

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Drug-eluting stents (DESs) have markedly reduced in-stent restenosis (ISR) and repeat revascularizations (12). However, in spite of the use of DESs, percutaneous coronary intervention (PCI) is still associated with stent failure and is related to stent thrombosis or restenosis (34), which in turn may be related to fatal clinical events. Thus, it is important to investigate the pathological mechanisms of stent failure. Although several factors for stent failure have been reported, one of the main mechanisms is neoatherosclerosis (NA), i.e., the de novo development of atherosclerosis within the neointimal region (5).
This article discusses the prevalence, predictors, and clinical implications of NA observed by optical coherence tomography (OCT).
OCT AND NA
OCT-defined NA
NA is defined as atherosclerotic changes in neointimal tissue. It was firstly described in pathologic specimens with bare metal stents (BMSs), and also recently reported in DES (5). It is characterized by the presence of clusters of lipid-laden foamy macrophages with or without necrotic core formation and/or calcification within the neointimal tissue of stented segments. Histological examination can be used for diagnosis; however, it can be difficult to obtain pathologic specimens. Therefore, several intra-coronary imaging modalities, including intravascular ultrasound (IVUS) and OCT, can be used to evaluate coronary stents, particularly the mechanisms of stent failure. Current guidelines recommend IVUS or OCT to assess the mechanisms of stent failure (67). However, compared to IVUS, OCT is preferred over IVUS due to the resolution capacity (80–120 vs. 10–20 µm), and OCT is better for evaluating neointimal tissue within the stented segment. OCT can provide detailed information regarding restenotic tissue (tissue structure, backscatter, microvessels, and composition) (8910). Therefore, it can be used to visualize distinct morphological characteristics of NA, such as macrophage infiltration, lipid accumulation, in-stent calcification, or neointimal rupture.
On OCT images, OCT-defined NA is mainly confined to lipidic or calcific neointima (1112). Lipidic neointima is shown as diffusely bordered, signal-poor regions with overlying signal-rich bands. Calcific neointima shows well-delineated, signal-poor regions with sharp borders (1314). Fig. 1 presents the lipidic and calcific neointima defined by OCT evaluation.
Prevalence and predictors of NA
Several studies used OCT to examine the prevalence and risk factors of NA. Table 1 summarizes the prevalence of OCT-based NA. The prevalence varies, according to the stent type, the follow-up duration, and clinical indications. Takano et al. (9) evaluated neointimal characteristics after BMS implantation at early (< 6 months, n = 20) and late (≥ 5 years, n = 21) phases, using OCT. Lipid-laden neointima was not observed in the early phase, whereas it was observed at the late phase (67% of the patients). Habara et al. (15) compared neointimal characteristics between early (≤ 1 year) and late restenosis within BMS (> 5 years), and showed that the heterogeneous appearance of neointima was more frequent in late restenosis compared with early restenosis (61% vs. 6%). Thus, after BMS implantation, the prevalence of NA increased with the stent age. Similarly, after DES implantation, stent age is a major predictor of NA. We previously reported on the serial changes (9 months and 2-year follow-up after DES implantation) of neointima characteristics in DES-treated lesions using OCT (16). Lipid-laden neointima (27.6% vs. 14.5%, P = 0.009) and thin-cap neoatheroma (13.2% vs. 3.9%, P = 0.070) were more frequently detected at 2-year follow-up compared with 9 months of follow-up. In addition, the change of neointimal morphology from homogeneous to heterogeneous or a lipid-laden pattern was observed in 30% of cases. Kang et al. (17) investigated 50 patients who presented with stable (n = 30) or unstable angina (n = 20) with DES restenosis using OCT, and found lipid-containing neointima in 90% of lesions. Twenty-six lesions (52%) had thin-cap fibroatheroma (TCFA)-containing neointima and 29 lesions (58%) had at least one in-stent neointimal rupture. In addition, when we analyzed a total of 212 DES-treated patients (second-generation DES, 52.4%) with > 50% neointimal cross-sectional area (CSA) stenosis that were retrospectively enrolled from the Korean multicenter OCT registry, the incidence of NA increased with stent age (18). NA was found in 1.6% (1/64) of the lesions identified in less than 1 year. In comparison, NA was observed in 73.9% (17/23) of the lesions over 7 years (18).
