

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Esophageal cancer is one of the most common malignancies and a major cause of cancer-related deaths worldwide (1). Over 50% esophageal cancers are found to be incurable at the time of diagnosis because of metastases (2). Dysphagia is the most common symptom of incurable esophageal cancer. The aim of esophageal stenting is to restore luminal patency and thereby maintain oral intake and improve quality of life. However, this procedure carries a risk of major complications such as bleeding and perforation (3). Since the first reports of esophageal stents in the late 1970s, these devices have rapidly evolved from rigid plastic tubes to flexible, self-expanding metallic stents (SEMS) (4). SEMS are cylindrical metallic frames that exert self-expansive forces until they reach their maximum fixed diameter (5). Palliation of esophageal cancer with SEMS was first reported by Domschke et al. (6) in 1990. Since then, SEMS placement has developed into a widely accepted method for treating malignant esophageal strictures and esophagorespiratory fistulas (ERFs) (3).
TYPES OF SEMS
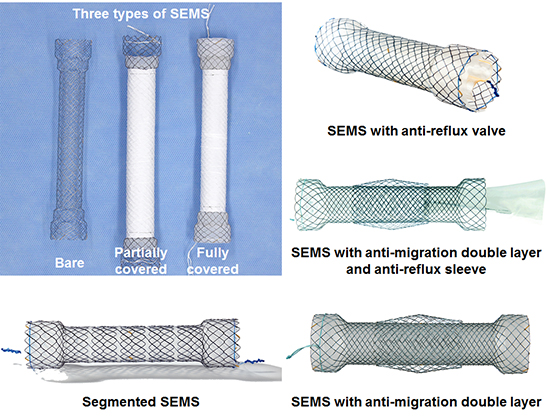
A wide range of SEMS for esophageal cancer are available in Korea (Table 1), and even more are available internationally. Knowledge of the advantages and disadvantages associated with different designs aids physicians in selecting the optimal SEMS for a given condition. Early SEMS were woven from stainless steel wires. At present, all available SEMS are woven from wires made of nitinol, a nickel and titanium alloy known for its shape-memory and superelastic properties. Nitinol SEMS are a major breakthrough because of their greater conformability and smaller profile compared with those of stainless steel SEMS. Two different methods are used to weave SEMS: braiding and knitting (Fig. 1). Braided SEMS are composed of crisscrossed wires that are easily displaced against each other. These SEMS are highly flexible but retain a high axial force. In knitted SEMS, the wire junctions are looped around each other. These SEMS not only are highly flexible but also a have a low axial force and minimal foreshortening. Segmented SEMS consist of several individual SEMS units connected in tandem (Fig. 2). This type of SEMS has high flexibility, but because of the rigidity of the individual SEMS units, it tends to buckle rather than bend. SEMS can be exposed or fully or partially covered with a membrane made of various materials (e.g., silicone and expanded-polytetrafluoroethylene [ePTFE]) to prevent tumor ingrowth (Fig. 3). Most SEMS have antimigration features (e.g., shouldered ends and double-layer design) to decrease stent migration (Fig. 4). To decrease gastroesophageal reflux, some manufacturers offer variants of SEMS with antireflux features such as sleeves and valves (Fig. 5). For insertion, SEMS is compressed and loaded into a distal-release or proximal-release delivery system (Fig. 6). Depending on the profile of the delivery system (> 10.5 Fr or ≤ 10.5 Fr), SEMS is deployed either over the guidewire (over-the-wire technique) or through the working channel of the endoscope (through-the-scope [TTS] technique).
Table 1
Commercially available SEMS for esophageal cancer in Korea

SEMS = self-expanding metallic stents, ePTFE = expanded-polytetrafluoroethylene, TTS = through-the-scope.
![]()
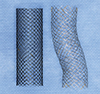 | Fig. 1Photograph shows a braided SEMS (right) (constructed in-house) and a knitted SEMS (left) (constructed in-house).
SEMS = self-expanding metallic stents.
|
 | Fig. 2Photograph shows a segmented SEMS (Choostent; M.I. Tech, Pyeongtaek, Korea).
SEMS = self-expanding metallic stents.
|
 | Fig. 3Photograph shows an uncovered SEMS (right) (EGIS; S & G Biotech, Seongnam, Korea), PCSEMS (middle) (EGIS; S & G Biotech), and FCSEMS (left) (EGIS; S & G Biotech).
