

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Sebaceous carcinoma (SC) is a rare malignant neoplasm that arises from the adnexal epithelium of sebaceous glands (1). Most SCs develop de novo and present as a highly aggressive form, although they may originate from benign sebaceous neoplasms. The most common clinical presentation is a painless, slowly enlarging subcutaneous nodule; however, SC may exhibit various colors and morphology depending on its site of origin. SCs have been traditionally classified into 2 groups: ocular type and extraocular type (2). SC can histologically be classified into well-, moderately, or poorly differentiated depending on the degree of differentiation and cellular atypia. The clinical presentation and histopathology of SC are so diverse that the diagnosis can often be missed.
In Koreans, limited data are available on the clinical and histopathological characteristics of patients with SCs, particularly the extraocular type. Herein, we analyzed 29 patients with histopathologically proven SC at Chonbuk National University Hospital. The goal of this study was to evaluate the clinical and histopathological characteristics of both ocular and extraocular SC in Koreans.
MATERIALS AND METHODS
Between January 2001 and October 2014, 29 patients were histologically diagnosed with SC at Chonbuk National University Hospital. Their medical records and pathologic slides were reviewed retrospectively.
Clinical features
The following clinical data were obtained: age, sex, location, duration, tumor size and color, lymph node (LN) and distant metastasis, treatment modalities, and recurrence. T staging for the primary tumor was evaluated based on the American Joint Committee on Cancer tumor, node, and metastasis (TNM) staging (3).
Histopathological features
Our histopathological review mainly focused on the degree of differentiation, overall growth patterns, cell types, and intraepithelial spread. The histological classification was based on Font's classification: well-differentiated, moderately differentiated, or poorly differentiated tumors (1). Prominent patterns of infiltrative growth were categorized into lobular, papillary, trabecular, and others. The existence of comedonecrosis showing total cellular dissolution in the centers of lobular lesions was also assessed. The infiltrative cell type was categorized into epidermoid, basaloid, basosquamous, and others. We also assessed whether there was pagetoid intraepithelial spread.
RESULTS
Demographic data
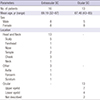
Of the 29 patients who were diagnosed with SC, 16 were identified as having extraocular SC and 13 as having ocular SC (Table 1). The mean age at presentation was 69.19 ± 37.19 (range, 32–87) years for patients with extraocular SCs and 67.46 ± 24.46 (range, 43–85) years for patients with ocular SCs. Both extraocular and ocular SCs occurred most commonly in the 8th decade. The second most common age group was the 7th decade (Fig. 1). There was no sexual difference in the frequency of extraocular SC occurrence; however, ocular SC had a female preponderance (8/13, 61.54%). The eyelid (13/29, 44.83%) was the most common site of SC. The most common site of extraocular SC was the scalp (5/16, 31.25%), followed by the cheek (3/16, 18.75%) and temple (2/16, 12.50%). The other locations were the forehead, nose, neck, axilla, forearm, and scrotum. The most common site of ocular SC was the upper eyelid (7/13, 53.84%), followed by the lower eyelid (4/13, 30.77%).
Table 1
General information of 29 patients with SC
![]()

Clinical findings
The clinical data are shown in Tables 2 and 3. Differently colored tumors were observed. Of the 16 extraocular SCs, 7 were pink (43.75%), 3 were flesh colored (18.75%), 2 were red (12.50%), 2 were brown (12.50%), and 2 were yellow (12.50%) (Fig. 2). Yellow tumors were the most common in ocular SCs (7/13, 53.85%), followed by flesh colored (3/13, 23.08%) and pink (1/13, 7.69%). Off-white colored tumors were only found in ocular SCs (2/13, 15.38%) (Fig. 3). Four extraocular SCs were associated with bleeding.
Table 2
Clinical characteristics of patients with extraocular SC
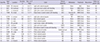
SC = sebaceous carcinoma, Rt. = right, Lt. = left, ND = not described, SCC = squamous cell carcinoma, BCC = basal cell carcinoma, EMPD = extramammary Paget's disease, LN = lymph node, WLE = wide local excision, MMS = Mohs micrographic surgery.
![]()
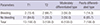
Table 3
Clinical characteristics of patients with ocular SC

SC = sebaceous carcinoma, Rt. = right, Lt. = left, ND = not described, SCC = squamous cell carcinoma, BCC = basal cell carcinoma, WLE = wide local excision.
