

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Subarachnoid hemorrhage (SAH) is a devastating, although uncommon, type of stroke with high morbidity and mortality rates (1). Preclinical studies have shown that therapeutic hypothermia (TH) is a promising treatment for ischemic stroke, and large-scale studies are currently examining the effects of hypothermia on the outcome of ischemic stroke (234). However, hypothermia as a treatment for hemorrhagic stroke is not fully understood. There is limited experimental and clinical evidence that TH effectively improves the clinical outcome for patients with SAH, except for a reduction in intracranial pressure (56789). Induced hypothermia during aneurysm surgery is currently not routinely recommended, but may be a possible option in patients with good-grade aneurysmal SAH (10).
There are currently insufficient data to draw any conclusions on the benefits of TH, particularly in patients with poor-grade aneurysmal SAH. A high-quality randomized clinical trial of intraoperative mild hypothermia to improve postoperative neurological deficits in patients with poor-grade aneurysmal SAH might be feasible (11).
The aim of this pilot randomized controlled trial was to investigate the safety and feasibility of mild TH using endovascular or surface cooling devices in poor-grade SAH patients after successful clipping or coil embolization.
MATERIALS AND METHODS
Patient selection
We performed a single-center randomized controlled study to evaluate the safety and feasibility of mild TH in patients with poor-grade SAH. Patients with poor-grade SAH treated with microsurgical clipping or coil embolization at the Ulsan University Hospital, Ulsan, Korea were enrolled between May 2015 and February 2016. Computed tomography (CT) was performed on all patients and images were interpreted by the attending emergency physician. Patients with a suspected SAH were analyzed by CT angiography or intra-arterial digital subtraction angiography to identify potential intracranial aneurysms. Determination of aneurysm treatment was a multidisciplinary decision based on characteristics of the patient and aneurysm. Emergency microsurgical clipping or endovascular treatment with or without surgical decompression was performed within 24 hours of symptom onset in patients with SAH. We recorded patient characteristics at admission, including demographic data, neurological and neuroradiological data, risk factors for delayed cerebral ischemia (DCI), laboratory findings, in-hospital complications, and mortality (Table 1). We also measured the core body temperature of all patients with esophageal probe.
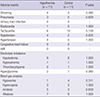
Table 1
Baseline characteristics and demographics in patients with mild hypothermia and controls

The inclusion criteria for this pilot trial were: 1) 18–80 years of age; 2) spontaneous SAH owing to ruptured intracranial saccular aneurysm; 3) complete aneurysm closure by microsurgical clipping or coil embolization within 24 hours of symptom onset; 4) poor-grade SAH defined as Hunt & Hess Scale 4, 5 and modified Fisher Scale 3, 4 at study enrollment; and 5) TH with achievement of target temperature within 1 hour of intervention (12).
The exclusion criteria were as follows: 1) older than 80 years of age; 2) systemic inflammation response syndrome or sepsis at study enrollment; 3) increased bleeding tendency or ongoing life-threatening hemorrhage; 4) multiple or dissecting aneurysms; and 5) disagreement among the patient's family about treatment.
Sample size and randomization
Considering the mortality rate of poor-grade SAH patients of nearly 50%, an alpha error of 0.05 and a 1:1 ratio of TH and control patients, the estimated sample size for a study with 70% power was 22 patients (11 in each group) in “a priori” power analysis with G*power software v.3.1 (13). Twenty-two patients were randomized in a 1:1 ratio based on using sealed and numbered envelopes using computational random-number generator from an independent third party. After informed consent was received, randomization was done by opening sealed allocation envelopes either “TH” or “control” treatment group.
