

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Allergen-specific immunotherapy (AIT) is the only method capable of altering the natural courses of allergic diseases. Compared with pharmacologic agents that merely offer symptomatic relief, AIT has been found to be effective in preventing sensitization to new allergens, in reducing the risk for developing asthma, and in maintaining its therapeutic effects upon treatment completion (12). In numerous studies, AIT was proven to significantly decrease symptoms and medication, and improve bronchial hyperreactivity since its introduction as a treatment for allergic asthma (AA) (3).
Subcutaneous immunotherapy (SCIT) has been shown to offer greater efficacy, although with a higher incidence of systemic adverse reactions, compared to sublingual immunotherapy (45). Several studies to enhance the therapeutic effects of SCIT and reduce its potential for side effects are, however, underway: improved safety and efficacy have been reported with additional use of omalizumab or toll-like receptor agonists and with modification of allergen extracts (6).
The clinical outcomes of AIT can differ from patient-to-patient according to their ethnicity, climate, and especially, major allergens of their residing area. However, biomarkers and clinical parameters predictive of clinical responses to AIT are lacking. Therefore, in a retrospective cohort covering 12 years, we sought to investigate the clinical outcomes and prognostic factors of SCIT in Korean adults with AA.
Go to : 
MATERIALS AND METHODS
Subjects
The retrospective cohort analyzed in the present study comprised 627 patients who received SCIT between 2000 and 2012 at Ajou University Hospital upon receiving a diagnosis of AA with or without allergic rhinitis (AR). Patients were diagnosed with AA according to clinical symptoms of coughing, wheezing, chest tightness, dyspnea, airway hyperreactivity (PC20 ≤ 25 mg/mL of methacholine), or airway reversibility defined as increases in forced expiratory volume in the first second (FEV1) of ≥ 12% and ≥ 200 mL from pre-bronchodilator use. All patients showed positivity to at least one inhalant allergen (Allergopharma, Reinbek, Germany) during a skin prick test (SPT) as follows: house dust mites (HDMs) (Dermatophagoides pteronyssinus [D1] and Dermatophagoides farinae [D2]), tree pollens (Alder, Birch, Hazel, Beech, Ash, and Oak), grass pollens (Orchard, Rye, Bermuda, Timothy, Kentucky, and Meadow), and weed pollens (Ragweed and Mugwort). Positivity to any allergen on SPT was identified via allergen-induced wheals with a mean diameter the same or larger than the diameter of histamine-induced wheals. For patients lacking SPT results, serum-specific immunoglobulin E (IgE) levels to allergens at baseline higher than 0.35 kU/L were deemed indicative of allergen sensitivity. We excluded patients with positive SPTs to animal dander or mold without sensitization to HDM or pollen. Also, total IgE and specific IgE levels to the allergens were measured using the ImmunoCAP system (Thermo-Fisher, Uppsala, Sweden).
In all patients, we reviewed medical records on drug prescriptions, the presence of exacerbation, adverse events (AEs) during immunotherapy, and results of lung function test and serum total IgE levels over the treatment period.
Immunotherapy
All patients underwent SCIT with Novo-Helisen Depot® (Allergopharma) in which allergen extract is adsorbed to aluminum hydroxide. The SCIT treatment period was divided into 2 phases: an initial build-up phase and a maintenance phase. The modes of immunotherapy were classified as conventional and rush immunotherapies. For conventional SCIT, patients received subcutaneous injections of gradually increasing doses of allergen extract every week for 12 weeks, followed by once-a-month maintenance doses. For rush SCIT, allergen extract was administered at increasing doses every 2 hours for 3 consecutive days, followed by maintenance doses every month (7). All patients on rush SCIT had been taking premedications such as antihistamines and/or leukotriene receptor antagonists (LTRAs) for at least 1 week before starting immunotherapy and during the accelerating phase. Because we excluded patients who had positive to animal dander and/or molds on SPT or specific IgE tests without sensitization to HDM or pollen, SCIT for the study subjects were divided into HDM only, pollens only, and mixed groups in the present study.