![]()
 | Fig. 2Clinical presentations of extraocular SC. (A) Light-pink hard nodule on the forehead. (B) Deep-brown crusted nodule on the right cheek. (C) Light-brown nodule on the right parietal scalp. (D) Light-pink hard nodule with ulceration on the scrotum. (E) Red pedunculated nodule with ulceration on the left cheek. (F) Flesh-colored crusted plaque on the left neck.
SC = sebaceous carcinoma.
|
 | Fig. 3Clinical presentations of ocular SC observed using slit-lamp biomicroscopy. (A) Yellow papule on the left upper eyelid. (B) Yellow confluent papules on the conjunctival side of the right upper eyelid. (C) Flesh-colored papule on the right upper eyelid. (D) Off white-colored nodule on the left caruncle.
SC = sebaceous carcinoma.
|
Squamous cell carcinoma (SCC; 6/16, 37.50%) was the most common clinical diagnosis for extraocular SCs, and chalazion (7/13, 53.85%) was the most common diagnosis for ocular SCs. Distant metastasis was not observed in any patient, and only one patient with extraocular SC showed metastasis to a cervical LN. Most of the patients with extraocular SCs had tumors in stage T1 (13/16, 81.25%) and the rest had tumors in stage T2 (3/16, 18.75%); however, patients with ocular SCs had tumors in various T stages (T1: 1/13, 7.69%; T2a: 8/13, 61.54%; T2b: 3/13, 23.08%; and T3a: 1/13, 7.69%).
The extraocular SCs were resected via Mohs micrographic surgery (MMS) with a 2-mm margin (first MMS, 9/16, 56.25%) and wide local excision (WLE) with a 5–6-mm margin (WLE, 7/16, 43.75%). Most of the ocular SCs were removed by WLE with a 5–6-mm margin (12/13, 92.31%). The patients were followed-up for an average of 32.06 months (range, 2–60 months) for extraocular SC and 30.46 months (range, 4–60 months) for ocular SC after surgery. During the follow-up period, there was no recurrence or death reported.
Histopathological findings
Details of the main histological features are shown in Table 4. The poorly differentiated tumor type was most commonly observed in both extraocular (7/16, 43.75%) and ocular (5/13, 38.46%) SCs. In extraocular SC, moderately differentiated and well-differentiated types were found in 6 (37.50%) and 3 patients (18.75%), respectively. In ocular SC, moderately differentiated and well-differentiated types were evenly distributed (n = 3, 23.08% for each) (Fig. 4A-C).
Table 4
Histopathologic findings of SC

![]()
 | Fig. 4Histopathological observation of SC. (A) Well-differentiated SC with sebocyte-like tumor cells (H & E, × 100). (B) Moderately differentiated SC (H & E, × 100). (C) Poorly differentiated SC with fine stippling of the nuclear chromatin and few mitoses present (H & E, × 200). (D) Lobular pattern of infiltrative growth with central necrosis (H & E, × 100). (E) Trabecular pattern of infiltrative growth, and the inset shows an epidermoid dyskeratosis (H & E, × 100; inset, × 400). (F) Papillary pattern of infiltrative growth with unencapsulated margins (H & E, × 100). (G) Tumor cells surrounded by layers of basaloid cells (H & E, × 100). (H) Epidermoid infiltrative cell type with nonkeratinizing cells within a large lobule manifesting nonvacuolated eosinophilic cytoplasm with scattered pleomorphic nuclei in a comedonecrosis pattern (H & E, × 100). (I) Basosquamous infiltrative cell type with lobules composed of small cells with scant eosinophilic cytoplasm (H & E, × 100). (J) Intraepithelial tumor cells with a pagetoid spreading pattern (H & E, × 100).