Table 1
Prevalence, predictors, and clinical implication of OCT-based NA

| Authors | Year | Subjects | Stent type and number of lesions | Duration | Prevalence | Predictors of NA | Clinical implication |
|---|---|---|---|---|---|---|---|
| Takano et al. (9) | 2009 | Patients with OCT follow-up | BMS, n = 21 | ≥ 5 yr | 67% | - | - |
| Kang et al. (17) | 2011 | Symptomatic patients with ISR lesions and intimal hyperplasia > 50% of stent area | 1st and 2nd DES, n = 50 | Median, 32 mon | 90% | - | Patients with unstable angina (vs. stable angina) had more unstable OCT findings. |
| Kim et al. (16) | 2012 | Patients with serial OCT follow-up at 9 mon and 2 yr | 1st DES, n = 43; and 2nd DES, n = 33 | 9 mon; and 2 yr | 15%; and 28% | - | - |
| Yonetsu et al. (12) | 2012 | Patients with OCT follow-up and mean neointimal thickness > 100 µm | BMS, n = 73; DES, n = 106 | Mean, 26.9 mon | 47% | Stent age, DES vs. BMS, smoking, CKD, no use of ACEi/ARB | - |
| Ko et al. (31) | 2012 | Patients with VLST after DES implantation | 1st and 2nd DES, n = 18 | 42 mon | 22% | Time to OCT study | - |
| Lee et al. (34) | 2013 | Patients with OCT follow-up and > 50% CSA neointimal stenotic lesions | BMS, n = 24; DES, n = 128 | Median, 70.7 mon | 35.5% | Stent age, use of first-generation DES, and hypertension | NA was associated with higher TLR (93% vs. 78%) and higher stent thrombosis (15% vs. 0%). |
| Kim et al. (26) | 2015 | Patients with OCT follow-up (≤ 12 mon) and mean neointimal thickness > 100 µm | 1st and 2nd DES, n = 482 | ≤ 12 mon, early neoatherosclerosis | 6% | Hypertension, pre-stent LDL-cholesterol ≥ 130 mg/dL | NA was associated with higher clinical symptoms (13% vs. 57%) and higher TLR (9% vs. 55%). |
| Lee et al. (18) | 2015 | Patients with > 50% neointimal CSA stenosis | 1st DES, n = 101; and 2nd DES, n = 111 | 55 mon; and 12 mon | 46%; and 11% | CKD, LDL-cholesterol at follow-up more than 70 mg/dL, stent age | NA was associated with a higher acute coronary syndrome (19.0% vs. 3.9%). |
| Kuroda et al. (27) | 2016 | Patients with OCT follow-up > 1 yr after stent implantation | BMS, n = 37; DES, n = 277 | > 1 yr | 17% | LDL-cholesterol, CRP levels at follow-up | NA was associated with a higher MACE (composite of death, myocardial infarction, and TLR) (37% vs. 9%). |
OCT = optical coherence tomography, BMS = bare metal stent, ISR = in-stent restenosis, DES = drug-eluting stent, CKD = chronic kidney disease, ACEi = angiotensin converting enzyme inhibitor, ARB = angiotensin-II receptor blocker, VLST = very late stent thrombosis, CSA = cross-sectional area, NA = neoatherosclerosis, TLR = target-lesion revascularization, LDL = low-density lipoprotein, CRP = C-reactive protein, MACE = major adverse cardiovascular event.