Evaluation of clinical outcomes
Clinical responses were examined at one-year intervals. We classified clinical responses to SCIT into 3 categories: 1) Remission was defined as no further requirement of maintenance medication (e.g., inhaled corticosteroids [ICSs] or LTRA for AA and intranasal corticosteroids or non-sedating antihistamines for AR), as well as no complaint of symptoms relating to asthma in medical chart for at least 1 year, or as a negative response to a methacholine challenge (> 25 mg/mL) (89); 2) A controlled state was defined as patients whose symptoms were controlled well with maintenance treatment and required no further rescue medication, such as that with oral corticosteroids and short acting beta agonist for last 1 year of SCIT; 3) An uncontrolled state was defined as patients with poorly controlled symptoms with maintenance treatment alone, requiring oral corticosteroids and/or antibiotics more than once a year to control allergic symptoms. AEs associated with SCIT were recorded upon spontaneous reports from patients, as well as through objective observations by physicians. This aspect was investigated based on clinical history at each injection visit. Systemic adverse reactions in the patient record were graded according to the grading system proposed by the World Allergy Organization (10). A single simultaneous occurrence of a local and systemic AE was considered as individual local and systemic AEs. And if different grade of systemic side effects occurred, for example, generalized pruritus and asthma, more severe grade were described.
Statistical analysis
Simple cross-tabulations and descriptive statistics for the clinical characteristics of the study subjects were examined using χ2 and t-tests. Rates of remission, controlled, and uncontrolled states over time were determined by means of life tables and extension of survival analysis. The effect of individual predictor variables, such as mode of immunotherapy, target allergens, comorbidities, and the occurrence of AEs, on time to remission was analyzed by univariate and multivariate Cox proportional hazards regression models, accommodating for both continuous and binary variables. Hazard ratios (HRs) are presented with 95% confidence intervals (CIs). A generalized estimating equation was used to analyze temporal correlations between total IgE and specific IgE levels to HDM according to SCIT outcomes. All statistical analyses were performed with SPSS software, version 22.0 (IBM Corp., Armonk, NY, USA). P values less than 0.05 were considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board of Ajou University (AJIRB-MED-MDB-15-449). Informed consent was not required by the board due to retrospective study nature.
Go to :
RESULTS
Study subjects
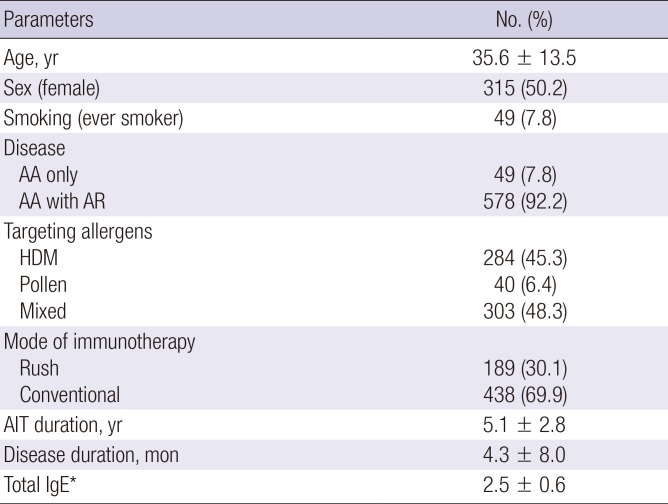
Among the 627 enrolled patients, 578 (92.2%) had both AA and AR, and 49 (7.8%) had been suffering from only AA. Overall, 284 (45.3%) received SCIT for HDM, 40 (6.4%) for pollens, and 303 (48.3%) for mixed allergens (at least one pollen with HDM). Rush SCIT was administered to 189 (30.1%) patients, whereas the other 438 (69.9%) patients received conventional SCIT. Target allergens and modes of immunotherapy are shown in Table 1 and Fig. 1 in more detail. The mean age of the AA group was 35.6 ± 13.5 years, with 49.8% being male. The mean duration of immunotherapy for AA was 5.1 ± 2.8 years.
