

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Helminthiases are distributed globally. Korea was a heavily endemic country of intestinal helminthiases but most had been nearly eliminated (1). However, clonorchiasis and some kinds of intestinal trematodiasis remain endemic now (2). Clonorchiasis and other tissue-invading helminthiases are targets of differential diagnosis for patients with suggestive clinical symptoms or signs of related diseases. The tissue-invading helminthiases such as paragonimiasis, cysticercosis, and sparganosis have been regarded with clonorchiasis as major problems in Korea among the people who enjoy eating raw or pickled fish, crab, meat, or others (3).
Absolutely, demonstration of worms, larvae, or eggs of certain helminths can make a precise diagnosis, but it is not sensitive, and sometimes impossible for tissue-invading helminths. Moreover, the method to recover worms or larvae from the tissue is invasive. Given these problems, serodiagnosis was developed for tissue helminthiases (456789). For serodiagnosis, enzyme-linked immunosorbent assay (ELISA) is simple and sensitive enough to detect specific antibodies to parasite antigens (10). The ELISA was developed as multi-antigen screening because of frequent cross-reactions between helminthiases.
This study reviewed the ELISA results and clinical records of traceable subjects in our serodiagnosis laboratory to monitor positive status and its significance of clonorchiasis, paragonimiasis, cysticercosis, and sparganosis in Korea.
Go to : 
MATERIALS AND METHODS
Human serum samples and ELISA data
A total of 6,017 serum samples were requested for serodiagnosis by multi-antigen ELISA in the Institute of Endemic Diseases, Seoul National University, Seoul, Korea from 1996 to 2006. Physicians or surgeons of Seoul National University Hospital, Seoul National University Bundang Hospital, Seoul National University Boramae Medical Center, and Seoul National University Hospital Healthcare System Gangnam Center requested the serology test to confirm or differentiate suspected patients with tissue helminthiases. All of the ELISA data with the 4 major helminth antigens were included in this study. Only 165 of them were analyzed of their clinical manifestations.
Parasite and parasite antigens
Crude extracts of live worms of Clonorchis sinensis, Paragonimus westermani, and larval spargana were obtained from the homogenized worms in phosphate buffered saline (PBS) at pH 7.2 (8.1 mM Na2PO4, 1.5 mM KH2PO4, and 136 mM NaCl) and protease inhibitors (1 mM tosyl-L-lysine chloromethyl ketone, 100 μM iodoacetamide, and 10 μg/mL pepstatin A). The crude extracts were centrifuged at 13,000 rpm for 30 minutes at 4°C and the supernatant was aliquoted and preserved at −70ºC until used as crude antigens. Cystic fluid of metacestodes of Taenia solium, which were collected from naturally infected pigs in China, was frozen at −70ºC and was used as antigen for cysticercosis ELISA. The protein concentration of the antigens was estimated by the BCA™ protein assay kit (Pierce, Rockford, IL, USA).
Serology by ELISA
Each serum sample was tested for 4 antigens simultaneously by ELISA to detect specific immunoglobulin G (IgG) antibodies. Every 96-wells included positive and negative reference serum samples which were previously confirmed in the serology laboratory. The conventional ELISA procedure was applied to the requested serum samples as previously described (45678). The substrate for color reaction was 100 μL of tetramethyl benzidine (TMB; Pierce). The absorbance was measured at 450 nm with the Emax precision microplate reader (Molecular Devices, Sunnyvale, CA, USA). The whole assays were duplicated and mean absorbance was reported. The samples with absorbance over the cut-off values were regarded as positive: 0.25 for clonorchiasis, 0.28 for paragonimiasis, 0.29 for cysticercosis, 0.24 for sparganosis.
Statistical analysis
All analyses were carried out with SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). A P value of less than 0.05 was considered to indicate statistical significance.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Seoul National University, College of Medicine, Seoul, Korea (IRB No. E-1205-009-408). The IRB waived informed consent from the subjects under the condition of anonymous collection of serum samples from the serum pools of involved authors' institution. All of the procedures followed the guidelines of the IRB.
Go to :
RESULTS
Demography of subjected patients
The mean age of the 6,017 study subjects was 51.5 ± 15.1 years, a range of 1–104. There were 3,763 men, 1,741 women, and unknown 513. Most tests were originally requested to confirm or differentiate the tissue helminthiasis. A few of them were repeatedly requested more than twice for follow-up but not specified due to anonymous data management.
