir was 3 days (IQR, 2–7 days), from nadir to start of recovery was 2 days (IQR, 1–5 days), and the total duration of admission was 14 days (IQR, 6–33 days). Comparing clinical progression between the 0–19 years old group (n = 32) and the ≥ 20 years old group (n = 16), there was a significant difference between the groups for time from vaccination to onset of symptoms (0–19 years: 1 day, IQR, 1–3 days; ≥ 20 years: 10 days, IQR, 3–15 days; P < 0.001), time from onset of symptoms to nadir (0–19 years: 2 days, IQR, 1–6 days; ≥ 20 years: 5 days, IQR, 3–8 days; P = 0.014), time from nadir to start of recovery (0–19 years: 1 day, IQR, 1–3 days; ≥ 20 years: 7 days, IQR, 3–10 days; P < 0.001), and for the total duration of admission (0–19 years: 9 days, IQR, 6–14 days; ≥ 20 years: 45 days, IQR, 33–93 days; P < 0.001) (Fig. 2).
Clinical features
The neurological symptom patterns were analyzed at both the entry and nadir time points (Table 2). 1) Motor system: at entry of hospital, weakness in bilateral lower limbs were the most frequent motor symptom and 21 patients (43.8%) were unable to walk 10 m without help (GDS, 3–6). At nadir, all 4 limbs weakness were the most frequent motor deficit and 36 patients (75.0%) were GDS 3–6. 2) Sensory system: pain was more common problem than sensory deficit. 3) Respiratory or cranial-nerve-innervated muscle weakness: patients who showed symptoms of cranial nerve palsy at entry were more likely to have severe deficit (GDS, 3–6) at nadir (OR, 1.50; 95% confidence interval [CI], 1.19–1.89; P = 0.023). 4) Autonomic dysfunction: at entry, 3 patients (6.3%) showed autonomic disturbance and at the nadir, 10 patients (20.8%) had autonomic dysfunction. Those with autonomic problem also more likely to be have severe deficit at nadir (OR, 1.39; 95% CI, 1.13–1.70; P = 0.048). 5) DTR: although the majority of cases showed decreased or absent DTR, 33.3% of patients had preserved DTR even at nadir.
Table 2
Comparison of the clinical features of study patients at hospital entry and at nadir (n = 48)

Values are presented as number (%).
GDS = Guillain-Barré syndrome disability score, DTR = deep tendon reflex, BP = blood pressure, HR = heart rate, GI = gastrointestinal.
![]()
Laboratory features
Missing values were excluded from the analysis of the CSF and NCS (Table 3). 1) CSF: the time from onset of symptoms to lumbar puncture was 3 days (IQR, 1–6 days) and 11 of these patients demonstrated albuminocytologic dissociation. Increase in CSF protein concentration was associated with the time from onset of symptoms to testing. Only less than 20% of patients who were tested within 3 days showed increased protein concentration, while 75% of patients who were tested after 8–14 days showed increased protein concentrations (Fig. 3). 2) Electrophysiological study: NCS was performed in 42 patients (87.5%) and 32 patients were available for raw data analysis (Table 3). The median time from onset of symptoms to testing was 4 days (IQR, 2–7 days). Blink reflex test showed abnormal response on 3 out of 4 cases. On average, NCS was performed 1.4 times and the results of NCS were related to the time from the onset of symptoms to testing. Among patients who were tested within 7 days of onset of symptoms, 44.1% (15/34) revealed polyneuropathy pattern. Among patients who were tested within 8–14 days, 85.8% (6/7) showed abnormal findings.
Table 3
Results of GBS diagnostic studies

GBS = Guillain-Barré syndrome, CSF = cerebrospinal fluid, WBC = white blood cell, IQR = interquartile range, NCS = nerve conduction study, MNCV = motor nerve conduction velocity, CMAP = compound muscle action potential, SNCV = sensory nerve conduction velocity, SNAP = sensory nerve action potential, MRI = magnetic resonance imaging.
![]()
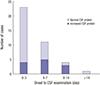 | Fig. 3The number of cases and percentages with elevated protein concentration in CSF analysis and the timing of lumbar puncture after symptom onset. During the first week, most of CSF examinations were performed (86.8%) but albuminocytologic dissociation was found in less than 20%. In the second week, positive rate of albuminocytologic dissociation increased up to 75%.
CSF = cerebrospinal fluid.
|
DISCUSSION
The present study analyzed the clinical and laboratory characteristics of 48 cases of GBS that occurred after immunization between 2002 and 2014. Each case was selected based on the data of experts meeting for compensation of vaccination, ACVIC in Korea. Although some cases did not fulfill the Brighton criteria level 1–3, we regarded these cases as possible GBS because they were also reviewed thoroughly and concluded having GBS by experts meeting.
