

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Globally, Neisseria meningitidis (meningococcus) is an important causative agent of sepsis and meningitis, responsible for substantial morbidity and mortality. Even with appropriate treatment, the case fatality rate ranges from 5% to 15% (1). Pharyngeal carriage of meningococci is a prerequisite for invasive meningococcal disease (2). This bacterium can cross the epithelial barrier of the pharynx to enter the bloodstream, causing septicemia. Subsequently, it can cross the blood-brain barrier, giving rise to meningitis (3). Only few genetic types, termed “hypervirulent clones,” are responsible for most disease, in contrast to the extremely diverse carriage isolates (4). To understand the epidemiology and transmission of meningococcal disease, molecular characterization of meningococci isolated from the nasopharynx—the reservoir for invasive, disease-causing strains—is essential.
Meningococcal carriage rates vary by age, with peak prevalence (10%–35%) in adolescents and young adults (56). Male sex, cigarette smoking, passive exposure to smoke, kissing, and overcrowding are associated with carriage, and many of these factors are also risk factors for meningococcal disease (578910). To understand the epidemiology and pathogenesis of meningococcal disease, the carriage state needs to be investigated. Although many carriage studies have been conducted among various populations in Europe and the United States (6), data is limited in Korea. Most Korean data is derived from epidemiologic studies of the Korean army, because of the high prevalence of meningococcal infection (and high associated mortality rate) in this particular group (111213141516). Only 4 reports have evaluated other populations (12171819). Despite the high risk of meningococcal carriage among adolescents, only 2 Korean studies of adolescents have been reported (1217). Choi et al. (17) reported on the carriage rate in high-school students. However, their study was a contact investigation of a case of meningococcal meningitis, and the study population was small (n = 78). Moreover, no serologic or genetic characterization of isolates has been performed in any studies of adolescents.
The aim of the present study was to gain information about the carriage of N. meningitidis among Korean adolescents. We provide the first report on the carriage rate, serogroup, and multilocus sequence typing (MLST) of meningococcal carrier isolates obtained from adolescents in Korea.
MATERIALS AND METHODS
Study population and recruitment
Subjects were recruited from 9 high schools (A to I) in Gyeonggi province, Korea (Ansan, Bucheon, Goyang, Gwangmyeong, Siheung, and Suwon), and samples were collected in April and May 2015. Two schools (A and G) had dormitories. Subjects who agreed to participate in the study and met the inclusion criteria (the first year of high school, equal to the 10th of 12 years of formal education in western countries) were enrolled. Individuals with craniofacial malformations were excluded. A trained physician took a posterior oropharyngeal swab (Culture Swab™ Plus Amies Gel with Charcoal; BD Diagnostic Systems, Sparks, MD, USA) from behind the uvula, the posterior wall of the oropharynx.
Questionnaire for risk factor analysis
The baseline characteristics of each subject were assessed through a questionnaire. Questions pertained to personal characteristics, place of residence, recent symptoms of upper respiratory tract infection, recent history of antibiotic use, active smoking, and visits to crowded places in the past week. Active smoking was defined as currently smoking at least one cigarette per day. Crowded places included shopping malls, public game rooms, or private academies; subjects were asked how often they frequented such places in the last week. In the risk factor analysis, frequent visits to crowded places was defined as more than 4 visits in the last week.
Laboratory methods
Isolation of meningococcal strains
The oropharyngeal swabs were immediately placed in transport media (Culture Swab™ Plus Amies Gel with Charcoal; BD Diagnostic Systems), stored at room temperature, and transported within 4 hours to the Ewha Center for Vaccine Evaluation and Study, Medical Research Institute, Ewha Womans University School of Medicine. The swabs were immediately inoculated on to Thayer-Martin selective agar for the growth of Neisseria species. The media were incubated at 37°C in 5% CO2 and examined at 18–24 hours for the growth of meningococcus-like colonies. The plates with negative growth after 24 hours were re-incubated and re-examined after 48 hours. Suspected meningococcal colonies (round, smooth, moist, glistening, convex, and gray) were sub-cultured on chocolate agar for identification with matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry (Vitek® MS; BioMérieux, Marcy l'Etoile, France). After analysis, acceptable identification was defined as all confidence scores of duplicates being > 90%. The results were interpreted as “not acceptable” for identification if there were discrepancies between 2 spots, or when the confidence score was < 90% in any spot. If the result of the analysis was “not acceptable,” the conventional method of identification was performed. The conventional method included Gram staining, oxidase tests, catalase tests, and carbohydrate fermentation tests. Gram-negative cocci that were oxidase- and catalase-positive were identified as meningococcus. In addition, molecular confirmation of meningococcus was accomplished by polymerase chain reaction (PCR) amplification with the presence of the conserved gene crgA (20). All confirmed isolates were stored in 10% skim milk and 10% glycerol in trypticase soy broth at −70°C for subsequent serogrouping and MLST.