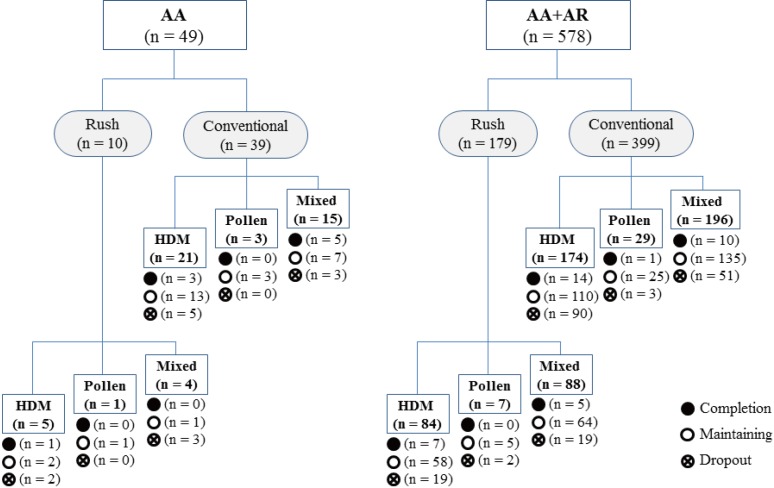 | Fig. 1Target allergen and treatment status for each patient group.
AA = allergic asthma, AR = allergic rhinitis, HDM = house dust mite.
|
Table 1
Baseline characteristics and clinical outcomes among the study subjects (n = 627)
Values given are the mean ± standard deviation or number (%).
AA = allergic asthma, AR = allergic rhinitis, HDM = house dust mite, AIT = allergen-specific immunotherapy, IgE = immunoglobulin E.
*Geometric mean after logarithmic transformation.
![]()
A total of 203 patients (32.4%) dropped out from SCIT: 149 (73.4%) quit immunotherapy arbitrarily without giving a reason. The others reported inconvenience with the time-consuming treatment (34, 16.7%), being transferred to another hospital (12, 5.9%), other disease treatment or pregnancy (7, 3.4%), and severe AEs (1, 0.5%) as reasons for quitting SCIT.
Efficacy and safety of immunotherapy
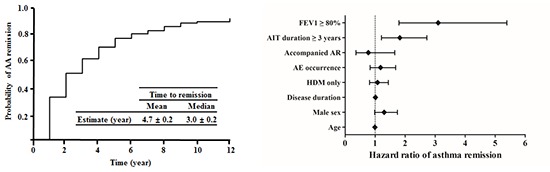
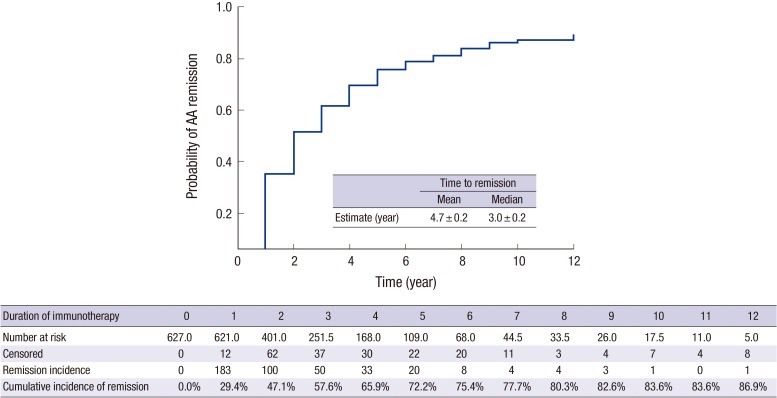
After 12 years, the cumulative incidence of clinical remission from AA was 86.9% (Fig. 2). In patients with AA, 29.5% achieved remission after the 1st year of SCIT, and the cumulative incidence of AA remission continuously increased to 72.2% in the 5th year. As we evaluated the efficacy outcomes only for the 46 patients who completed SCIT during the study period, 37 (80.4%) achieved asthma remission, 7 (15.2%) had controlled asthma, and 2 (4.3%) had uncontrolled asthma. However, we need further studies to follow-up the patients to evaluate whether their asthma is relapsed or maintained remission. The mean duration of SCIT until remission from AA was 4.7 ± 0.2 years, with a median of 3 years.