Secular trends in seropositivity of clonorchiasis, paragonimiasis, cysticercosis, and sparganosis
From 1996 to 2006, 6,017 serum samples were requested for multi-antigen ELISA of 4 major tissue helminthiases; clonorchiasis, paragonimiasis, cysticercosis, and sparganosis. There were 1,502 (25.0%) seropositive subjects for any of the 4 helminthiases. For clonorchiasis 728 (12.1%) were positive, for paragonimiasis 166 (2.8%), for cysticercosis 729 (12.1%), and sparganosis were 263 (4.4%) (Table 1). During the period of 1996–2006, the seropositive rates of clonorchiasis, sparganosis, and cysticercosis were fluctuating but slowly decreasing after 2004 (Fig. 1).

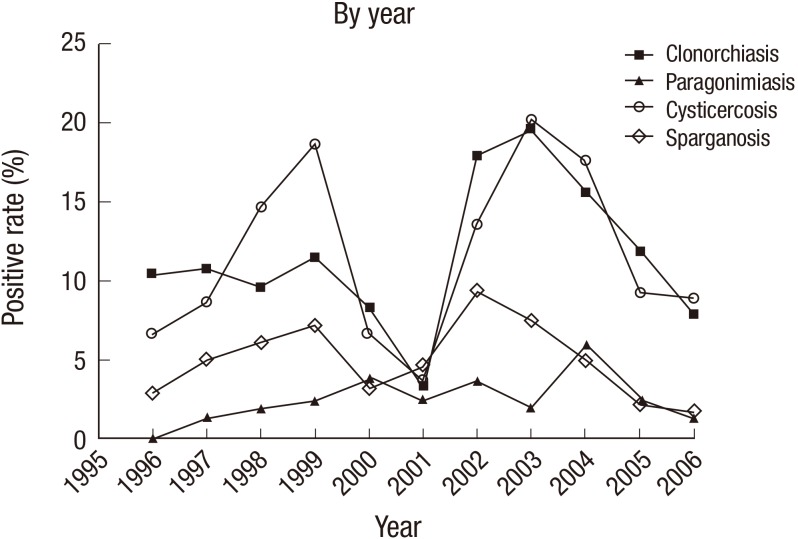 | Fig. 1Changes in ELISA positive rates of clonorchiasis, paragonimiasis, sparganosis, and cysticercosis among suspected patients in Korea from 1996 to 2006.
ELISA = enzyme-linked immunosorbent assay.
|
Table 1
ELISA positive rates by helminthiases
![]()
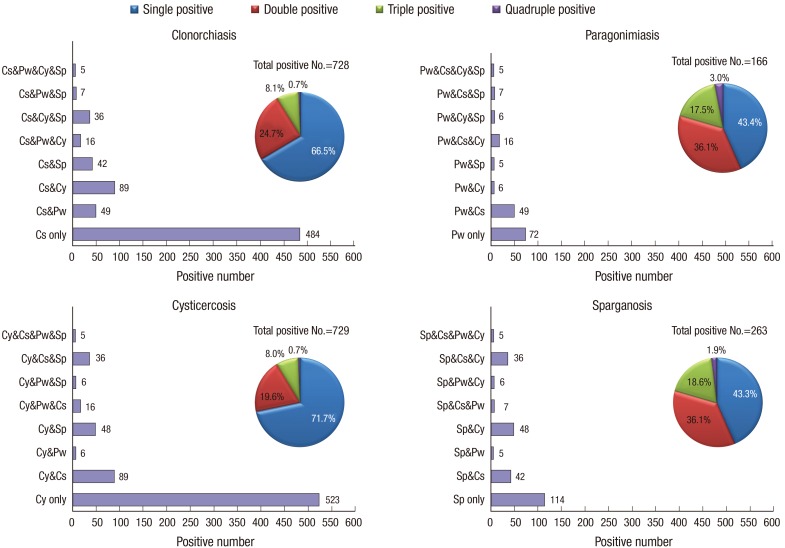
Multi-antigen positivity
The positive serologic reaction to multi-antigens was observed in 309 (20.6%) of the 1,502 total seropositive subjects (Fig. 2). Of the 728 positive samples for clonorchiasis, 244 (33.5%) were simultaneously positive to other antigens. A total of 180 (24.7%) were double positive, 59 (8.1%) triple positive, and 5 (0.7%) quadruple positive. The double positive reaction of clonorchiasis was common with cysticercosis (89 serum samples) or with paragonimiasis (49 serum samples). A total of 166 serum samples were positive for paragonimiasis and 94 (56.6%) of them were multiple positive. The most common positive reaction was double with clonorchiasis (49; 29.5%), and 16 (9.6%) were triple positive with cysticercosis. Of the 729 cysticercosis positive cases 206 (28.3%) were multiple positive; 89 (12.2%) with clonorchiasis, 48 (6.6%) with sparganosis, 6 (0.8%) with paragonimiasis, 36 (4.9%) triple positive with clonorchiasis and sparganosis, and 5 (0.7%) for all 4 helminthiases. Sparganosis was positive in 263 of the screened subjects, and 149 (56.7%) were multipositive; 48 (18.3%) were with cysticercosis, 42 (16.0%) with clonorchiasis. Those of multi-antigen positivity were regarded as positive for the antigen of strongest reaction and with cross-reaction to others.