MALDI-TOF analysis
The analysis was performed according to the manufacturer's instructions. All suspected isolates were inoculated in double deposit of a disposable target slide (Vitek® MSDS; BioMérieux) by picking an overnight culture with a 1 μL disposable loop (one colony/deposit). The preparations were overlaid with 1 μL of α-cyano-4-hydroxycinnamic acid (CHCA) matrix solution. After drying, the target plate was loaded into the mass spectrometer. Spectra were generated and compared to the reference database (Saramis for Vitek® MS RUO system; BioMérieux). After analysis, results were provided by the instrument system as a percentage score representing similarity in terms of presence/absence of specific peaks between the generated spectrum and the database spectra. All identifications at the genus or species level with a score > 90% were considered reliable identifications.
Serogrouping
PCR was performed for all meningococcal isolates using species-specific primers. Genomic DNA was isolated using the Wizard Genomic DNA Purification Kit (Promega, Madison, WI, USA). PCR was performed as described by Taha (20) and Bennett et al. (21). Target genes to detect meningococcus for serogrouping were crgA (common primer), orf-2 (serogroup A), siaD (serogroups B, C, W135, and Y), and ctrA (serogroup 29E, X, and Z).
MLST
MLST was performed on all culture isolates using fragments from 7 housekeeping genes (abcZ, adk, aroE, fumC, gdh, pdhC, and pgm) for typing (22). After DNA preparation and amplification by PCR, sequencing of PCR-amplified fragments using the Sanger method was performed by Macrogen (Seoul, Korea). The sequences were compared with existing alleles on the Neisseria MLST website (http://pubmlst.org/neisseria/) for determination of allele numbers, sequence types (STs), and clonal complexes (CCs) of the isolate. New alleles and STs were submitted to the MLST website for assignment. eBURST v3 software (Imperial College London, London, UK; available at the MLST website, http://eburst.mlst.net/) was used to assess the relationships among the isolates and to assign the strains to a CC.
Statistical analysis
Continuous variables were described as means, and categorical variables as numbers and percentages. Risk factor analysis was performed using logistic regression, obtaining odds ratios (ORs) as a measure of association, with their respective 95% confidence intervals (CIs). P < 0.05 was considered significant for statistical analysis.
Ethics statement
The protocol, informed consent, and assent form were reviewed and approved by Institutional Review Board of Ewha Womans University Mokdong Hospital (EUMC 2015-01-061). The study was conducted in accordance with good clinical practices (national regulations and International Conference on Harmonization [ICH] E6) and the principles of the Helsinki Declaration. Written informed consent was obtained from all participants and their parents or legal guardians following a detailed explanation of the study.
RESULTS
Baseline characteristics and meningococcal carriage rate
A total of 2,908 students in 9 high schools were invited to participate to the study, and 1,460 were enrolled (response rate, 50.2% [95% CI, 48.4%–52.0%]). The reasons for refusal and the demographic data of those who refused were not investigated further. The demographic characteristics of the enrolled subjects are shown in Table 1. Meningococcus was identified from 49 (3.4%) of 1,460 nasopharyngeal swab samples (Table 1). Consequently, the carriage rate of each school ranged from 1.3% to 6.8%, and the highest carriage rate was observed in school D.
