

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breast cancer is one of the most common cancers in women worldwide, accounting for 25% of all new cancers (1). In Korea, breast cancer is the highest-ranking type of cancer among registered female patients, and the incidence of breast cancer in females has also continued to increase (2).
Many women who survive breast cancer experience a range of diseases and chemotherapy-related problems, including vasomotor symptoms, decreased psychosocial functioning, and reduced health-related quality of life (QOL) (34). Several studies have reported that almost 50% of women experienced depression and/or anxiety up to 12 months after chemotherapy (5). Studies that have examined the rates of clinically significant anxiety and depression in women for breast cancer have found a difference between the preoperative and postoperative periods (67). For example, Van Esch et al. (8) reported that 33% of breast cancer patients experienced anxiety symptoms before they received a treatment, and 15% reported anxiety symptoms after surgery. Furthermore, the anxiety prevalence rate after cancer recurrence was 45%. Goldberg et al. (9) have documented that 32% of women diagnosed with breast cancer experience major or minor depression before treatment, while 24% of these patients reported depression following treatment. In a Korean study focused on breast cancer patients after treatment, 31% of women had symptoms of depression and anxiety after completion of chemotherapy (10). Palliative therapy for patients with breast cancer has been the focus of investigation due to the need for better postoperative care and to control the adverse effects of chemotherapy (1112).
To reduce the adverse effects of chemotherapy and to support psychological well-being for patients with breast cancer, a variety of trials have been conducted, including cognitive behavioral therapy and stress management intervention for problems associated with breast cancer (41314). Several studies have revealed significant results that physical activity (PA) can reduce the clinical symptoms of breast cancer and improve QOL, physical functioning (15), depression (16), and anxiety (12). Furthermore, PA might be associated with a reduction in the recurrence rate and an increase in disease-free breast cancer survival (1718).
However, few studies have investigated the relationship between PA intensity and health status in patients with breast cancer (19). Observational evidence suggests that a moderate level of PA reduces the risk of death from breast cancer (19). Some researchers have recommended that a suitable type of exercise would combine both aerobic and resistance exercise and would consist of one session involving muscular resistance and 2 moderate-intensity aerobic sessions per week, with each session lasting 30–40 minutes (1520).
In the current study, we aimed to investigate the correlation between PA level and mental health status in a population-based sample of Korean female patients with breast cancer. We hypothesized that the intensity and frequency of PA in patients with breast cancer would be lower than those observed in healthy controls. The secondary hypothesis was that even less intense physical activities would improve the physical and psychological health status of patients with breast cancer compared to those of healthy control participants.
MATERIALS AND METHODS
Participants
A total of 92 patients with metastatic breast cancer were enrolled from Chung-Ang University Hospital. All participants had an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0–2; objective measurable disease; and adequate bone marrow, hepatic, cardiac, and renal function. Inclusion criteria were as follows: 1) female with breast cancer, and 2) 18–60 years of age. There were 3 exclusion criteria: 1) current or history of medical disease, 2) history of psychiatric disease, and 3) history of substance abuse (Table 1). Of the 92 patients with breast cancer, 76 were clinical stage IV, 5 were clinical stage I, 4 were clinical stage II, and 2 were clinical stage III. In addition, 5 did not complete the tests. To increase patient homogeneity, we included the data of the 76 patients with breast cancer, clinical stage IV. Fifty age- and sex-matched healthy control participants were asked to complete the same scales as those used in the experimental group. Six healthy controls did not complete the tests, ultimately resulting in 76 breast cancer patients and 44 healthy controls for our analysis.
Table 1
Demographic characteristics
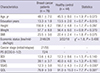
Data are mean ± SD.
BMI = body mass index, PS = performance status, ECOG = Eastern Cooperative Oncology Group, BDI = Beck Depression Inventory, STAI = State-Trait Anxiety Inventory, SSAS = Somatosensory Amplification Scale, QOL = quality of life, SD = standard deviation.
*P < 0.050; †P < 0.001.