SEMS = self-expanding metallic stents, PCSEMS = partially covered self-expanding metallic stents, FCSEMS = fully covered self-expanding metallic stents.
|
 | Fig. 4Photograph shows a SEMS with shouldered ends and a double-layer design (Niti-S Double; Taewoong Medical, Gimpo, Korea).
SEMS = self-expanding metallic stents.
|
 | Fig. 5Photograph shows (A) a SEMS with antireflux sleeves (Niti-S Double Anti-reflux; Taewoong Medical, Gimpo, Korea); (B) a SEMS with antireflux valves (Hanarostent; M.I. Tech, Pyeongtaek, Korea).
SEMS = self-expanding metallic stents.
|
 | Fig. 6Photograph shows a SEMS deployed using a proximal-release delivery system (Niti-S; Taewoong Medical, Gimpo, Korea).
SEMS = self-expanding metallic stents.
|
Uncovered vs. covered SEMS
The currently available SEMS for esophageal cancer include uncovered and covered SEMS. Uncovered SEMS are prone to tumor ingrowth, which can lead to recurrent dysphagia. For this reason, these stents are seldom used today. Instead, covered SEMS have become the mainstay for esophageal cancer because the covering membrane of these stents can prevent recurrent dysphagia caused by tumor ingrowth; however, these stents are much more prone to migration than are uncovered SEMS (3). Covered SEMS are either fully covered (FCSEMS) along the entire length of the stent or partially covered (PCSEMS), in which the proximal and distal ends of the stent are devoid of a covering membrane. Because FCSEMS can prevent tumor embedding entirely, they are usually easily removable under endoscopic and/or fluoroscopic guidance. In contrast, PCSEMS do not prevent tumor embedding within the uncovered portions; therefore, these stents may be less prone to migration and more difficult to remove under endoscopic and/or fluoroscopic guidance than are FCSEMS. In a case series by Seven et al. (7), the migration rate was significantly higher with FCSEMS than with PCSEMS (38% vs. 9%; P < 0.001). However, the tumor overgrowth rate was significantly higher with PCSEMS than with FCSEMS (53% vs. 29%; P = 0.004). As no randomized controlled trials have compared FCSEMS and PCSEMS, future studies are needed to determine the optimal type of covered SEMS.
Anti-migration features
Early-model SEMS often used outer fixation barbs to prevent migration; however, these stents appeared to be associated with an increased risk of intractable pain and fatal bleeding (89). Larger-diameter SEMS have also been investigated. One study showed that 22–25-mm diameter SEMS are associated with a migration rate of only 3% (10). However, several prospective studies have revealed a major complication rate of > 20% and mortality rate of > 6% (891112). Several newly-developed SEMS have antimigration features that take both efficacy and safety into consideration. These SEMS are of 2 types: SEMS with additional components and SEMS with modified shapes. The former includes those with a double layer (Niti-S Double; Taewoong Medical, Gimpo, Korea) and a skidproof design (Hanarostent® Esophagus Skidproof; M.I. Tech, Pyeongtaek, Korea); the latter includes SEMS with a shouldered design. The Niti-S Double SEMS (Taewoong Medical) has an outer uncovered layer and an inner covered layer. Although this stent has a very low migration rate (only 2%–3%), it is much more difficult to remove under endoscopic and/or fluoroscopic guidance compared to conventional FCSEMS because its outer uncovered layer does not prevent tumor embedding (1213). The skidproof SEMS, which has multiple skidproof flaps, has a migration rate of 15%, suggesting that the skidproof flaps are of only limited value for preventing migration (14). The efficacy and safety of the shouldered design for preventing migration is not very well documented in the literature. However, all available SEMS used in Korea for esophageal cancer have adopted this design, with the exception of a few intended for placement in the cervical esophagus. One SEMS with a double-stepped shoulder design (EGIS; S & G Biotech, Seongnam, Korea) is equipped with outer shoulders and relatively small inner shoulders. However, randomized controlled trials are needed to determine whether this stent has a lower migration rate than those with a conventional shoulder design.