Prevalence of helminthiases by age and sex
The overall positive rate of helminthiases was 25.0% (Table 2). The patients with the highest rate were 27.9% in their 60s and 26.4% was the next in their 70s. Those with the lowest rate were in their 20s (13.9%). The positive rate by sex was 27.4% in men and 19.1% in women (Table 3) (P < 0.001). Table 3 shows disease-specific prevalence by sex, and the gap between men and women especially resulted in the different positive rates in clonorchiasis.
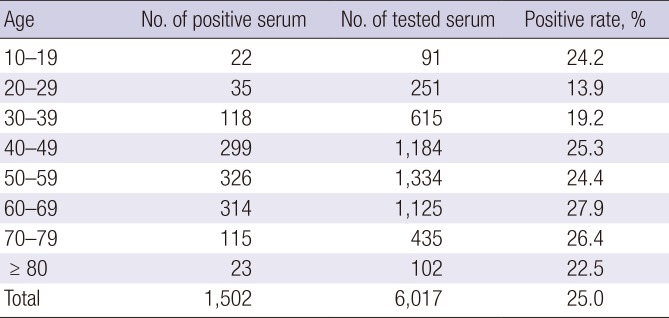

Table 2
ELISA positive rates of helminthiases by age
![]()
Table 3
Prevalence of helminthiases by gender
![]()
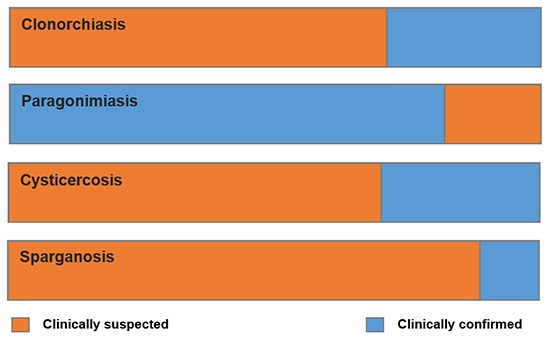
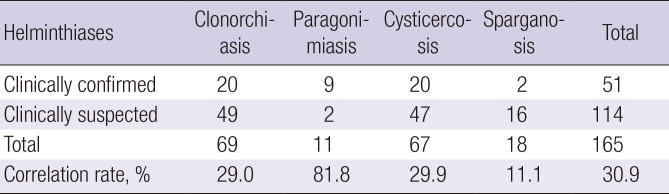
Correlation analysis of seropositive subjects with clinical diagnosis
Most of the subjects were clinically suspected and the ELISA tests were requested for differential diagnosis. Medical records of 165 patients with positive parasite-specific IgG antibodies were reviewed to confirm the clinical diagnosis by results of white blood cell (WBC) count, eosinophil count, clinical manifestations, and exposure history. Of the 165 patients, 51 (30.9%) were clinically confirmed. The correlation rate with clinical diagnosis for clonorchiasis was 29.0% (20/69), paragonimiasis 81.8% (9/11), cysticercosis 29.9% (20/67), and sparganosis 11.1% (2/18) (Table 4). Most of the seropositive cases of paragonimiasis were compatible with the clinical diagnosis. There was no significant difference of WBC numbers and eosinophil numbers between the suspected and confirmed groups. ELISA absorbance was compared between clinically suspected only and clinically confirmed by other diagnostic methods (Fig. 3). The high ELISA absorbance was significantly correlated with clinical diagnosis of cysticercosis (P = 0.009). There was no significant correlation of ELISA absorbance between clonorchiasis (n = 21) and clonorchiasis with cholangiocarcinoma (n = 24) (P = 0.980) (Fig. 4).