![]()
PA and mental health status assessment
International Physical Activity Questionnaire (IPAQ)-Korean
PA in patients with breast cancer and also in healthy controls was assessed using the Korean version of the IPAQ, short form (2122). The participants were asked to report both moderate and vigorous PA performed during the previous 7 days. This 7-item inventory utilizes a series of yes or no and fill-in-the-blank questions to assess the time spent per week engaged in various types and intensities of PA. Each activity and intensity score is provided a metabolic equivalent (MET) according to the published manual (e.g., MET for walking = 3.3, moderate intensity = 4.0, vigorous intensity activity = 8.0) (2324). A higher score indicates a greater PA level, and the Cronbach's α and test-retest reliability of the IPAQ after translation into Korean were previously reported as 0.65 (22).
Beck Depressive Inventory (BDI)
The depression status of patients with breast cancer and that of the healthy controls were measured with the Korean version of the BDI, a widely used, 21-item self-report questionnaire that covers the major features of depression (25). The BDI yields a total score that ranges between 0 and 63, with higher scores reflecting more severe levels of depression. The inventory was translated into Korean and checked by back-translation into English by another translator. The Cronbach's α and test-retest reliability of the IPAQ after being translated into Korean have been previously reported as 0.91 (26).
Spielberg State-Trait Anxiety Inventory (STAI)
The anxiety status in patients with breast cancer and healthy control participants was measured using the Korean version of the STAI (27). This scale included a total of 40 items, 20 of which describe trait anxieties and 20 that detail state anxieties. The scale has been translated into Korean and has shown internal consistency and reliability, with a Cronbach's α = 0.91 for state and Cronbach's α = 0.82 for trait anxieties.
Somatosensory Amplification Scale (SSAS)
The Korean version of the SSAS was used to assess the tendency to experience somatic sensations as intense, noxious, and disturbing (28). This scale contains 10 items designed to measure the extent to which people are somatically sensitive; a high score indicates a greater tendency to intensify normal somatic sensations (29). The Cronbach's α and test-retest reliability of the SSAS after being translated into Korean have been previously reported as 0.75 (28).
QOL scale
The Korean version of the QOL scale was used to measure the QOL in patients with breast cancer and in healthy control participants (30). The 26-item QOL scale contains 5 subscales: overall domain, physical health domain, psychological domain, social relationships domain, and environmental domain. The Cronbach's α and test-retest reliability of the SSAS after being translated into Korean have been previously reported as 0.90 (30).
Statistical analysis
Differences between groups in terms of age, education, economic status, and physical fitness (including height, weight, and body mass index [BMI]) were analyzed using an independent t-test or the χ2 test. These tests were also used to assess PA and mental health status. The correlation between PA and mental health status was analyzed with Pearson correlation or Spearman correlation. For all statistical analyses, the significance level α was set at 0.05. To control for multiple comparisons in the correlation between each PA and that participant's mental health status, the significance level α was set at 0.01 (0.05/5, for each PA and 4 factors of mental health). All analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographic characteristics
The 2 groups were generally well-matched at baseline with regard to key demographic and anthropometric variables (Table 1). Specifically, there were no statistically significant demographic differences between the groups about age (t = 1.9; P = 0.073), years of education (t = 0.7; P = 0.515), height (t = 1.7; P = 0.097), weight (t = 0.9; P = 0.370), BMI (t = 1.8; P = 0.075), and economic status (χ2 = 1.83; P = 0.400). No statistically significant mental status differences were noted between groups on the BDI (t = 1.48; P = 0.140) or STAI (t = 1.3; P = 0.193). However, there were statistically significant differences between the scores of SSAS (t = 2.2; P = 0.030) and QOL (t = 7.7; P < 0.001).
Comparison of PA between patients with breast cancer and healthy controls
There was statistical significance in the differences in level and frequency of PA and MET between breast cancer patients and healthy controls (Table 2). Specifically, scores of vigorous (t = 2.8; P = 0.010), moderate (t = 10.6; P < 0.001), and low (t = 4.7; P < 0.001) intensity PA in breast cancer patients were significantly lower than those of the healthy controls, respectively. Moreover, the frequency of moderate PA in breast cancer patients was significantly lower compared with that of healthy controls (t = −2.6; P = 0.011). In turn, the frequency of low PA in breast cancer patients was significantly higher than that in healthy control participants (t = 2.85; P = 0.005).
Table 2
The comparison of PA between patients with breast cancer and healthy control
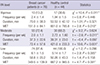
Data are presented as number (%) or mean ± SD.
PA = physical activity, MET = metabolic equivalent, SD = standard deviation.
*P < 0.010; †P < 0.001.