Anti-reflux features
Placement of SEMS across the gastroesophageal junction leads to an increased risk of gastroesophageal reflux because the stent can bypass the lower esophageal sphincter. SEMS with antireflux features such as sleeves or valves have been developed to remedy this problem. These SEMS decrease transprosthetic reflux compared to those without antireflux features. Dua et al. (15) reported in their in vitro study that the proportion of daily esophageal acid exposure time was significantly less after placement of SEMS with antireflux sleeve than that without (1% vs. 49%; P = 0.03). Shim et al. (16) reported in their study that the proportion of time during which esophageal pH was < 4 was significantly less in patients who received a SEMS with antireflux valve, compared to those who received a conventional SEMS without antireflux valve (3% vs. 29%; P < 0.001). Laasch et al. (17) reported in their randomized controlled trial that reflux was seen in only 12% patients who received a SEMS with antireflux sleeve, compared to 96% patients who received a conventional SEMS. However, Blomberg et al. (18) reported no significant difference in health-related quality of life between patients who received a SEMS with an antireflux sleeve and those who received a conventional SEMS. Sabharwal et al. (19) reported no significant difference in reflux rate between SEMS with an antireflux sleeve and conventional SEMS used in conjunction with a high-dose proton pump inhibitor (14% vs. 8%; P = 0.650). Coron et al. (20) reported that SEMS with an antireflux valve was effective in preventing reflux, but at the cost of an increased likelihood of minor adverse events such as migration and/or obstruction of SEMS (55% vs. 18%; P = 0.020). On the basis of these results, the routine use of SEMS with antireflux features could not be recommended. However, previous studies were limited by small sample size and variability in antireflux features. Further studies are needed to determine if antireflux features could reduce the risk of gastroesophageal reflux.
Proximal vs. distal-release delivery systems
The majority of available SEMS use a distal-release delivery system. This type of delivery system deploys SEMS by proximally retracting the outer sheath relative to the inner pusher catheter. However, accurate positioning of the proximal end of a SEMS that is distally released may not be possible in certain situations. For example, when there is a need to deploy a SEMS at a more proximal region within the esophageal, the proximal end of SEMS ideally should be deployed above the stricture but below the cricopharyngeal region to avoid irritating the nerves that control the coughing response. Under such circumstances, a proximal-release delivery system that deploys SEMS by distally extending the outer sheath relative to the inner pusher catheter can aid in more accurate placement of the proximal portion of SEMS. However, this type of delivery system only is offered by a few manufacturers.
SEMS PLACEMENT PROCEDURE
SEMS can be placed under endoscopic and/or fluoroscopic guidance. The outcomes of these procedures are the same, regardless of which guidance method is used. Fluoroscopic SEMS placement is usually well-tolerated under local anesthesia, whereas endoscopic SEMS placement usually requires sedation. The authors are radiologists and typically perform SEMS placement under fluoroscopic guidance alone. There are a variety of guidewires and catheters available for SEMS placement. The authors routinely use the 0.035-inch stiff-angled hydrophilic guidewire (Radiofocus M; Terumo, Tokyo, Japan) and the 5.4-Fr multifunctional coil catheter (Song-Lim; S & G Biotech). Once the guidewire and the catheter have been negotiated through the stricture, a limited amount of diluted water-soluble contrast medium is injected through the catheter to delineate the stricture. The location and length of the stricture is radiopaque-marked on the patient's skin, and the catheter is removed with the guidewire left in place. The delivery system is advanced through the stricture over the guidewire, and SEMS is deployed under continuous fluoroscopic monitoring. Balloon dilation of the stricture before SEMS placement is generally discouraged to avoid perforation but can be useful to allow advancement of the delivery system through the stricture. It is important to “overstent” the stricture by at least 1 cm on each end to prevent tumor overgrowth. If the placed SEMS does not expand to at least half of its fully expanded diameter, balloon dilation of SEMS should be performed. After the procedure, patients are allowed oral intake of liquids within 24 hours. Because of the risk of food impaction, they should not be permitted any food until an upper gastrointestinal series after 1–3 days show full expansion of SEMS.