AEs were recorded in 128 patients (20.4%) in the AA. Most AEs (98.4%) occurred during the build-up phase. Of the 438 patients who underwent conventional immunotherapy, 50 (11.4%) had AEs, a significantly smaller proportion than the 78 of 189 (41.3%) individuals who underwent rush immunotherapy (P < 0.001). Among all patients in this study, local AEs occurred in 99 (15.8%), and systemic AEs occurred in 109 (17.4%). The severities of the systemic AEs reached grade I in 89 (14.2%), grade II in 19 (3.0%), and grade IV in another one patients (0.2%). No patient died from an immunotherapy-related AE.
To demonstrate as a predictive biomarker, baseline total IgE and specific IgE to D1 and D2 were investigated in 284 patients received SCIT with HDM only. Total serum IgE levels at the beginning of SCIT were increased in those achieving remission than those that did not, although the difference was not statistically significant (910.5 vs. 720.7 kU/L, P = 0.274). We discovered significantly higher levels for specific IgE to D1 in remission group than non-remission group (32.2 vs. 22.5 kU/L, P = 0.017). Also, specific IgE to D2 was significantly higher in remission group (43.6 vs. 33.2 kU/L, P = 0.031). However, these significance disappeared after adjusting age and sex in D1 (P = 0.215) and D2 (P = 0.492). Specific IgE to D1/total IgE and specific IgE to D2/total IgE ratio were not different in both groups.
Predictors of clinical responses to SCIT
Analyzing clinical parameters related to remission from AA, we found mode of immunotherapy, history of smoking, target allergen, specific IgE to HDM, occurrence of AE, and presence of AR to have no influence on either asthma remission or the duration of immunotherapy until remission (Table 2). A significant increase in remission rate and shorter periods of immunotherapy were recorded patients with high baseline FEV1 (≥ 80%), compared to patients with lower FEV1 (< 80%) (69.3% vs. 34.9%, 4.2 ± 0.2 vs. 7.9 ± 0.6 years, P < 0.001). Also, a higher remission rate was achieved in patients who underwent immunotherapy for more than 3 years than those who underwent immunotherapy for less than 3 years (71.5% vs. 35.7%, P = 0.047). Multivariate Cox regression analysis revealed that remission rate was shown to be positively associated with a predicted FEV1 at baseline ≥ 80% (HR, 3.10; 95% CI, 1.79–5.39; P < 0.001) and receiving immunotherapy for more than 3 years (HR, 1.82; 95% CI, 1.21–2.72; P = 0.004). Remission rates in AA patients were not found to be associated with sensitization to HDM or pollens (Table 3).