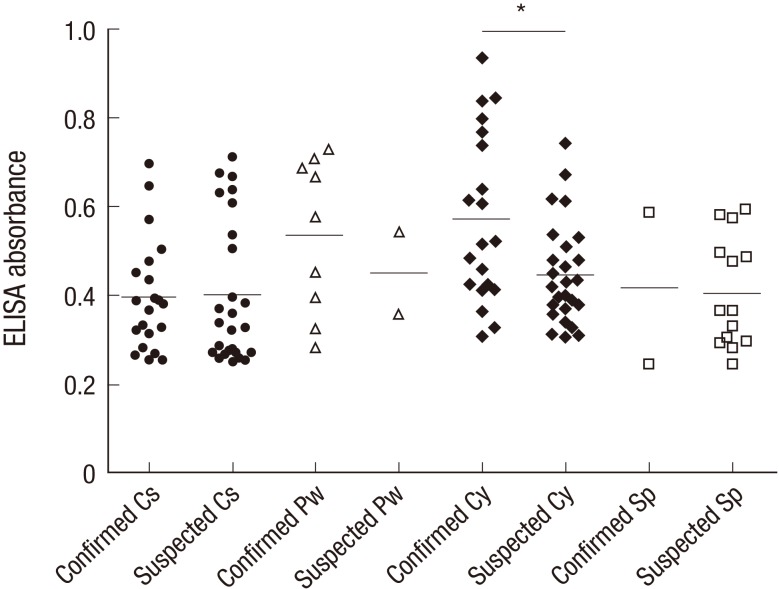 | Fig. 3ELISA absorbance distribution of clinically confirmed and suspected patients.
ELISA = enzyme-linked immunosorbent assay, Cs = clonorchiasis, Pw = paragonimiasis, Sp = sparganosis, Cy = cysticercosis.
*P = 0.009.
|
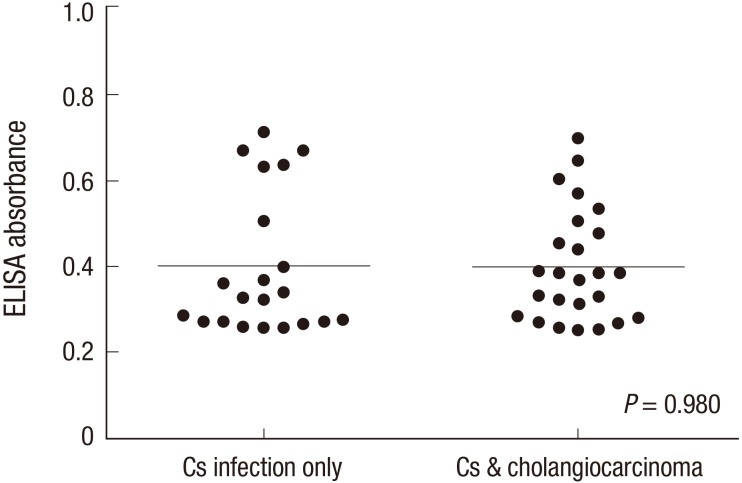 | Fig. 4ELISA absorbance of patients with clonorchiasis and clonorchiasis with cholangiocarcinoma.
ELISA = enzyme-linked immunosorbent assay, Cs = clonorchiasis.
|
Go to :
DISCUSSION
The overall serology positive rate of the multi-antigen ELISA for 4 tissue helminthiases was 25.0% of the whole 6,017 screened subjects at our laboratory. By individual helminthiasis, the overall positive rate was 12.1%, 2.8%, 12.1%, and 4.4% for clonorchiasis, paragonimiasis, cysticercosis, and sparganosis, respectively. Although most of the requested subjects were clinically suspected, overall seropositivity remained as high as 25% for 4 major tissue-invading helminthiases from 1996 to 2006 in Korea. Since the ELISA system detects serum IgG antibodies, the positive reaction means presence of reacting antibodies by antigenic exposure due to previous infection. Furthermore, helminths are sharing some antigenic molecules which cause cross-reactions (34678910). The ELISA positive reactions in the present study included real infection, past infection, and cross-reaction.
Lee et al. (3) reported serum antibody positive rates of 7.6% for total helminthiasis and 5.0%, 1.4%, 4.2%, and 2.4% for clonorchiasis, paragonimiasis, cysticercosis, and sparganosis, respectively, after subjecting 74,448 requested samples over the country from 1993 to 2006. The present positive rates during 1996–2006 were about double of theirs. The higher rates in the present study may be interpreted by the difference of locality of target subjects. Lee et al. (3) subjected the patients referred from the whole country but the present study mainly subjected patients from Seoul National University Hospital and sister hospitals in Seoul or suburbs. The positive rates by locality, reported by Lee et al. (3), were significantly higher among patients in Seoul than those in other cities or provinces. Since the Seoul National University Hospital plays the role of the central tertiary hospital for patients with some difficult diseases of diagnosis or treatment, there has been a tendency of patient concentration in the big tertiary hospitals in Seoul including Seoul National University and sister hospitals. That is the main reason of higher seropositive rates among patients in Seoul although the transmission of tissue-invading helminths occurs mainly in rural areas outside of Seoul. Because most of the tissue helminthiases have non-specific symptoms or signs, it is not easy to care for the patients correctly.