TH protocol
Patients in the TH group were cooled with an endovascular cooling catheter (Zoll Medical, Chelmsford, MA, USA) placed in the inferior vena cava or with a surface cooling pad device (Arctic Sun; Medivance, Inc., Louisville, CO, USA) applied to the patients. The cooling procedure was initiated as soon as the catheter or cooling pad was installed after securing the ruptured aneurysm and continued until the core body temperature reached 34.5°C–35.0°C. The target temperature was 34.5°C, which avoided overcooling or severe complications (514). The core body temperature was recorded every hour using a thermometer at the tip of an esophageal probe. Shivering during mild TH was evaluated using the Bedside Shivering Assessment Scale and patients with a score > 1 was treated with deeper sedation or with a bolus of intravenous meperidine and muscle relaxant in refractory cases (15).
The cooling procedure was maintained for 48 hours then gradual rewarming was initiated. The target rate of active controlled rewarming was 0.5°C of temperature elevation every 12 hours with the reference to the other clinical trial protocol (rewarm target temperature 36.5°C) (4).
Imaging
SAH was initially diagnosed based on CT and aneurysms were identified using CT angiography or intra-arterial digital subtraction angiography. Comprehensive image analysis was performed by a neuroradiologist blinded to the laboratory and clinical data. Follow-up imaging was performed within 24 hours and consecutive scans were carried out at 48- to 72-hour intervals depending on the clinical aspects.
A macrovascular vasospasm was confirmed as an angiographic vasospasm by intra-arterial digital subtraction angiography. Transcranial Doppler blood flow measurements were routinely performed on the day of admission for baseline velocities and on the third and seventh postoperative days for monitoring cerebral vasospasm following SAH by an experienced neurosurgeon who specialized in ultrasound examination. Transcranial Doppler vasospasm was defined as the mean cerebral blood flow velocity in any vessel > 120 cm/s (16). Patients with a mean cerebral blood flow velocity ranging from 120 to 200 cm/s were suspected to have vasospasm, and transcranial Doppler was repeated every 2 days until the velocities normalized. In all cases of Doppler-based vasospasm with any evidence of clinical symptoms, angiographic vasospasm was confirmed by diagnostic subtraction angiography.
DCI was defined as the presence of the focal neurological deterioration or a decrease in the Glasgow Coma Scale of at least 2 points and an infarction on the CT scan that was not visible at admission or immediately following treatment (17).
Adverse events
The rate of adverse events occurring during hypothermia and until 5 days of admission is listed in Table 2. The vital signs of all patients were monitored and daily laboratory follow-up was conducted. Blood pressure and core body temperature were monitored at least every hour on the intensive care unit. Bradycardia was defined as a heart rate of less than 50/min; tachycardia was defined as any heart rate over 100/min; hypotension was defined as a mean arterial pressure < 80 mmHg; and hypertension was defined as a blood pressure of > 185/105 mmHg.
Table 2
Adverse events in hypothermia and control patients within 5 days of admission
Pneumonia was defined as the following 3 criteria: 1) positive chest radiograph; 2) at least of 1 sign of acute infection (documented temperature > 38°C, white blood cell [WBC] count < 4,000 mm3/L or > 12,000 mm3/L; and 3) at least 2 of following: new onset purulent sputum, worsening symptom, rale or bronchial breath sounds, and worsening gas exchange (18). Congestive heart failure was identified by a positive finding on the chest radiograph or echocardiography. Acute myocardial infarction was defined by increased levels of creatinine kinase or troponin-T, and by an ST-T wave change on the electrocardiograph. A parenchymal hemorrhage of the brain was defined as any hemorrhage on the follow-up CT, and brain edema was identified as: 1) localized brain region hypodensities exerting mechanical pressure on the surrounding structures; 2) effacement of the hemispheric sulci and basal cisterns; or 3) bilateral disruption of the hemispheric gray-white matter junction at the level of the centrum semiovale (19). Hypokalemia (< 3.5 mmol/L), hyponatremia (< 135 mEq/L), thrombocytopenia (< 100,000/µL), hyperglycemia (> 200 mg/dL), hypoxemia (PaO2 < 50 mmHg), hypercapnia (PaCO2 > 45 mmHg), acidosis (arterial blood pH < 7.35), and alkalosis (arterial blood pH > 7.45) were also determined.