SC = sebaceous carcinoma, H & E = hematoxylin and eosin.
|
The majority of prominent patterns of infiltrative growth were lobular (Fig. 4D) in both extraocular (11/16, 68.75%) and ocular (10/13, 76.92%) SCs. A trabecular pattern (Fig. 4E) was observed in 3 extraocular and 1 ocular SCs, and a papillary pattern (Fig. 4F) was observed in only 2 extraocular SCs. Comedonecrosis was found in 6 extraocular (37.50%) and 3 ocular (23.08%) SCs. Basaloid cells (Fig. 4G) were the most common infiltrative cell type in both extraocular (9/16, 56.25%) and ocular (8/13, 61.54%) SCs. Epidermoid or squamous cell types (Fig. 4H) were found in 5 extraocular (31.25%) and 3 ocular (23.08%) SCs. A basosquamous cell type (Fig. 4I) was found in only 2 extraocular SCs (12.50%) and pagetoid intraepithelial spread (Fig. 4J) was found in 2 extraocular (12.50%) and 3 ocular (23.08%) SCs.
DISCUSSION
SC is very rarely diagnosed in clinical settings because its presentation is similar to that of other benign and malignant lesions, and making a histological diagnosis is not easy because of its rarity and the difficulty in determining the sebaceous differentiation of tumor cells (4). In the literature, it has been called a sebaceous gland carcinoma, a sebaceous cell carcinoma, and a Meibomian gland carcinoma; however, recently, SC has been accepted as the commonly used term (2). The literature regarding SC is insufficient, although there have been many published studies, including a recent retrospective review of 1,349 SC cases from the Surveillance, Epidemiology, and End Results (SEER) database of the National Cancer Institute in the US (5). Very limited data in Korea are available for patients with SC and for the extraocular type in particular, and the data available consists primarily of single case reports (6-18). We analyzed 29 cases of SC, which is the largest number of Korean SC cases reported in a study to date.
Our data are consistent with previous studies reporting that SCs primarily occur in the skin of the eyelid or in the extraocular skin of the head and neck region, where sebaceous glands are more concentrated (51920). The predilection for the upper eyelid is believed to be related to the relatively greater number of modified sebaceous (Meibomian) glands that are present in the upper eyelids (21). Although it has been reported that ocular SC occurs equally between the sexes and extraocular SC is more common in men (22), our study showed a female predominance in ocular SC, an equal sex distribution in extraocular SC, and a slight female predominance in the entire cohort. SC associated with Muir-Torre syndrome has been rarely reported, and no such patient was included in our study (2324).
Since the known risk factors for SC include Asian ethnicity, SC has been thought to have a higher incidence in Asian countries (3). However, a recent review of the SEER data demonstrated that there was no Asian predominance in the overall incidence of SC (5). This may be attributed to the relatively small number of other skin malignancies in Asians, such that SC seems to have a higher incidence. There are currently no data available on the incidence of SC in Korea. To determine the exact incidence of SC in Korea, multi-institutional data collection involving large referral centers is required.
The clinical presentation of SC is varied depending on the location of the lesion. Extraocular SC usually appears as a painless pink or yellow nodule; however, it can also present as flesh-colored to red papules, plaques, or nodules (3). Bleeding associated with SC was reported in approximately one-third of the cases in previous studies (125); however, in our study only 25% (4/16) of patients with extraocular SC showed bleeding from the tumor. Only 15.4% (2/13) of patients with stage T1 disease and 66.7% (2/3) with T2 disease presented with bleeding. Three had a moderately differentiated type (3/6, 50%), and 1 case was a poorly differentiated type (1/7, 14.3%) (Table 5). Intraepithelial spread was not observed in all 4 cases. However, we were not able to identify a significant relationship between bleeding and aggressive behavior because there were too few patients in this study.
Table 5
Analysis of bleeding of tumor according to T levels and pathologic types of extraocular SC
![]()
The clinical differential diagnosis of extraocular SC includes various neoplastic conditions such as basal cell carcinoma (BCC), SCC, amelanotic melanoma, Merkel cell carcinoma, and cutaneous lymphoma, or non-neoplastic benign sebaceous conditions such as nevus sebaceus, xanthoma, and sarcoidosis (3). Ocular SC, usually appearing as a yellow or pink painless nodule, is easily mistaken for a chalazion, which is a benign mass, and this can cause delays in diagnosis and appropriate treatment. Other conditions to be considered while establishing a diagnosis include blepharitis, conjunctivitis, keratoconjunctivitis, BCC, SCC, and other benign sebaceous neoplasms (26). A skin biopsy should be performed in every case that is suspected to be SC, in particular when recurrent chalazion, eyelid thickening, lash loss, lid eversion, or ulceration of the eyelid are present (27). In our study, the most frequent clinical diagnoses of extraocular SC and ocular SC were SCC and chalazion, respectively.
