

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Tropical storms including hurricanes, typhoons and cyclones significantly impact human populations and result in public health consequence including storm related mortality, injury and psychosocial effects (1). Rapid health needs assessment tools have been used to assess resources required for decision making during the disaster recovery phase (2345678). Based on information from rapid health and need assessments after disasters, policy makers and stakeholders can identify the public health status of damaged areas and support optimal health care interventions to the affected victims.
The United States' Centers for Disease Control and Prevention (CDC) developed a rapid needs assessment tool named the Community Assessment for Public Health Emergency Response (CASPER) (910111213). This tool has been used 53 times from 2003 to 2012 to assess needs following disasters (12). CASPER suggests multistage cluster sampling to select households to interview and recommends a standardized survey process within 72 hours. CASPER samples households based on a system of addresses which is not feasible to other nations. Furthermore, both different types of structures and types of disasters could be barriers to implement rapid need assessment tools developed from advanced countries.
The Korean Centers for Disaster Control and Prevention (KCDC) developed a rapid need assessment toolkit optimized to addresses and characteristics of administrations, infrastructure and disaster response systems in Korea. We benchmarked the advantages of previously developed toolkits from advanced countries and modified these to the disaster response system of Korea. The KCDC conducted pilot trials using the Public Health Assessment for Emergency Response (PHASER) toolkit after 2 different typhoons struck Korea during summer 2012.
In this study, we developed the rapid health need assessment toolkit optimized for weather related disasters in Korea. The goal of this study was to assess the public health needs following typhoons in both urban and rural areas in Korea, 2012.
MATERIALS AND METHODS
Study design
This was a prospective observational study that used the PHASER toolkit developed by the KCDC. We conducted pilot trials using the PHASER toolkit to assess health needs following typhoons in Paju and Jeju during the summer of 2012.
Development of PHASER protocol
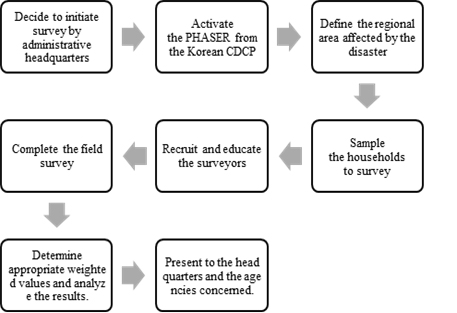
The KCDC developed the PHASER toolkit. The PHASER toolkit focused on a rapid health needs assessment after weather related disasters including but not limited to typhoons, floods, heat waves, and freezing temperatures. We developed the formal process of PHASER; decision to initiate survey, administrative collaboration, education for interviewers, data collection and statistical analysis, and feedback to stakeholders. We used question banks optimized for weather related disasters and standardized survey registry, tracking sheets, and informed consent forms. We also developed methodology to sample interviewees following the disasters using methods for expanded programs on immunization.
According to the PHASER protocol, the administrative headquarters in a region affected by a disaster requests activation of the PHASER survey from the KCDC. The KCDC will then dispatch a specialized PHASER survey team to the disaster area. The PHASER team will define the regional area affected by the disaster and sample the households to survey. The PHASER protocol recommends to survey 400 households at the province level and 200 household at the county level. The PHASER team will then recruit and educate the surveyors. After completing the survey, the PHASER team determine appropriate weighted values and analyze the results. Finally, within 72 hours from initiation of the survey, reports from the PHASER survey are presented to the headquarters of the damaged areas and the agencies concerned.
Selection of participants: preparation of PHASER
We studied Paju and Jeju for the use of PHASER surveys following typhoons to these areas in June and September 2012. In May 2012, meetings were conducted between the KCDC and disaster preparedness administrators in Korea. We utilized the enumeration areas developed by the Statistics Korea for the Korea census survey as the first step of the multistage cluster sampling method.
Following the disasters and according to PHASER protocol, 200 households in Paju and 400 households were surveyed on Jeju. If adults at the selected household was unavailable at the time of the PHASER survey, the household was excluded from the survey. All households excluded from the survey were replaced by a similar household based on a previously prepared list of substitute households.
Method of measurement
In June and again in September 2012, the KCDC activated the PHASER survey following typhoons in Paju and Jeju. After each typhoon, both the KCDC and the study authors visited the damaged regions and initiated the surveys.
We used 2 standardized survey forms including both a household tracking sheet and a household survey sheet. The tracking sheets included information on the number of households sampled or substituted, reasons to substitute a sampled household, types of household structure (e.g., apartment or house). The household survey forms included questionnaires on the number of individuals living in the house (including the number of children under 2 years of age and over 65 years of age), and the damage and the structural safety of the actual house. We additionally surveyed the availability of resource for daily life including toilet, telephone (landline and mobile capacity), gas, electrical power, elevator functionality, water availability, and garbage removal. We additionally evaluated resources required to satisfy basic health needs including food, medical service, transportation, and physical or financial support to restore destructed resources. We surveyed the clinical results of the disaster in the sampled household including the occurrence of either disease or injury, requirement for medical services, and the presence of psychiatric symptoms occurring after the disaster (e.g., attention disorder, sleeping disorder, etc.). Finally, we assessed the accessibility of medical services and prescription drug to use for 3 to 7 days after the typhoon.