Medical records of 165 ELISA positive patients were reviewed and 51 (30.9%) of them were confirmed of the clinical evidence of tissue helminthiases. The highest correlation rate was 81.8% (9/11) for paragonimiasis and the lowest was 11.1% (2/18) for sparganosis. The rate was 29.0% (20/69) in clonorchiasis and 29.9% (20/67) in cysticercosis, and these confirming rates were rather lower than expected. Of course, the 114 remaining unconfirmed patients were highly suspected and a part of them might be true in spite of negative clinical evidence. Also, some cured patients may be included. The present findings on the relevance between clinical evidence and serology demonstrated that serodiagnosis of tissue helminthiases is less specific than expected. Especially the ELISA positivity of clonorchiasis and cysticercosis should be reevaluated because there have been increasing numbers of cured patients in Korea. The ELISA diagnosis is reliable for paragonimiasis but not for sparganosis. The serodiagnosis of sparganosis may include false positive by cross-reaction and must be reevaluated by further studies. Although clinical evidence is not definite, high ELISA absorbance may suggest high probability and it is significant in cysticercosis.
Clonorchiasis is still actively transmitted in Korea. According to Jeong et al. (11), the egg positive rates of clonorchiasis were 11.7%, 9.9%, 6.5%, 3.1%, and 1.0% among residents living along the Nakdong, Seomjin, Geum, Yeongsan, and Han River, respectively. The report confirmed that clonorchiasis is still actively transmitted in endemic areas in Korea. The ELISA is a useful diagnostic tool for clonorchiasis as well as stool microscopy. The ELISA diagnosis of clonorchiasis using crude antigen has 88.2% sensitivity and 87.8% specificity in our laboratory (4). Since the ELISA detects specific serum IgG antibody to the trematode, the positivity includes cured cases as well as present infection. Therefore, the present 12.1% positive rate of clonorchiasis may include both active and past infections. Since most of clonorchiasis cases become more and more lightly infected, the diagnostic sensitivity of both stool microscopy and ELISA becomes less sensitive. In this context, it is better to make diagnosis of clonorchiasis by either positive by stool microscopy or ELISA.
The present findings were analyzed by year, age, and sex. The positive rates showed a range of fluctuation but it is hard to confirm clear tendency of yearly trends of the ELISA positive rates. Since the laboratory technical person was changed and the service was stopped for a while and rebuilt, the results were inconsistent in 2001. By age, the highest rate was observed in 60s which was significant only in clonorchiasis. By sex, men showed significantly higher prevalence than women and this finding was mainly attributed by clonorchiasis. The present finding was similar with the previous report in 2010 (3).
Polyparasitism and consequent cross-reaction between the 4 helminth antigens should be noted. In the present study, cross-reaction was observed mainly between helminths in the same classes, such as clonorchiasis and paragonimiasis, sparganosis, and cysticercosis (345678). For example, C. sinensis antigen reacted more frequently with 3 other tissue-invading helminthiases, and cross-reacted with 25% of serum samples from paragonimiasis (4). The ELISA using crude antigen of P. westermani provided good sensitivity and specificity over 95% to serum samples from patients with paragonimiasis (6), but serum samples from clinically confirmed sparganosis showed slightly higher cross-reaction to cysticercus antigen (12). Nevertheless, multi-antigen ELISA is indispensable to distinguish the cross-reactions (13).
The ELISA absorbance was same between confirmed patients with clonorchiasis and clonorchiasis with cholangiocarcinoma. ELISA can hardly provide any clue to expect cholangiocarcinoma in patients with clonorchiasis.
This study was limited by its retrospective nature and also by the inability to confirm cross reactivity by other serological methods. Since only requested subjects were tested, clinical information was very limited. Only 165 of the ELISA positive patients were reviewed of their medical records, and the small number limited the clinical significance. Also, it was impossible to confirm whether multi-antigen positive reaction was by real polyparasitism or by cross-reaction (13). Fortunately, the intestinal helminths are rare and the cross-reaction by them may be negligible. To improve the specificity, recombinant proteins were recommended for antigens of ELISA (14151617).
In conclusion, the multi-antigen ELISA using 4 helminth antigens is useful to differentiate suspected tissue-invading helminthiases, especially ELISA diagnosis of paragonimiasis is reliable. The seropositivity is still as high as 25% among suspected patients in Korea.
Go to :
 XML Download
XML Download