![]()
With regard to stent type, DES might be associated with a higher risk of NA, compared with BMS, and Yonetsu et al. (12) evaluated NA predictors, where all subtypes of DES were found to be independent predictors of NA compared with BMS. Similarly, Ali et al. (19) reported that prior DES vs. BMS (odds ratio [OR], 7.0; P = 0.006) was a predictor of NA. However, among the DES cases, second-generation DES was not found to be more protective against NA compared with the first-generation DES (18). Additionally, NA was observed earlier in DES-treated lesions compared with BMS-treated lesions based on the results of a pathologic study (5). A possible explanation for the higher risk of NA with DES vs. BMS could be that the inhibition of neointimal hyperplasia by local drug delivery causes delayed coverage and dysfunction of endothelial cells. Although endothelial cells could be barriers that prevent lipid infiltration and inflammatory cell migration, incomplete maturation of the regenerated endothelium was more frequently observed in DES vs. BMS (2021). Considering these suggested mechanisms, although these metallic stents have been related to NA, bioresorbable vascular scaffolds could be expected to reduce NA. The recovery of vasomotion in the scaffolded segment was noted after bioresorbable vascular scaffold implantation, and a signal-rich layer separated the potentially thrombogenic plaque components from the lumen; this suggests a favorable long-term healing response with potential plaque sealing, which was observed in a recent OCT follow-up study (2223). Furthermore, no cases of necrotic core accumulation of adluminal origin were observed (24).
This study did not evaluate whether the initial OCT findings at the index PCI can predict the development of NA at follow-up OCT, and the presence of unstable underlying lesion morphology was found to be a significant risk factor of NA based on autopsy cases (5). Nakazawa et al. (5) reported that stent struts embedded in the necrotic core, where the effect of the drug likely persists for a long period of time, potentially causes dysfunctional and/or incompetent endothelium, which can lead to the development of NA. Similarly, Tian et al. (25) found that NA was more frequently associated with adjacent lipid plaque at follow-up OCT. Therefore, the plaque character can be determined by pre-procedural OCT and can be used as a predictor of NA.
Although one of the strongest risk factors of NA is a longer time interval to follow-up, when we used OCT to evaluate the incidence of NA that developed after short post-DES implantation durations, early NA was also observed in 6.4% of 482 DES-treated lesions within 12 months after stent implantation (at a median post-implantation follow-up of 9.1 months) (26). Independent predictors of early NA were hypertension (OR, 3.20; P = 0.010) and pre-stent low-density lipoprotein (LDL) cholesterol ≥ 130 mg/dL at the time of index procedure (OR, 3.89; P = 0.002). Other clinical predictors of NA are also summarized in Table 1. Yonetsu et al. (12) assessed 179 stents (mean duration, 26.9 months; DES, 59%) and reported OCT-detected NA (lipid-laden neointimal and/or calcification within the neointima) in 84 lesions (47%). In this study, independent determinants of OCT-detected NA were current smoking, chronic kidney disease (CKD), and absence of angiotensin-converting enzyme inhibitors or angiotensin II receptor blockade usage. We also analyzed the restenotic lesions with first-generation DES (n = 101) and second-generation DES (n = 111), and found CKD and LDL cholesterol at follow-up with values that were more than 70 mg/dL, which were both independent predictors of NA. From the Kobe University Hospital OCT registry (175 patients, 314 lesions), Kuroda et al. (27) found that C-reactive protein (CRP) level (OR, 1.022; P = 0.001) and LDL cholesterol (OR, 1.022; P = 0.008) at follow-up were independently associated with the presence of NA. Although the exact mechanisms need to be investigated further, these results additionally support the postulated mechanism of NA; that is to say, oxidative stress and inflammation lead to atherosclerotic changes inside neointima (1226). These findings support the importance of secondary prevention after stent implantation.
CLINICAL IMPLICATION OF NA: ISR AND STENT THROMBOSIS
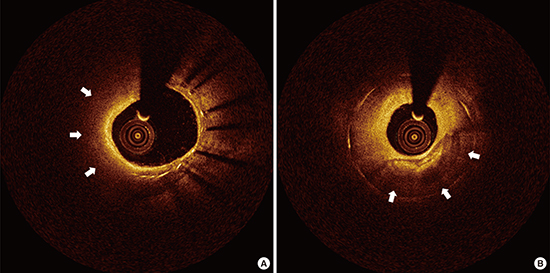
Recent studies with OCT suggest that NA may play an important role in late stent failure, both for ISR and stent thrombosis. Vergallo et al. (28) reported that the mean neointimal thickness was independently associated with the presence of NA (OR, 2.53; P < 0.001). This association was independent from stent type and time from implantation, suggesting a possible pathologic link between the 2 processes, neointimal thickness and NA. Similarly, after DES implantation, late ISR and very late ISR were associated with NA, suggesting that these could contribute to the late catch-up phenomenon after DES (29). Additionally, recent OCT findings in patients with late and very late stent thrombosis (VLST) reported a high prevalence of plaque rupture and impaired healing (30313233). According to a prospective multicenter registry, ruptured neoatherosclerotic lesions were more frequent with BMS than with DES (36% vs. 14%, P = 0.005), and late/VLST were mainly related to malapposition (31%) and NA (28%) (32). Therefore, NA may contribute to both ISR and stent thrombosis. Neoatherosclerotic OCT images in patients that presented with ISR and stent thrombosis are shown in Fig. 2.