![]()
Correlations between PA intensity and mental health status
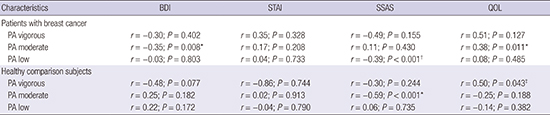
There were significant correlations between PA level and mental health status within breast cancer patients and healthy controls (Table 2). In breast cancer patients, a moderate level of PA was inversely correlated with BDI score (r = −0.35; P = 0.008) and positively correlated with QOL score (r = 0.38; P = 0.011). In contrast, a low level of PA was inversely correlated with SSAS score (r = −0.39; P < 0.001)(Table 3). In healthy control participants, a vigorous level of PA was positively correlated with QOL score (r = 0.50; P = 0.043), while a moderate level of PA was inversely correlated with SSAS score (r = −0.59; P < 0.001)(Table 3).
Table 3
Correlations between PA level and mental health status

PA = physical activity, BDI = Beck Depression Inventory, STAI = State-Trait Anxiety Inventory, SSAS = Somatosensory Amplification Scale, QOL = quality of life.
*P < 0.010; †P < 0.001; ‡P < 0.050.
![]()
DISCUSSION
Based on our findings, somatosensory amplification in patients with breast cancer was higher than that in healthy participants. At the same time, QOL scores in patients with breast cancer were lower than the scores for the healthy controls. These findings are in agreement with a large number of previous studies in breast cancer survivors (3132) and are also consistent with published studies that have reported that breast cancer survivors have severe concerns about disease recurrence and experience body change stress after breast surgery (3334).
Not surprisingly, PA in breast cancer patients demonstrated significantly lower MET scores and lower intensity than healthy participants. These findings agree with those of Rogers et al. (12), who reported that domestic or gardening activities and moderate intensity tasks accounted for the largest percentage of total energy expenditure among rural breast cancer survivors.
In accordance with our primary hypothesis, we found that the intensity of PA was significantly correlated with several mental health factors. Interestingly, our results revealed that a moderate or low level of PA improved depression, somatosensory amplification, and QOL in patients with breast cancer, while vigorous PA intensity enhanced somatosensory amplification and QOL in healthy participants.
Interestingly, Holmes et al. (19) have suggested that a moderate level of PA would be beneficial compared to a highly vigorous level of PA because the former would be associated with circulation of ovarian hormones (35). Additionally, lower estrogen levels have been linked to increased survival in patients with breast cancer (3637).
In fact, women with breast cancer who follow the Centers for Disease Control and Prevention recommendations for all individuals in the United States to exercise at moderate intensity for 30 or more minutes per day on 5 or more days per week might experience more effective breast cancer treatment (38). In contrast, vigorous activity has been linked to an increased risk of upper respiratory tract infection due to the associated reduction in immune function (39) and therefore might be less beneficial than moderate activity for breast cancer patients (19). Although few studies have supported this hypothesis, proper PA was associated with lower levels of circulating ovarian hormones (37) and lower levels of estrogen (39), which can explain the positive effects in breast cancer patients.
However, it is still controversial whether the intensity of PA affects mental health in breast cancer patients. In fact, the American Cancer Society Guidelines suggest that adults should engage in at least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity activity each week (40). This difference might be associated with the inconsistent of effect of PA reported by prior studies and the fact that the most effective intensity, frequency, and type of exercise are currently unknown (15). The findings of the present study suggest that future research is needed to advance the effort to correlate PA with the mental health status of breast cancer patients.
There were several limitations of the current study. First, this study only included patients with clinical stage IV breast cancer. Second, the cross-sectional research design of the study precluded the full observation of the time effects of PA in breast cancer patients. A longitudinal observational design would be better equipped to show the cause-effectiveness of PA. Future studies with a large number of participants and longitudinal long-term follow-up are needed.
Based on the results of the current study, breast cancer patients who engage in regular PA had significantly lower MET scores and frequencies of moderate intensity than healthy participants. However, a moderate or low intensity of PA was inversely correlated with depression and somatosensory amplification and was positively correlated with QOL in breast cancer patients. Finally, we recommend that progressively low-to-moderate doses of PA could be well adapted to produce positive effects on mental health status in breast cancer patients.
 XML Download
XML Download