Table 1
Demographic data of subjects and carriage rate

![]()
Risk factor analysis
Associations between social or behavioral factors and meningococcal carriage rate were assessed. The proportion of subjects with each risk factor is shown in Table 2. Active current smokers (122/1,460 [8.4%]) had significantly higher carriage rates (10/122 [8.2%]) than non-smokers (39/1,338 [2.9%]) (OR, 2.97; P = 0.002). Sex (male, 902/1,460 [61.8%]) was also significant factor, with a higher rate (40/902 [4.4%]) in boys than in girls (9/558 [1.6%]) (OR, 2.83; P = 0.004). Although not significant, subjects with a history of frequently attending crowded places within the last week (288/1,460 [19.7%]) had higher carriage rates (15/288 [5.21%]) (OR, 1.84; P = 0.051). However, passive smoking, dormitory residents, and symptoms of current upper respiratory tract infection had little or no effect.
Table 2
Univariate analysis of risk factors for meningococcal carriage among 1,460 healthy Korean adolescents

Values are presented as number (%).
OR = odds ratio, CI = confidence interval.
*Statistically significant risk factor for meningococcal carriage (P < 0.05); †Daily smoker, smoking > 1 cigarette per day; ‡Exposure to smoke for > 1 hour per week; §Crowded places include shopping malls, public game rooms, or private academies.
![]()
Serogroups and STs of carrier strains
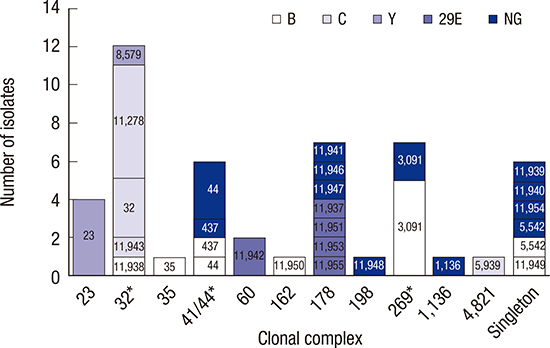
Of the 49 meningococcal isolates, 15 (30.6%) were non-groupable (Table 1). Serogroup B was the most common (24.5%) serogroup identified. Serogroups A, W135, X, and Z were not found. All isolates of serogroup Y were collected from school D (Table 1). By MLST analysis, 16 STs (ST-11937, ST-11938, ST-11939, ST-11940, ST-11941, ST-11942, ST-11943, ST-11946, ST-11947, ST-11948, ST-11949, ST-11950, ST-11951, ST-11953, ST-11954, and ST-11955) were newly assigned and 27 different STs were identified in this study (Fig. 1). The most frequent STs were ST-3091 (7 isolates, 14.3%) and 11278 (6 isolates, 12.2%). Of 27 STs, 19 (70.4%) were represented by only one isolate each. A total of 25 isolates (51.0%) belonged to CCs known as hypervirulent clones (CC-32, CC-41/44, and CC-269). Fig. 1 shows the distribution of the meningococcal isolates by capsular group and CC. Serogroup B, C, and Y isolates mostly belonged to CC-269, CC-32, and CC-23, respectively. Although most STs were confined to a single serogroup, ST-44, ST-437, ST-3091, and ST-5542 were shared by 2 serogroups (serogroup B and a non-groupable serogroup). In serogroup B, 8 isolates (66.7%) shared STs with non-groupable isolates. The distribution of serogroups and STs is illustrated in the eBURST diagram displayed in Fig. 2. There were 11 CCs and 6 singletons, with CC-178 and CC-32 comprised of various STs.
 | Fig. 1Association between serogroups and CCs of meningococcal isolates identified in healthy Korean adolescents. The different colors of the bars correspond to different serogroups as determined by PCR. STs are shown on bars of CCs.
CC = clonal complex, PCR = polymerase chain reaction, ST = sequence type, NG = non-groupable.
*The asterisk indicates hypervirulent clones.
|
 | Fig. 2Single locus variant eBURST network of the 49 meningococcal carriage strains. The circle sizes correlate with the number of strains of each ST. Single locus variants are connected by lines. The serogroup of each ST is shown within parentheses.
eBURST = electronic Based Upon Related Sequence Types, ST = sequence type, CC = clonal complex, NG = non-groupable.