All surveyors completed a 4-hour survey training course before initiating the PHASER survey. Surveyors in Paju were nurses and officers working at public health center. On the other hand, surveyors in Jeju were nursing school students. After finishing their assigned surveys, each interviewer returned to the command center. At that time, all tracking sheets and survey forms were reviewed by KCDC and the researchers for checking the accuracy of their visiting to the sampled households and the correctness of their substitution.
Outcome measurement
The primary outcomes were the clinical results (the occurrence of either disease or injury, requirement for medical services, and the presence of psychiatric symptoms occurring after the disaster) and accessibility of medical services after typhoon. The secondary outcomes were the resources required to satisfy the health needs for daily life. We assessed the outcomes descriptively and also calculated the weighted value of each question to evaluate estimated overall damage of each region affected by the typhoon.
Statistical analysis
Households were sampled for each affected region. The PHASER sampling methodology included a multistage cluster design. In the initial stage, we selected 40 enumeration districts for a county (Paju city) and 80 enumeration districts for a province (Jeju island). In the first sampling stage, the selection of enumeration districts reflects the proportion of types of houses in the damaged areas. In the second stage, we selected 5 households in each enumeration districts. Thus, 200 households were selected from the county region (Paju) and 400 households from the province (Jeju).
Descriptive statistics were used to assess performance and operation of PHASER. We measured the response rate defined as the number of households responded to surveyors divided by the number of households visited to interview. We additionally measured the cooperation rate as the number of households that completed the PHASER survey divided by number of households visited to interview.
We conducted a descriptive analysis for all surveyed items. We additionally calculated the weighted value for each questionnaire based on the sampling criteria of each region. We assessed the number and percentage of each question and present with 95% confidence intervals (CIs).
RESULTS
From August 26 to 28 2012, typhoon Bolaven impacted to Paju and Jeju. Maximal wind velocity for 10 minutes was 45 meter per second (100 miles per hour) and the central minimum pressure was 910 hectopascal.
On August 30, 2012, Paju and Jeju were again struck by a typhoon. Typhoon Tembin had a maximal wind velocity for 10 minutes was 45 meter and a central minimum pressure of 945 hectopascal.
Operation of PHASER for Paju and Jeju
PHASER research team and KCDC visited Paju on August 31, 2012. Initially, we conducted the surveyor training program. We recruited 20 surveyors and created 10 survey teams composed of 2 surveyors each. Each survey team was assigned 20 households to survey. Following training completion, the PHASER survey began at 1:00 pm, and all surveyors finished surveying at 6:00 pm on August 31. In Paju, interviewers visited 812 households (Table 1), 238 households had surveys attempted (response rate 29.3%) and 190 households successfully completed the survey (cooperation rate 79.8%).
Table 1
Performance and operation of PHASER for Paju and Jeju

PHASER = Public Health Assessment for Emergency Response.
*Response rate = (No. of households attempted face to face interview/No. of total households visited to interview) × 100; †Cooperation rate = (No. of households completed PHASER survey/No. of households attempted face to face interview) × 100.
Jeju was surveyed on September 1, 2012. Similar to Paju, we recruited 50 surveyors and created 25 survey teams each composed of 2 interviewers. We designated these survey teams to 400 households. After a similar morning training program, the survey teams visited the sampled households and completed survey by 9:00 pm on September 1, 2012. On Jeju, interviewers visited 1,237 households, attempted to interview 436 households (response rate 35.2%) and completed surveys at 386 households (cooperation rate 88.5%).
Available resources and health needs for daily life
In Paju, most resources for daily life functioned well except elevator (4.2% were unavailable). In contrast, the proportion of answer unavailability for electrical power was 21.6% (95% CI, 14.7%–28.6%) and elevator was 14.0% (95% CI, 9.1%–18.8%) in Jeju(Table 2).
Table 2
Unavailable resources for daily life in Paju and Jeju
Survey results for the required resources to satisfy health needs for daily life are presented in Table 3. In Paju, 10.0% (95% CI, 4.6%–15.4%) of house lacked electrical power indicating 2,805 households (95% CI, 1,276–4,334) required electrical power. In Paju, 9.5% needed water supply and 2.6% required medicines. In Jeju 4.9% of surveyed households lacked electrical power indicating 5,496 (95% CI, 2,240–8,752) households were without electrical power. Food was lacking in 4.4% households indicating 4,857 (95% CI, 1,543–8,171) households in the surveyed area were without food.