In this study, majority of the patients (66.7%) were under 20 years old, and this is believed to be the direct result of the mass immunization in schools in response to the influenza virus (H1N1v) epidemic in 2009. In almost all cases, GBS developed within 3 weeks of immunization and it is consistent with previous reports (13). Each stage of clinical progression such as the interval from onset to nadir, nadir to recovery and time of stay in hospital were relatively brief compared to previous study of GBS, particularly in young age group. Age is an important prognostic factor (1) and younger population of this study should affect the shorter duration of each stage. Although recent report of the pediatric GBS compared to adult group showed the shorter interval from onset to nadir (6.3 vs. 7.3 days) (14), it would be more rapid course in young age group with post-vaccination GBS. In GBS, the severity is often estimated with walking ability and need for ventilator support. At the nadir, 75% of patients could not walk and 19.4% needed ventilator support and none of them died with GBS related problem. Severity at nadir is quite similar results to large scale GBS studies without vaccination (1516). So, in this study, post-vaccination GBS would have rapid clinical progression with similar severity at nadir. Bilateral leg weakness was the most common early motor symptom and pain was the most common non-motor symptom (17).
In addition to influenza vaccines, cases of GBS have been reported after immunization with various vaccines, including measles, mumps, and rubella (MMR), hepatitis B, diphtheria, tetanus, and pertussis (DTP) and polio (1819). Nevertheless, no causal relationship between the MMR vaccine and GBS has been reported (202122). In Korea, there are still no reports linking GBS to vaccines other than those for influenza (4), and the results of the present study showed that all cases were associated with influenza immunizations. Local immunization clinics usually use the trivalent seasonal influenza vaccine recommended by the World Health Organization (WHO). In 2009, additional mass vaccination was performed using the A/California/7/2009 (H1N1)-like virus monovalent vaccine in response to the new influenza epidemic. According to a recent meta-analysis, the monovalent influenza vaccine was more strongly associated with GBS compared the trivalent influenza vaccine (3). The present study also found that 83.3% of the total GBS cases were associated with the monovalent influenza vaccine. However, a domestic study comparing GBS incidence before and after widespread vaccination with the monovalent vaccine in 2009 did not demonstrate a significant increase in incidence (23). Therefore, there is room for debate about the relative risks of the monovalent and the trivalent vaccines. Because this study was based on assessment data for compensation for AEFI, it is difficult to ascertain the full incidence of GBS for the various individual vaccines. However, from 2002 to 2014, 48 compensation applications were received, and previous infection could not be excluded as a causative factor in 5 cases (10.4%). Additionally, 18 cases (37.5%) were classified as Brighton criteria level 4, which is the lowest level of certainty in GBS diagnosis. This suggests a very low incidence for vaccine-related GBS.
The most important study in the diagnosis of GBS is NCS. It often shows no or only subtle abnormality in the very early stage of GBS (24) and NCS findings tend to change according to GBS progression (9). Furthermore, to verify the subtype of GBS such as acute motor axonal neuropathy (AMAN) and acute inflammatory demyelinating polyneuropathy (AIDP), the follow-up NCS with proper interval is needed. In our study, most NCS study was performed within the first week of disease and in only less than half, follow-up NCS was done. Furthermore, NCS could not be done in a unified manner across institutions. For the proper study of post-vaccination GBS, standardized protocol for minimum requirements of NCS parameter and study schedule with follow-up is needed.
Most previous study with post-vaccination GBS focused on the incidence and prevalence. However, subtypes of GBS after immunization are not well characterized. Subtypes in this study included axonal type as well as demyelinating type and this finding suggests heterogeneous pathogenesis although after exposure to the same causative triggering factor.
The main reasons for the level 4 in Brighton criteria were test results (i.e., CSF testing, NCS, and DTR) that were not compatible with diagnosis of GBS, or insufficient testing data. Comparing Brighton criteria level 1–3 groups and level 4 group, we did not find significant differences in the entire clinical course, including the time from immunization to symptoms, symptoms to the nadir, as well as the time from the nadir to the start of recovery, and total length of stay (P > 0.05). However, there were more patients who were unable to walk unassisted at the nadir in the level 1–3 groups, signifying a GDS score of 3–6 (P = 0.036). The certainty of diagnosis according to Brighton criteria can decrease due to insufficient testing data or missing values. Therefore, in order to evaluate GBS following immunization, complete treatment and testing results need to be obtained.
The Brighton criteria are used worldwide for the evaluation of GBS following immunization. In order to increase diagnostic accuracy when symptoms develop within 6 weeks of immunization and in the absence of alternative diagnoses to explain the symptoms and clear causative factors such as previous infection, vaccine-related GBS should be suspected. Detailed tests should be subsequently performed to aid early diagnosis. Due to the nature of NCS and CSF tests, follow-up testing need to be performed 1–2 weeks after the presentation of symptoms.
 XML Download
XML Download