 | Fig. 2OCT images of neoatherosclerotic neointima in patients with ISR (A) and stent thrombosis (B). (A) Lumen is narrow for NA in a patient with ISR. (B) Disrupted neointima (arrows) with thrombi (arrowheads) is observed in a patient with stent thrombosis.
ISR = in-stent restenosis, NA = neoatherosclerosis.
|
Patients with NA had higher chances of symptoms or need of repeat vascularization (Table 1) (34). We evaluated the neointimal characteristics of 152 lesions (128 DESs and 24 BMSs) with > 50% CSA neointimal stenosis. NA was observed in 54 lesions (35.5%, 35 DESs and 19 BMSs), and patients with NA vs. without NA had a higher rate of target lesion revascularization (92.6% vs. 77.6%, P = 0.018) and stent thrombosis (14.8% vs. 0%, P < 0.001) (34). Similarly, from the Korean multicenter OCT registry, patients with NA showed a higher rate of acute coronary syndrome at follow-up OCT (19.0% vs. 3.9%, P = 0.001) (18). In addition, based on data from the Kobe University Hospital OCT registry, the incidence of major adverse cardiovascular events (MACEs; e.g., composite of death, myocardial infarction, and target-lesion revascularization [TLR]) was significantly higher in patients with NA vs. those without NA (36.9% vs. 9.3%, P < 0.001). This was mainly driven by an increase in the rate of cardiac death (6.5% vs. 0%, P = 0.017) and TLR (30.4% vs. 7.7%, P < 0.001). Moreover, the incidence of stent thrombosis (definite/probable) was significantly higher in patients with NA (6.5% vs. 0%, P = 0.017) (27). Patients with early NA (within 12 months after stent implantation) also had a higher incidence of clinical symptoms (13% vs. 57%, P < 0.001) and had undergone a higher frequency of TLR (9% vs. 55%, P < 0.001) at the time of OCT follow-up (26).
Clinical presentation of NA can vary from asymptomatic or stable angina to life-threatening acute coronary syndrome because of stent thrombosis. Compared to patients with stable angina, patients with unstable angina show higher incidences of unstable OCT findings, including TCFA-containing neointima, neointima rupture, and thrombus (P = 0.027) (17). OCT-defined rupture of lipidic neointima was observed in patients with VLST (31).
In addition, when treating ISR, the neointimal characteristic of ISR lesions, particularly NA, could impact the periprocedural myocardial injury. We analyzed a total of 125 patients with ISR lesions (35). Post-PCI creatine kinase-myocardial band (CK-MB) elevation was observed in 20 (16.0%) patients, and multivariate analysis revealed that the maximum length of segments with NA (OR, 1.463; P = 0.011) and TCFA (OR, 14.328; P = 0.041) were independent predictors for post-PCI CK-MB elevation. Thus, NA may underlie the vulnerability of neointima to PCI, with a distal microembolization of neointimal debris.
Although routine OCT examination is not necessary for all patients who undergo follow-up angiography, the data from these studies indicates that OCT examination can be valuable for patients with symptoms and angiographically-significant stenosis. For these patients, OCT examination can determine the presence of NA for future risk stratification and can be useful for evaluating the mechanism of stent failure for targeted therapeutic approaches. Additional studies are needed to determine whether these results can be translated to clinical improvements.
CONCLUSION
Recent evidence has indicated that NA is a considerable mechanism of late/VLST and restenosis. In addition, it is an important substrate for future adverse events. Thus, detection of NA by OCT and identification of morphological characteristics, including in-stent lipidic or calcific neointima, is helpful for predicting and preventing greater future adverse events.
 XML Download
XML Download