Outcome assessment
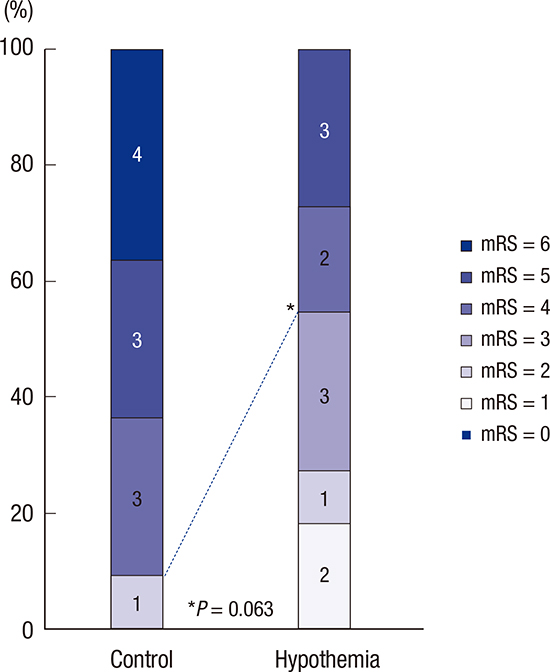
The primary outcome measure for feasibility controlling temperature was the percentage of patients whose core body temperature remained at < 36°C for > 95% of the 48-hour treatment period. The clinical outcome, including modified Rankin Scale (mRS) scores, was also evaluated 3 months after admission. The mRS scores were evaluated by a neurosurgeon or stroke neurologist unrelated to this study. The clinical outcomes were classified as either good (mRS = 0–2) or poor (mRS = 4–6) 3 months after admission. The radiological outcome and mortality were evaluated after 1 month.
General neurocritical care treatment
All eligible patients received standard neurocritical treatment in our stroke center according to the guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage (20). Aneurysms were occluded by microsurgical clipping or endovascular coil embolization within the first 24 hours of admission. All patients receiving TH were sedated using midazolam in combination with remifentanil for analgesia. When the patient's temperature in the control group was exceeded above 37.8°C for > 1 hour, conventional fever management was begun with propacetamol intravenously.
Statistical analysis
All analyses were conducted according to the intention-to-treat principle. A 2-sided P value of < 0.05 was considered statistically significant. Baseline characteristics, demographics, and adverse events were compared between the patient groups by Mann-Whitney U and Fisher's exact tests. Radiological and clinical outcomes were evaluated using χ2 and Fisher's exact tests. Continuous variables without normal distribution were reported as medians and interquartile ranges.
Ethics statement
This study protocol was reviewed and approved by the Institutional Review Board and Ethics Committee of Ulsan University Hospital, Ulsan, Korea (IRB No. 2015-03-025). Informed consent was obtained from patients' relatives or legal representatives to treat patients who met the inclusion criteria.
RESULTS
Seventy-five patients with aneurismal SAH were surgically managed in our institute between May 2015 and February 2016. Twenty-six patients had poor-grade SAH, and 22 of these patients were included in our study after being screened by the inclusion/exclusion criteria.
General demographics
Twenty-two patients (9 males, 13 females; average age 52.82 ± 10.18 years) met the inclusion criteria. Eleven patients were randomly assigned to the TH group and 11 patients to the control group. Baseline characteristics did not differ between the TH and control groups (Table 1). Additionally, there were no differences in the location and treatment of the aneurysm between the 2 groups (P = 1.000).
