

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Syphilis is generally considered to be largely eradicated in many countries; however, its incidence remains high in the developing world and is increasing in developed countries (12). Syphilis continues to affect pregnant women, despite the numerous control measures established for its prevention. The World Health Organization (WHO) has estimated that nearly 1 million pregnant women worldwide are infected with syphilis annually (3). According to current data from the Korea Centers for Disease Control and Prevention, the rates of syphilis and congenital syphilis (CS) were 1.42 cases per 100,000 population and 0.05 cases per 100,000 live births in 2014 (4).
CS is caused by transplacental transmission of Treponema pallidum from mother to fetus or during birth by contact with maternal lesions. Untreated syphilis during pregnancy has a > 70% probability of transmission rate (5). Transmission in utero causes the widest dissemination of spirochetes into the fetus and fetal or perinatal death occurs in 40% of affected infants (5). About two-thirds of live born infants are asymptomatic at birth, and symptoms usually present during the neonatal period. In the absence of treatment, symptoms develop within weeks or months. Overt renal disease is rare in patients with CS. Syphilitic renal involvement may vary from mild transient proteinuria (6) to more significant disease such as nephrotic syndrome (NS) or nephritis (7). Hence, it is important to be familiar with its symptoms and signs. Physicians should be aware of the various clinical features of syphilis to enable early diagnosis. We report a case of CS in a 2-month-old infant who presented only with NS.
CASE DESCRIPTION
In February 2015, a 2 months old male baby was admitted to the hospital with gross hematuria and generalized edema. He was born at term with an uncomplicated perinatal course and normal growth. The mother was a 27 years old Korean who had regular prenatal care. He had been healthy until the week before admission. Brown urine had developed 7 days prior to admission, and intermittent edema was detected after birth. At that time, his height was 56.5 cm (3–5th percentile), weight was 6.4 kg (25–50th percentile), and head circumference was 38.5 cm (10–25th percentile). A general physical examination revealed mild soft tissue edema and a distended abdomen without hepatosplenomegaly. There were no mucocutaneous symptoms such as skin eruption, desquamation, or snuffles and no limitations in the movement of extremities.
Complete blood cell counts demonstrated normocytic normochromic anemia (hemoglobin, 8.0 g/dL and hematocrit, 24.7%) with leukocytosis (white blood cells [WBC], 26,600/mm3). Serum electrolytes, liver, and renal function tests were within normal ranges. His C-reactive protein was elevated (8.4 mg/dL), and total protein and albumin levels were low (3.8 and 1.4 g/dL, respectively). Urinalysis revealed 4+ proteinuria, erythrocytes, and WBCs. The urinary protein/creatinine ratio was 62.5. Congenital nephrotic syndrome (CNS) was diagnosed and cause of CNS include congenital infection was evaluated at the first day of admission. Serologic tests for rubella, herpes simplex virus, and toxoplasmosis were all negative. He was positive for cytomegalovirus (CMV) immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies. However, CMV was not observed in culture and polymerase chain reaction analysis of urine and blood. Antinuclear antibody was positive with a cytoplasmic pattern, but anti-dsDNA and anti-Smith antibodies were negative and accompanied by normal complement levels. On the fourth day, a rapid plasma reaction (RPR) test and blood venereal disease research laboratory (VDRL) test were positive with titers of 3.4 RPR unit and 1:16, respectively. Despite no other symptoms of syphilis, a treponemal test was performed to confirm the diagnosis. The T. pallidum hemagglutination assay (TPHA) was reactive at a dilution of 1:1,280 and fluorescent-treponemal antibody-absorbed test was also reactive. Cerebrospinal fluid showed a normal cell count and protein level; however, the VDRL and TPHA were positive. Radiographs of both limbs disclosed symmetric single-layer periosteal reaction. Cranial ultrasonography was normal, and neurological examination including hearing test was normal. After diagnosing CS, his mother was tested for syphilis, and her RPR was positive at 24 RPR units. Nevertheless, the mother showed no specific symptoms. The results of her routine antenatal screening test were positive for syphilis; no treatment was done due to hospital error.
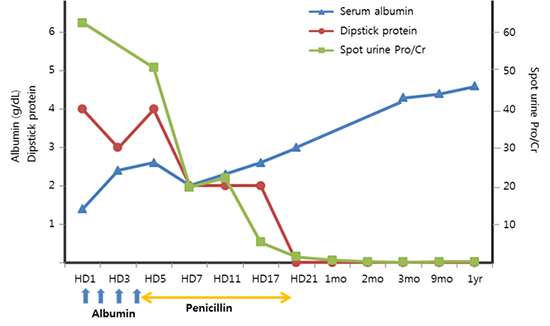
The baby was treated with penicillin G for 15 days. His anemia improved slowly during 2 weeks of hospitalization. In addition, his total protein and albumin levels increased slowly to 5.0 and 3.0 g/dL, respectively. Proteinuria and hematuria improved within several days. The VDRL titer decreased from 1:16 to 1:8 during treatment. No CMV IgG antibody was detected at the 2-week follow up, so it was considered transplacental transmission during pregnancy. Renal biopsy was not performed because of the remission of proteinuria.