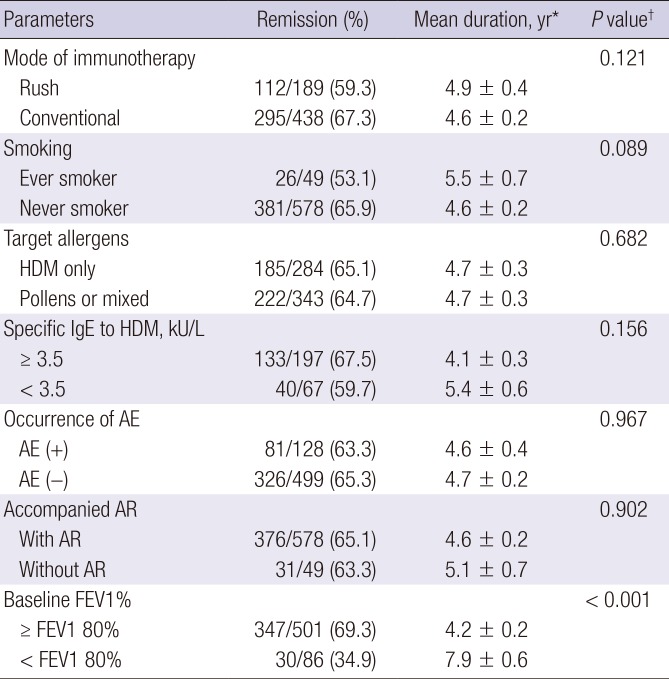
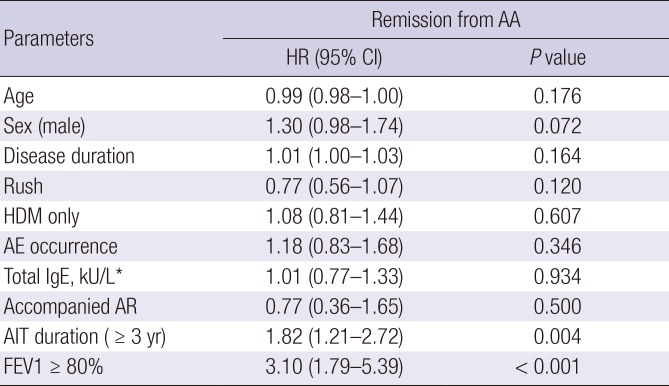
Table 2
Difference in the proportion of patients who achieved remission and mean durations until remission
HDM = house dust mite, IgE = immunoglobulin E, AE = adverse event, AR = allergic rhinitis, FEV1 = forced expiratory volume in the first second.
*Values given are the mean ± standard deviation; †P value was calculated by using Kaplan-Meier method.
![]()
Table 3
Cox regression models for predicting asthma remission during AIT
AA = allergic asthma, HR = hazard ratio, CI = confidence interval, HDM = house dust mite, AE = adverse event, IgE = immunoglobulin E, AR = allergic rhinitis, AIT = allergen-specific immunotherapy, FEV1 = forced expiratory volume in the first second.
*Geometric mean after logarithmic transformation.
![]()
To identify determinants of poor outcomes during AIT, subgroup analyses of 512 AA patients who underwent SCIT for at least 3 years were performed. Among them, 366 (71.5%) achieved remission, and 100 (19.5%) of them reached at a well-controlled state. Only 46 (9.0%) patients suffered from uncontrolled asthma after undergoing SCIT for more than 3 years. Female sex (odds ratio [OR], 4.14; 95% CI, 1.56–10.98; P = 0.004), FEV1 less than 80% (OR, 4.44; 95% CI, 1.81–10.94; P = 0.001) were significant determinants of uncontrolled asthma in the subgroup analysis of AA patients.
Comparison between SCIT with a single allergen (HDM only) or multiple allergens for multi-sensitized subjects
Multi-sensitization was defined as sensitivity to both HDM and at least one pollen allergen. Of 141 AA patients who were sensitized to both HDM and any pollen, 59 underwent SCIT with HDM alone, while the other 82 patients underwent SCIT with multiple allergens. There was no significant difference in the mean duration to achieve asthma remission between patients who underwent SCIT with HDM only (mean ± standard error [SE], 5.08 ± 0.70 years) and those using multiple allergens (mean ± SE, 4.5 ± 0.5 years; P = 0.750).
Go to :
DISCUSSION
In our retrospective cohort, SCIT with aluminum hydroxide adsorbed allergen extract facilitated remission in 86.9% of patients with AA within 4.7 years on average. During SCIT, baseline FEV1 ≥ 80%, and maintenance of immunotherapy for more than 3 years were highlighted as significant predictors of asthma remission. We could not find baseline specific IgE to D1 and D2 to be a predictor for better response of immunotherapy in patients with AA on SCIT with HDM alone. Finally, in multi-sensitized patients, SCIT with multiple allergens and SCIT with HDM alone revealed not different clinical results. Considering that approximately 20%–30% of adults with asthma went into remission over a period of 20 years in previous prospective studies (89), 86.9% of the cumulative incidence of asthma remission in the present study result was remarkable.