Feasibility of TH
We accomplished the primary outcome in 10 out of 11 patients receiving TH. The median time from symptom onset to induction of TH was 10 hours (range, 4.5–12.0 hours). Six patients receiving TH reached a core body temperature of < 36°C in a median time of 2 hours (0.5–7.0 hours) and the core temperature was well maintained at 33.4°C–36.0°C (34.6°C ± 0.34°C). Three patients in the TH group (27.2%) were cooled using an intravascular cooling device. After cooling, patients were warmed up for 45 hours (range, 21–57 hours) (Fig. 1). Only one patient was not warmed up actively because the patient regained consciousness and TH was terminated at 48 hours after induction of hypothermia. No technical malfunction of the cooling devices was identified.

Safety of TH
Overall adverse events were more common in the control group (n = 74) compared with the TH group (n = 62). However, the occurrence of each individual adverse event did not differ significantly between the TH and control group (Tables 2 and 3). In particular, pneumonia was reported in 3 patients from the TH group (27.2%) and in 5 patients in the control group (45.5%) (P = 0.659). All pneumonia patients were successfully treated with empirical antibiotics. Hyperglycemia occurred in 2 patients in the TH group (18.1%) and in 7 patients in the control group (63.6%) (P = 0.080), despite the continuous intravenous administration of insulin. No significant differences in other laboratory findings were observed between the TH and control groups (Table 2).
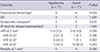
Table 3
Radiological and clinical outcomes in hypothermia and control patients
Radiological outcomes
In the TH group, 10 patients had adverse radiological events: 8 parenchymal hemorrhages, 4 delayed cerebral infarctions, 2 symptomatic vasospasms, and 2 cases of delayed hydrocephalus treated with ventricular-peritoneal (VP) shunting. Patients in the TH group had fewer symptomatic vasospasms (18.1% vs. 36.4%; P = 0.635), and DCI (36.3% vs. 45.6%; P = 1.000) compared with the control group. However, radiological outcomes were not significantly different between the 2 groups (Table 3).
Functional outcome and mortality
There was a higher proportion of good-to-moderate outcomes in the TH group compared with the control group (mRS ≤ 3 at 3 months, 54.5% vs. 9.1%; P = 0.063) (Table 3, Fig. 2). The frequency of poor outcomes (mRS = 4–6) was doubled in the control group (45.5% vs. 90.9%; P = 0.063) (Table 3, Fig. 2). The overall mRS scores were not significantly different at 3 months (P = 0.090). The mortality rate was higher in the control group at 1 month (0.0% vs. 36.4%; P = 0.090).

DISCUSSION
This study is the first randomized controlled trial to investigate the safety and feasibility of mild TH using well-controlled equipment on patients with poor-grade SAH after successful intervention. Mild TH treatment of poor-grade SAH reduced symptomatic vasospasm and DCI, which were associated with better clinical outcomes. Additionally, we identified serious adverse events that were not significantly different between the groups during therapy.
Our TH protocol had 4 important differences from recent studies: 1) a poor-grade group rather than a good-to-moderate grade group was analyzed; 2) the target core body temperature was 34.5°C; 3) hypothermia treatment was performed within 1 hour after (not during) the intervention; and 4) TH was maintained and controlled rewarming was performed for 48 hours to prevent imminent rebound brain edema and pyrexia.
Recent clinical studies of SAH patients have demonstrated that TH is an additional limited treatment for refractory vasospasm and DCI rather than an acute major treatment strategy (212223). However, many aspects of hypothermia as a treatment for SAH remain unknown. Until recently, induced hypothermia during surgical treatment of aneurysm was not routinely recommended. It may represent a reasonable option in selected cases (class III; level of evidence B) (20).
We observed limited effects of TH following SAH, which is in contrast to the findings of ischemic stroke and post cardiac arrest care. We believe that the discrepancy between our findings and previously published findings can be explained by variations in the severity of hemorrhage and different hypothermia protocols described in previous studies. We hope, demonstrating a successful clinical outcome of TH in severe SAH would make this approach more applicable to the general SAH patient population.