|
DISCUSSION
This study provides the first data on the carriage rates of meningococcus among adolescents in Korea. Isolated meningococcal strains were analyzed according to host characteristics, genotype, and serogroup. The remarkable finding of this study is that serogroup B was the most prevalent, as has previously been reported in western countries (232425). However, the carriage rate was lower than in other reports (5611121314151617182324). Our observed carriage rate (3.4%) was much lower than expected on the basis of previous studies of adolescents (carriage rate, 10.4%–18.5%) (52324). Christensen et al. (6) systematically reviewed 89 studies, conducted worldwide, of meningococcal carriage rates. They estimated that the carriage rate among 15-year-olds ranged from 7.9% to 17.4%. Our finding of a low carriage rate may explain the low incidence (approximately 20 cases/year) of invasive meningococcal disease in Korea (http://stat.cdc.go.kr/). The differences in genetic background of hosts, climates, and geographic areas could be reasons for the low carriage rate. Different social behavior patterns could also explain the low prevalence we observed. Among British and Italian teenagers (524), the prevalence of known risk factors for meningococcal carriage (for example, smoking, exposure to cigarette smoke, and visiting crowded places) is reportedly higher than in Korean adolescents.
In Korea, meningococcal meningitis is a notifiable disease, and approximately 20 cases are reported annually (http://stat.cdc.go.kr/). Although meningococcal disease is regarded as a rare infection in Korea, several meningococcal outbreaks in the Korean army have been reported (11). An outbreak among military recruits in 2011, in particular, raised public awareness of the need for meningococcal vaccination (26). Since then, 2 quadrivalent meningococcal conjugate vaccines (MCV4) have been introduced, one in 2012 and the other in 2014. MCV4 vaccination was introduced in the national immunization program for military recruits in Korea in 2012. Although a limited number of carriage studies have been conducted among the general population in Korea, carriage rates among military recruits have been evaluated (111213141516). In the 1990s, the carriage rates among military trainees were 8.1%–79.4%, varying according to seasonality and duration of training. However, the carriage rates declined to 8.5%–21.7% in the 2010s. Carriage rates among non-military Korean populations were reported in only 4 studies: 0.8% in young children (19), 7.7% in adolescents in contact with a case of invasive disease (17), 25.3%–41.0% in adolescents (12), and 11.8% in university students living in dormitories (18). However, these results could not be compared directly since each study's subjects had different characteristics in terms of age, epidemic setting, or residential environment. A study conducted among adolescent male dormitory residents near a military base, which are risk factors for meningococcal carriage, showed high carriage rates (12).
Although not directly comparable, the carriage rate in the present study is relatively low. The swabbing technique used and culture conditions may influence the carriage rate (2728). We performed this study as recommended in the literature to increase the yield of meningococci. The sampling site should include the posterior pharyngeal wall behind the uvula (29). Charcoal-impregnated swabs are recommended. To inhibit the growth of other bacteria and to improve the yield of meningococci from samples, agar plates with selective antibiotics are used (30). These methods help to reduce the frequency of false negative results. Swabs may be directly plated onto solid medium on site or may be placed in an appropriate transport medium, such as Stuart medium, before plating in the laboratory. Caugant et al. (28) reported that direct plating was not significantly better than the use of Stuart's transport media, at least not when the plating in the laboratory was performed within 4 hours of acquiring the samples. Our swabs were placed in charcoal-impregnated Amies gel (a modification of Stuart medium) and plated onto selective agar medium within 4 hours to increase the recovery of meningococci. These procedures could minimize the influence of non-direct plating on carriage results.
Meningococcus is divided into 13 serogroups based on the immunologic specificity of the capsular polysaccharide. The capsular polysaccharide is the major virulence factor and the prime target for mucosal and humoral immunity. Five of these serogroups (A, B, C, W135, and Y) cause > 90% of invasive disease worldwide. Epidemic meningococcal diseases caused by serogroup A have largely been confined to developing countries, most often in the meningitis belt of sub-Saharan Africa (31). In Europe, most cases of meningococcal disease are caused by serogroups B and C (32). Serogroup B was shown to be dominant in European and US carriage studies (232425), whereas serogroups Y and A are frequently found in Africa (33). In the present study, as found in western countries, serogroup B was most prevalent, followed by serogroups C and Y. These patterns were also found in recent studies of military recruits (16), unlike the pattern found in the 1990s (1215). Despite limited information from the general population, serogroup B was found more frequently in recent carriage studies than was the case before the 2000s. In view of these results, the prevalence of serogroup B in meningococcal carriage is considered to have increased in Korea, as in western countries. Many carriage strains can easily lose their capsule, becoming serologically non-groupable (2534). The proportion of non-groupable isolates among carriage isolates was up to 88% in an immunized population (35). In our study, 42.9% of isolates were non-groupable, a figure comparable with those of previous carriage studies (182434).