Follow-up at 12 months after discharge, baby showed normal growth and development. His urinalysis result was normal with a normal level of albumin, and the RPR was non-reactive.
DISCUSSION
CNS is a relatively rare disorder that might be caused by several diseases. The majority of cases are caused by genetic mutations, but infections are a possible cause of CNS, particularly in developing countries. CS has long been known to cause CNS in newborns (5). However, syphilis prevalence decreased with the advent of penicillin in the 1940s. Since the initiation of national programs to prevent CS, it was considered a disease of the past in developed countries. Despite the marked advances in the management and control of syphilis, the incidence of syphilis is increasing again in many parts of the world (1238).
CS occurs when the spirochete T. pallidum crosses the placenta from an infected mother to the fetus during pregnancy or at birth by contact with maternal lesions (7). Intrauterine infection can result in still birth, hydrops fetalis, or prematurity. As clinical symptoms of CS vary, it is important to be familiar with the symptoms. Approximately two-thirds of live-born neonates with CS are asymptomatic at birth. If untreated, most infants develop symptoms within the first 5 weeks of life. Clinical symptoms are divided into early signs that occur during the first 2 years of life and late signs that develop later over the first 2 decades of life (7). The earliest sign of CS is usually nasal discharge that occurs 1–2 weeks before the rash appears. Other early stigmata include maculopapular rash, fever, hepatosplenomegaly, and bone involvement, particularly diaphyseal periostitis or metaphyseal osteochondritis. Late sign of CS develops as a result of scarring or persistent inflammation and gumma formation in various tissues. Symptoms manifest in approximately 40% of infants born to mother with untreated syphilis during pregnancy.
Renal manifestations of syphilis have been known since the 18th century (9). Significant renal involvement is infrequent in cases of CS and may vary from simple albuminuria to nephritis or NS. The incidence rate of CNS in CS range from 0.5% (10) to 2.4% (11). It has been considered to result from direct invasion of the kidney by spirochetes or secondary to a hypersensitivity reaction. Immune complex deposition has been implicated in the pathogenesis of NS associated with syphilis (1213). Development of immune complex glomerulonephritis may be affected by the degree of antigenic exposure and antibody response. Eradication of the antigen after anti-syphilitic therapy may result in prompt disappearance of renal abnormalities and their non-recurrence (14). In a recent year, Shim et al. (15) reported the CS infant with NS, however, the baby had typical skin lesion such as maculopapular rash, and desquamation. Although our patient fulfilled the criteria for congenial syphilitic nephropathy with unequivocal evidence of CS in the patient, evidence of syphilis in the mother, absence of any other etiology for CNS (14), he had no other symptoms of syphilis. This report emphasizes the importance of screening for syphilis in CNS even if symptoms are lacking for a diagnosis of syphilis.
The number of reported CS cases has increased in Korea according to the sentinel surveillance system started in 2001. A total of 94 cases were reported from 2001 to 2010; however, 99 cases were reported between 2011 and 2014 (8). It has been inferred to be an anthropological change paralleling the rebound increase in CS incidence. Kang et al. (8) revealed that about 20% of serologically positive mothers are foreign-born immigrants, and Park et al. (16) also reported that CS was significantly higher among immigrant mothers. Immigrant mothers may have a low socioeconomic background and may not have access to prenatal care, thus, increasing incidence of CS in immigrant mothers could be related to failure of prenatal care delivery systems (91617). A rising trend in the incidence of syphilis and CS has also been observed in other Asian and Western countries (12181920). A sharp increase in the incidence of syphilis infection has been documented among heterosexual population and men who have sex with men. The rates of syphilis infection in men who have sex with men range from 18% in a 2014 Thai study (19) to 61% in a 2014 US report (20). Increased incidence of syphilis in men could result in the transmission of syphilis to their wives and then children. Inadequate prenatal care and increased number of syphilis cases both have the potential to affect increases in the incidence of CS.
The CS is a preventable disease; however, its incidence has increased in the last 10 years. Therefore, clinicians still consider CS in the differential diagnosis of CNS due to the worldwide resurgence of syphilis.
 XML Download
XML Download