INDICATIONS
Palliative treatment for malignant esophageal strictures
In several randomized controlled trials, SEMS placement has been shown to provide superior efficacy to photodynamic therapy, laser therapy, and surgical bypass for the palliation of malignant esophageal strictures (212223242526). Systematic review and meta-analysis studies have demonstrated a technical success rate of virtually 100% and improvements in dysphagia scores by at least 2 points within 1–2 days of the procedure in > 95% patients (327282930). Self-expandable plastic stents (SEPS) are similar to SEMS with regard to relief of dysphagia in the short term, but adverse events such as migration occur more often with SEPS (31), making SEMS preferable over SEPS for palliating malignant esophageal strictures. Brachytherapy has also been widely used for the palliation of malignant esophageal strictures. According to multicenter randomized control trials, this treatment provides a survival advantage and better quality of life than does SEMS placement for palliating malignant esophageal strictures (3233). However, brachytherapy requires more time to relieve dysphagia than does SEMS placement (33). In addition, brachytherapy has several important limitations, including limited availability, technical difficulty, and the need for dedicated expertise.
Concomitant palliative treatment with SEMS and brachytherapy
Because brachytherapy usually takes 4–6 weeks to relieve dysphagia (34), concomitant palliative treatment with SEMS and brachytherapy has been proposed for palliating malignant esophageal strictures. Several studies have shown that this regimen provides quicker relieve of dysphagia, survival advantages, and possibly a better quality of life than SEMS placement alone (32333536). However, Shin et al. (35) reported a significantly higher risk of complications (i.e., migration, ERF, and bleeding) in patients who underwent concomitant palliative treatment with SEMS and brachytherapy than those who underwent SEMS placement alone (65% vs. 33%; P = 0.040). Several other investigators have also found a high risk of major complications (16%–35%), including bleeding and ERF, in patients who underwent concomitant palliative treatment with SEMS and brachytherapy (37383940). Park et al. (36) showed that the rate of ERF was significantly lower in patients who underwent SEMS removal within 6 weeks as compared to after 6 weeks of starting radiation therapy (6% vs. 30%; P = 0.030). However, randomized controlled trials are needed to confirm this finding.
SEMS placement as a bridge to surgery
In patients with stage IIA or IIB esophageal cancer (localized resectable disease), neoadjuvant chemotherapy or chemoradiotherapy before surgery is recommended (41). However, a substantial period of time is required to relieve dysphagia by neoadjuvant chemotherapy or chemoradiotherapy. SEMS placement has been increasingly used as a “bridging therapy” to surgery, improving dysphagia and allowing for oral nutrition during neoadjuvant therapy (29). However, according to recent studies, the use of SEMS placement as bridging therapy has a negative impact on oncological outcomes (424344). Mariette et al. (43) reported in their cohort of 2,944 patients that those who underwent SEMS placement as bridging therapy had a lower median time to recurrence (7 vs. 9 months; P = 0.040) and a lower 3-year overall survival rate (25% vs. 44%; P = 0.023). The following reasons have been suggested in an attempt to explain the negative outcomes associated with SEMS placement as a bridge therapy: First, mechanical injury caused by SEMS results in fibrosis that compromises the resectability of the tumor; Second, SEMS placement increases the levels of circulating neoplastic cells; Third chemotherapy increases the incidence of SEMS-related complications, such as migration and ERF; and Fourth, accurate restaging of the tumor after SEMS placement is technically difficult (454647). Therefore, some investigators argue that the placement of a feeding tube or percutaneous gastrostomy may be preferable over SEMS placement as a bridging therapy (4849). It should be noted, however, that in the study of Mariette et al. (43), SEMS was not removed until just before surgery; this factor may be the main reason for the negative outcomes. Several authors have reported that SEMS removal 4–6 weeks after starting neoadjuvant chemotherapy or chemoradiotherapy seems to decrease fibrosis and SEMS-related complications (353650). However, randomized controlled trials are needed to confirm this result.
Palliative treatment for malignant ERF
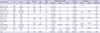
ERF (i.e., tracheoesophageal and bronchoesophageal fistula) are common complications of esophageal cancer, with incidence rates of 5%–26% (515253). This condition is caused by direct tumor invasion or as an adverse event of cancer therapies and can lead to malnutrition and respiratory failure. Therefore, prompt palliative treatment to seal off the fistula is considered a key priority in patients with this condition. Several studies have shown that covered SEMS are highly efficacious in their ability to seal off fistulas, with a success rate of 67%–100% (515455565758596061626364656667). In addition, some studies report that patients with fistulas experience improved quality of life after covered SEMS placement (6364). However, in some cases in which covered SEMS placement in the esophagus alone cannot not seal off the fistula, covered SEMS placement in both the esophagus and airway may be required (68). The clinical outcomes of SEMS placement for malignant ERF in the literature are summarized in Table 2.