The meningococcal vaccines currently available in Korea are based on the capsular polysaccharides of meningococcal serogroups A, C, W135, and Y. None of these vaccines provide protection against serogroup B meningococci. For this reason, the sub-capsular protein-based vaccines have been investigated and used to prevent meningococcal serogroup B diseases in western countries. However, since the sub-capsular antigens are variably expressed and antigenically variable among meningococcal isolates, prediction of vaccine coverage is an important issue for preventing meningococcal serogroup B diseases (36). In our results, serogroup B was dominant and was related to a hypervirulent CC. Proper prevention of meningococcal disease will require not only the introduction of meningococcal B vaccines, but also detailed characterization of circulating meningococcal B isolates.
Meningococcus is genetically and antigenically highly diverse. Meningococcal strains isolated from carriers are typically much more diverse (28). They are extremely heterogeneous genetically, with only a low proportion of carrier strains representing hyperinvasive clones (32). Most cases of meningococcal disease worldwide are caused by a limited number of hypervirulent lineages, which appear to have an increased propensity to cause invasive disease. To characterize meningococcal isolates, MLST is used as a highly reliable and reproducible method (37). The general acceptance of MLST over the past 10 years has enabled the assembly of a public repository of genotypic data representing well over 10,000 meningococcal isolates from both cases of disease and carriers in various parts of the world (http://pubmlst.org/neisseria). The association of clone complexes with carriage or disease could be measured by the ratio of patient-to-carrier strains for the various lineages represented in the database. In the PubMLST database, CC-1, CC-5, CC-8, CC-11, CC-18, CC-32, CC-41/44, CC-269, and CC-334 were positively associated with disease (disease/carriage ratio > 1), whereas CC-23 and CC-35 were positively associated with carriage (disease/carriage ratio < 1) (4). CC-269 has been identified as a major clone in various meningococcal disease surveillances (3839). The majority of serogroups B and C isolates in this carriage study were included in the hyperinvasive clone complexes, CC-32 and CC-269. However, these hypervirulent clones formed only a small proportion of meningococci carried in Italian adolescents and young adults from the UK (2324). These data suggest that awareness and preparation for preventive measures against outbreaks of meningococcal disease might be required. On the contrary, almost all non-groupable isolates were included in the CC with a low disease/carriage ratio.
The strengths of this study are that it is the first carriage evaluation of a large adolescent population in Korea and that it used genotyping. The molecular characterization of the colonized organism is essential to further understanding of the epidemiology of the disease. The molecular characterization results provide valuable information to improve knowledge of the epidemiology of meningococci in Korea. MALDI-TOF was used for the identification of meningococci in this survey, and yielded reliable results. MALDI-TOF mass spectrometry, based on the detection of protein or nucleic acid, has become an important tool in microbiology because it can reduce the time and labor needed to identify organisms (40). MALDI-TOF takes a few seconds to identify bacteria, whereas conventional methods take at least a day. Therefore, it is a useful method to evaluate a large number of samples.
Our study did have some limitations. Despite the large number of subjects, the results may not represent the epidemiology of meningococcal carriage in Korea due to the limited geographic area from which subjects were drawn. The high refusal rate may have introduced selection bias. Because no information could be obtained from refusers, this bias could not be estimated. Since this carriage study was cross-sectional study, seasonal variation and duration of the carrier state could not be evaluated. The number of dormitory residents included in this survey was insufficient to permit a risk factor analysis. Because our risk assessment was based on the response to a questionnaire, recall bias might have influenced the results, especially regarding the history of recent upper respiratory infection or visiting crowded areas.
In conclusion, we provide the first report on the carriage rate, serogroup, and MLST of meningococcal carrier isolates obtained from Korean adolescents. As in western countries, meningococcal serogroup B has emerged in Korea, and hypervirulent clones, such as CC-269, were identified. Ongoing monitoring of the genetic and serologic characteristics of circulating meningococcal isolates and ongoing assessment of the potential strain coverage of meningococcal vaccines, are necessary.
 XML Download
XML Download