Researchers have yet to agree upon the optimum period for administering immunotherapy. Most clinical trials to evaluate the efficacy of AIT have had a treatment period of approximately 1 to 2 years (11). However, immunotherapy for less than 2 years has been shown to increase recurrence rates after stopping immunotherapy (12). Further, while one study reported 3 years of AIT to be effective (13), another showed higher efficacy with AIT for 5 years (14). The average maintenance period until remission in the present study was 5.1 years, suggesting that approximately 5 years of AIT is warranted in patients with AA. Nevertheless, as the endotype, phenotype, and severity of allergic diseases differ for each patient, there may not be a single optimal duration for immunotherapy. In this regard, we found female sex, and shorter period of immunotherapy to be significantly associated with uncontrolled disease at the survey of AIT for AA patients. Given the confirmed cost saving effects of AIT, we recommend immunotherapy more than 3 years, up to 5 years.
Specific biologic markers to predict the effectiveness of immunotherapy have been investigated. In in vivo SPT, a decreased reactivity to allergens is observed after immunotherapy (15). However, the role of SPT results as predictors of immunotherapy effectiveness is limited by the relatively late appearance of reduced reactivity in SPTs. Meanwhile, a study on SCIT has shown that patients with a higher ratio of specific IgE to total IgE exhibit better clinical responses (16), whereas those with lower ratio were more effective in sublingual immunotherapy study (17).
Other studies in children and adults have also described significantly higher baseline levels of specific IgE to pollens or HDM in treatment responders than in non-responders (161819). Although we also found a tendency of increased specific IgE levels to HDM in individuals achieving remission, however, no statistically significant difference in those levels was observed after adjusting age and sex of the study population. While other studies on AIT for treating rhinitis alone and mainly on younger patients, but, patients enrolled into the present study were older than others and most of patients having both AA and AR. Thus, further validation is needed for determining clinical utility of the baseline specific IgE to HDM as a predictor of effective immunotherapy in adult AA patients.
Previous studies have been unable to clarify whether single allergen immunotherapy is as effective as AIT targeting multiple allergens in multi-sensitized patients with respiratory allergic diseases. Data reported in a study from the US favored multi-allergen AIT, while data from European countries supported the use of a single allergen (20). In multi-sensitized patients, we could not find superiority between single allergen immunotherapy for HDM and multi-allergen immunotherapy for HDM and pollens. Given that lack of information about multi-allergen immunotherapy including HDM, following study is needed to confirm which type of immunotherapy is more effective.
Comparable to other studies, systemic AEs in the present study occurred in 20.4% of AA patients (21). Almost all systemic AEs occurred in the build-up phase as in previous reports (2122). So once patients reached the maintenance phase, they would be considered to be safe for the following maintenance immunotherapy. Additionally, most of the systemic AEs were deemed grades I and II, and were not life threatening. Santos et al. (23) showed similar results in which 46% of systemic AEs were grade I and 54% were grade II. Finally, we found that patients who underwent rush immunotherapy suffered from AEs more frequently than those who underwent conventional immunotherapy. In our cohort, anti-histamines and LTRA have been found to be insufficient for reduction in the development of AEs for the patients who got a rush mode of SCIT to the levels of conventional mode of AIT. Premedication with systemic steroid and/or anti-IgE treatment prior to initiating rush immunotherapy, however, could potentially reduce the occurrence of serious AEs to the same levels as those in conventional immunotherapy (24).
The present study has several limitations. In our retrospective cohort analysis, lack of a control group that did not receive SCIT made it difficult to estimate the true effectiveness of AIT. And relatively high proportion of patients dropped out of immunotherapy with several reasons. The present study, nonetheless, also has some merit in that clinical outcomes (remission and control states) were applied as primary endpoints in a relatively large population. Also, the study covers maintenance durations of up 12 years in patients from a single institution.
In conclusion, this large retrospective cohort expands on previous results by demonstrating that AIT facilitates remission in 86.9% of adult AA patients with rare serious AEs. Also, a mean AIT duration of 3 years or more and initial FEV1 (≥ 80%) seemed to increase remission rates in Korean patients with AA.
Go to :
 XML Download
XML Download