Table 2
Clinical outcomes of SEMS placement for malignant ERF in the literature
| Author (reference) | Year | Country | No. of patients | Mean age, yr | Sex (M/F) | SEMS type | SEMS placement location | Treatment success | Complications | Median survival, day | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Esophagus | Airway | Both | Major | Minor | |||||||||
| Saxon et al. (54) | 1995 | USA | 12 | 61.0 | 9/3 | FC | 12 (100.0) | 0 | 0 | 8 (66.7) | 3 (16.0) | 0 | 117.0 |
| Morgan et al. (55) | 1997 | England | 20 | 60.3 | 12/8 | - | 20 (100.0) | 0 | 0 | 18 (90.0) | - | - | 65.3 |
| Low et al. (56) | 1998 | USA | 12 | 59.8 | 7/5 | FC | 12 (100.0) | 0 | 0 | 11 (91.7) | - | - | 93.0 |
| May and Ell (57) | 1998 | Germany | 11 | 58.0 | 10/1 | FC | 11 (100.0) | 0 | 0 | 10 (90.9) | 0 | 6 (54.5) | 121.0 |
| Siersema et al. (58) | 2001 | Netherlands | 16 | 66.4 | 12/4 | FC, PC | 16 (100.0) | 0 | 0 | 14 (87.5) | 4 (25.0) | 5 (31.3) | 58.0 |
| Wang et al. (59) | 2001 | USA | 33 | - | - | - | 33 (100.0) | 0 | 0 | 31 (93.9) | - | - | 134.0 |
| Sarper et al. (60) | 2003 | Turkey | 14 | - | - | PC | 14 (100.0) | 0 | 0 | 12 (85.7) | 0 | 0 | 49.0 |
| Shin et al. (51) | 2004 | Korea | 61 | 59.3 | 58/3 | FC | 55 (90.2) | 5 (8.2) | 1 (1.6) | 49 (80.3) | 14 (23.0) | 12 (19.7) | 94.0 |
| Murthy et al. (61) | 2007 | USA | 12 | 64.0 | 9/3 | FC, PC | 5 (41.7) | 4 (33.3) | 3 (25.0) | 12 (100.0) | 1 (8.3) | 0 | - |
| Ross et al. (62) | 2007 | USA | 21 | - | - | FC | 21 (100.0) | 0 | 0 | 19 (90.5) | - | - | 72.0 |
| Hu (63) | 2009 | China | 17 | 56.8 | 15/2 | FC | 17 (100.0) | 0 | 0 | 16 (94.1) | 2 (11.8) | 6 (35.3) | 93.0 |
| Herth et al. (64) | 2010 | Germany | 112 | 54.3 | 98/14 | PC | 37 (33.0) | 65 (58.0) | 10 (8.9) | 112 (100.0) | 7 (6.3) | 0 | 261.0 |
| Van Heel et al. (65) | 2010 | Netherlands | 15 | - | - | FC, PC | 15 (100.0) | 0 | 0 | 14 (93.3) | 5 (33.3) | 0 | 73.0 |
| Chen et al. (66) | 2012 | China | 30 | 51.2 | - | PC | 25 (83.3) | 0 | 5 (16.7) | 26 (86.7) | 0 | 14 (46.7) | 125.0 |
| Zori et al. (67) | 2014 | USA | 10 | - | - | FC | 6 (60.0) | 1 (10.0) | 3 (30.0) | 7 (70.0) | - | - | - |
| Total | - | - | 396 | 57.2 | 230/43 | - | 299 (75.5) | 75 (18.9) | 22 (5.6) | 359 (90.7) | 36 (12.0) | 43 (14.3) | 144.6 |
SEMS = self-expanding metallic stents, ERF = esophagorespiratory fistula, FC = fully covered, PC = partially covered.