SC has been reported to be an aggressive tumor, and metastasis and mortality rates have been reported to be as high as 29% in some series (2528293031). However, a recent study of the 2009 SEER database (5) has reported a rate of regional LN involvement of 1.3%, and an involvement of distant or unspecified LNs in only 0.4% of cases. Among our 29 patients, only 1 patient with extraocular SC showed regional LN involvement (3.4%), and no distant metastasis or death during the follow-up period was observed. This suggests that, contrary to widely held assumptions, SC might not be aggressive in most cases. Our case with cervical LN metastasis showed moderately differentiated, lobular and basaloid SC, and a lack of intraepithelial spread. The size of the lesion was 1.2 cm (T1), and it was associated with bleeding. However, these features cannot be considered significant, because there was only one case.
The staging of SC is different according to its location based on the American Joint Committee on Cancer TNM classification guidelines for non-melanoma skin cancers (32). The role of TNM staging for extraocular SC for predicting prognosis and management has not been studied; however, the relationship between TNM staging and disease progression has recently been validated by a retrospective cohort study of ocular SC. Stage T2b disease or higher T category in ocular SC can be predictive of nodal metastasis, and T3a disease or higher T category can be predictive of cancer specific mortality (33). Four of our patients with ocular SCs had tumors at stage T2b or higher; however, there was no nodal metastasis. Extraocular SC has been thought to be less aggressive than ocular SC, consistent with the findings of our study that indicate that ocular SC has a higher average T stage than extraocular SC.
Based on the degree of differentiation, SC can be classified into 3 categories: well-, moderately, or poorly differentiated (34). Previous studies have shown variable results with regard to these categories (135), and in our study, approximately 40% of tumors were classified as poorly differentiated. Commonly recognized histological patterns of infiltrative growth include lobular, papillary, and trabecular. The most common pattern in our study was the lobular pattern; this result is consistent with those of previous studies. The lobules may vary in size within the same tumor, and some lobulated tumors can display central necrosis (comedonecrosis). This specific finding is described as foci of exaggerated holocrine secretion rather than true necrosis.
The main cell types encountered in SC are basaloid, basosquamous, and epidermoid (36). Although mixtures of various types may be observed in the same specimen, only the dominant cell type was recorded in our study, and we found the most common infiltrative cell type was basaloid in both ocular and extraocular SCs. The basaloid type corresponds to the outer germinal cells of the secretory alveoli with scant cytoplasm, and it shows a strong hematoxylinophilia and a high nuclear-to-cytoplasmic ratio. In the epidermoid cell type, more visible eosinophilic cytoplasm may be observed, and it may display scattered dyskeratotic cells or nonkeratinizing cellular whorls (1). The basosquamous cell type displays intermediate cytoplasmic features of the basaloid and epidermoid types and more copious cytoplasm than basaloid cell type (36). Ocular lesions often show a pagetoid pattern in the overlying conjunctiva or epidermis of the eyelid (2537). This feature was observed in one-third of all cases in one series (38). Such changes are very rarely seen in extraocular SC; however, these changes were observed in the ocular SCs (3 cases) as well as extraocular SCs (2 cases) in our study.
Immunostaining, including BerEP4, ADP, EMA, p53, Ki-67, and adipophilin staining for cytoplasmic lipids, is useful in diagnosing SC and differentiating it from SCC and BCC. Recently, staining for the androgen receptor was reported to be useful in diagnosing SC (39). Further studies using immunohistochemistry are warranted in Korea.
Surgical resection with WLE is the standard therapy for SC; however, MMS may have lower recurrence rates and maximal tissue conservation. A surgical margin of 5–6-mm in WLE is commonly recommended for SCs, and a 2-mm margin in MMS has been reported to be effective (40). Although more studies comparing the long-term outcomes of MMS vs. WLE are necessary, MMS is recognized as the best initial treatment modality for SC (39). Both WLE and initial MMS in our study showed excellent results.
SC often masquerades as an inflammatory disease or other tumors in both clinical and histological findings, leading to misdiagnosis and delays in proper management. A comprehensive clinicopathologic analysis of both ocular and extraocular SC has not yet been performed in Korea. Although this retrospective study has a small sample size and is limited to a single center, we expect this study to make a significant contribution to the diagnosis and management of SC in Korea.
 XML Download
XML Download