Table 3
Required resources to satisfy health need for daily life in Paju and Jeju
Clinical results and accessibility of medical services
Injured patients were identified in 0.5% (95% CI, 0.0%–1.5%) of households in Paju and 1.5% (95% CI, 0.3%–2.7%) of households in Jeju (Table 4). No mortality was detected. A need for medical services was identified in 2.7% (95% CI, 1.1%–4.4%) in Jeju, indicating 3,048 (95% CI, 1,188–4,908) households required medical care. In Paju, cognitive disorders were identified in 12.8% (95% CI, 5.0%–20.7%) and sleeping disorders in 6.8% (95% CI, 2.8%–10.8%) of households. In Jeju, sleeping disorder were identified in 17.4% of households indicating 19,338 (95% CI, 14,228–24,449) households with sleeping disorders. In Paju, 12.1% of interviewees had a barrier to medical service and 12.8% of Jeju interviewees had a barrier to medical service access (Table 5).
Table 4
Clinical outcomes affected by the typhoon in Paju and Jeju
Table 5
Accessibility of medical service in Paju and Jeju
DISCUSSION
We conducted a pilot trial of a rapid need and health assessment tool following a weather-related disaster using the PHASER toolkit developed by the KCDC. In summer 2012, Korea was struck by 2 typhoons, Bolaven and Tembin, within almost a week. We demonstrated the ability to complete PHASER surveys in both Paju and Jeju immediately after the typhoons. Both Paju and Jeju were identified as having a substantial electrical power requirement. No mortality was identified and both disease and injury occurrences were rare. In relatively advanced countries with well-developed social infrastructures and structurally sound buildings, injuries or worsening of disease status is likely rare.
Sleeping disorders, however, were identified in 6.8% of households in Paju and 17.4% of households in Jeju. Thus, psychiatric support to relieve psychiatric problems was necessary in both region after the typhoons.
Previous investigations also report psychiatric problems following natural disasters (614). After hurricane Ivan, the United States CDC conducted a rapid need assessment and the most common self-reported health problem was sleep disturbances in 54% of respondents (6). As natural disasters can result in psychiatric stresses, preparation for such problems is needed following natural disasters. To reduce mental health problems after a disaster, several reports recommend development and application of the psychological first aid program (151617). The PHASER survey clearly demonstrated that support of mental health services was necessary for both regions.
We utilized a multistage cluster sampling method based on the World Health Organization's expanded immunization program which is still used for immunization programs in developing countries (181920). The CASPER toolkit uses a system of country level addresses and recommends selecting 30 census blocks and 7 households. In Korea, a different system of addresses and a high proportion of high rise structures are barriers to implementation of the CASPER toolkit. Korean administrative officers, the KCDC, disaster medicine researchers, epidemiologists, and a statistician reviewed and benchmarked the concept of a 2 stage cluster sampling method based on the World Health Organization's expanded immunization program (181920). And we modified the sampling method using enumeration area units from the Statistics Korea as a sampling unit to implement the toolkit efficiently into disaster response system and address systems of Korea. The development of the rapid need assessment tools optimized for specific country nuances would best assess disaster response needs. In Korea, 24 tropical cyclones and 5 local windstorms were reported from 2000 to 2009 (21). At the report, 264 victims and 26 mortality cases were observed. PHASER toolkit optimized for disaster response system in Korea could useful to assessed medical resource need during such meteorological disasters.
During PHASER survey, securing recent geographic information and accessing enumeration area unit database was difficult. Acquisition of accurate recent information about change of roads or reconstruction of apartments is crucial to sample appropriate households to interview. And enumeration area unit data was managed by the Statistics Korea to take a census. Therefore, unofficial access and use of the enumeration area unit data was not permitted for layperson. To perform a 2 stage cluster sampling and assign the sampled households to interviewers efficiently, rapid acquisition of accurate geographic information and enumeration area unit data is important. To overcome this barrier, collaboration of PHASER survey team, KCDC and local administrative was helpful. The KCDC coordinated the official access to the enumeration area unit database. And then, we conducted a 2 stage sampling and selected households. After the process, the local administrative and local surveyors confirmed the appropriateness of selected households based on their recent geographic information such as apartments complex redevelopment.
This study has certain limitations. Measurements of health status by the PHASER survey is based on the self-report of the interviewee. Detailed assessment and diagnosis by medical professionals was not performed and accuracy of health status by the self-report method is a limitation. We recruited nursing students to serve as surveyors in Jeju. In Paju, nurses and community health center administrative officers were recruited. We trained the surveyors, but skill between reviewers may not have been consistent. Finally, this trial was pilot to implement the PHASER survey tool. Although we collected appropriate data, the results were not connected to community interventions to improve recovery after the typhoons.
In conclusion, we performed a pilot assessment of the PHASER toolkit to rapidly assess the needs of citizens for Paju and Jeju following typhoons Bolaven and Tembin in 2012. A substantial number of households had sleep disorders.
 XML Download
XML Download