![]()
CONTRAINDICATIONS
In the early days of SEMS placement, several conditions were considered to be contraindications, including cervical esophageal strictures < 2 cm from the upper esophageal sphincter and malignant esophageal strictures lacking a proximal “shelf” to prevent migration (6970). However, advancements in SEMS have made a great contribution to the management of malignant esophageal strictures in patients for whom treatment has traditionally proved technically difficult (71). Currently, there is no consensus on absolute contraindications for SEMS placement, but careful patient selection is important. SEMS placement is commonly considered contraindicated in terminally ill patients with a life expectancy of < 4 weeks, distal obstruction, perforation, bowel ischemia, sepsis, or uncorrectable coagulopathy (72).
COMPLICATIONS
Complications of SEMS placement can be classified as early or delayed. Early complications occur immediately or within 2–4 weeks after SEMS placement and include foreign body sensation, pain, gastroesophageal reflux, migration, bleeding, and perforation. Prolonged chest pain has been reported in up to 14% cases after SEMS placement, and is more common in the cervical esophagus (5373). For this reason, SEMS with small diameters have been developed for placement in the cervical esophagus (71). Small amounts of bleeding during and 1–2 days after SEMS placement occurs in 5% patients; however, major bleeding requiring intervention occurs in < 1% patients (53). Several studies reported that perforation during or soon after SEMS placement occurred in < 1% patients (275374). Perforations appear to occur more frequently in patients who were previously treated with chemo and/or radiation therapy; “full-thickness” perforation, which requires surgical intervention, is very rare (74). Delayed complications are more common than early ones and are defined as complications that occur at least 2–4 weeks after SEMS placement, including migration, tumor ingrowth and overgrowth, food impaction, and ERF. Although early complications are decreasing because of recent advances in SEMS and delivery systems, delayed complications still occur in up to 65% patients, with a re-intervention rate as high as 50% (3). Among both early and delayed complications, migration is the most common complication, occurring at a rate of 7%–75% (27). Tumor ingrowth is very rare nowadays because of the widespread use of FCSEMS but can still occur if the covering membrane is degraded or detached from the stent (53). In contrast, tumor overgrowth is still a common delayed complication, occurring in about 5% patients following SEMS placement (53). Food impaction also occurs in about 5% patients (53). In contrast, only a few cases of SEMS-related ERF have been reported in the literature, suggesting that this delayed complication is very rare (75767778). Complications of SEMS placement can also be classified as major and minor. Major complications are life-threatening conditions such as ERF, bleeding, and perforation; minor complications are those that are not life-threatening, including migration, tumor ingrowth and overgrowth, and food impaction (3212223242526272829303132333435363738394041424344454647484950515253545556575859606162636465666768).
FUTURE OF SEMS
Since the patients with incurable esophageal cancer have a very poor prognosis, the ideal palliative treatment for malignant esophageal strictures should provide rapid and durable relief of symptoms, result in few complications, require minimal hospital stay, and prolong survival. However, patients who underwent SEMS placement often failed to achieve long-term relief of symptoms due to stent malfunction and have to be admitted again for reintervention. In addition, palliation with SEMS only provides symptoms relief but does not prolong survival. Radioactive SEMS has recently been described to combine the advantages of SEMS placement (i.e., quicker relieve of dysphagia) and brachytherapy (i.e., survival advantage and better quality of life) (798081). Zhu et al. (79) showed in their recent multicenter randomized control trial that placement of SEMS loaded with radioactive seeds could result in a modest prolongation of survival in patients with incurable esophageal cancer (177 vs. 147 days; P = 0.005). Several drug-eluting SEMSs are also under development and have shown the potential to inhibit tumor growth in animals (808182).
SUMMARY
SEMS placement is a widely accepted method for treating malignant esophageal strictures and ERFs. A wide range of SEMS for esophageal cancer is available in Korea, and even more are available internationally. Knowledge of the advantages and disadvantages associated with different designs will aid physicians in selecting the optimal SEMS for a given condition. The outcomes of SEMS placement do not differ with respect to the guidance method used (endoscopic and/or fluoroscopic). Brachytherapy provides a survival advantage and a better quality of life than does SEMS placement for palliating malignant esophageal strictures but requires more time to relieve dysphagia. SEMS removal within 6 weeks of starting radiation therapy may decrease complications. If SEMS is not removed 4–6 weeks after starting neoadjuvant chemotherapy or chemoradiotherapy, it may have a negative impact on oncological outcomes. Radioactive and drug-eluting SEMSs may potentially be the future of palliative treatment for malignant esophageal strictures.
 XML Download
XML Download