When and how TH is administered after hospital admission should also be considered. Treatment of SAH with TH has been mostly reported before and during intervention (561222). However, patient with poor-grade SAH are at higher risk of re-bleeding compared to good-grade SAH (5). Hypothermia can impair blood clotting and induces platelet dysfunction at temperature ≤ 35°C. Bleeding diathesis and ongoing bleeding are contraindications for the use of TH (24). Nevertheless, we assumed applying TH in poor-grade SAH patient before securing the aneurysm might carry a significant re-bleeding risk. Early securing of the aneurysm minimizes its risk of re-bleeding (20). Therefore, we induced TH in selected patients following proper intervention to secure the ruptured aneurysm and reduce the risk of bleeding. Nonetheless, TH was induced earlier (within 24 hours) in our study compared with previous studies (within 48 hours) (14).
The ideal target temperature, initiation, and duration of TH for treating SAH have not been well established. Following cardiac arrest, the current guidelines recommend a target temperature of 32–36°C. TH should be initiated as soon as possible and maintained for at least 24 hours after the return of spontaneous circulation (25). We selected a target temperature of 34.5°C to avoid overcooling and unexpected complications while still maintaining the neuroprotective effect of mild TH in accordance with previous findings (826). Some experts advocate cooling at a slightly higher temperature of 34.5°C–35.0°C in patients with suspected or active bleeding (27). TH was maintained for 48 hours followed by gradual rewarming of 0.5°C every 12 hours to manage clinical deterioration after brain ischemic events (41222).
Fever is very common during neurocritical treatment, affecting 30%–60% of patients with ischemic stroke, traumatic brain injury, intracerebral hemorrhage, and SAH (2829). Many clinical studies have confirmed that fever is an independent predictor of adverse outcomes following stroke and post-anoxic injury after cardiac arrest (729303132). Additionally, the pathophysiological response to SAH is a marked reduction in and increased fluctuation of blood flow to the brain parenchyma, which causes hypoxic damage through changes in the levels of certain intermediate substances (33). Additionally, the brain is vulnerable to oxygen deficiency; thus, deprivation of oxygen will cause neuronal necrosis, apoptosis, and lethal brain edema, resulting in neurological deficits.
We can recommend application of TH for patients with poor-grade SAH because such treatment can control fever and provide neuroprotection. Hypothermia is a highly promising treatment during neurocritical care. TH reduced the risk of cerebral edema and hemorrhagic complications and improved clinical functional outcome after ischemic stroke (42434). Studies on human patients have shown that mild intraoperative hypothermia can reduce the production of reactive oxygen radicals by leukocytes, thereby diminishing cell damage during the process of inflammation (35).
This pilot study evaluated the feasibility and safety of TH in SAH patients. The mean time it took to reach the target temperature was faster in our study (4 hours to 34.5°C) compared with a previous study (48 hours to 35°C) (14). Most patients in the TH group were rewarmed for 45 hours. Only one patient did not remain stable during TH with an automatic temperature control device. This patient regained consciousness and TH was terminated after consultation with the neurosurgeon.
Major adverse events did not differ significantly between groups in our study. TH can induce undesirable physiological changes and adverse effects, such as hypotension, electrolyte imbalance, cardiovascular events, impaired coagulation function, and increased infection risk (36). In our study, the rate of pneumonia was lower in our study compared with previous findings (1437). This might be explained by differences in the duration of TH between the present study and previous studies (5714). All pneumonia patients were successfully treated with empirical antibiotics.
A positive finding from our study is the reduced risk of vasospasm and DCI. Decreased DCI and vasospasm in TH group compared with control group has been described previously (61438). The mortality at 1 month was higher in the control group and good-to-moderate functional outcomes were more frequent in the TH group at 3 months. However, our study sample did not have enough statistical power to demonstrate a significant difference. We hope that future studies will demonstrate that TH can be effective in treating SAH patients.
Our study has several limitations. First, this was a pilot study and should be interpreted with caution. Second, the observed clinical benefits of hypothermia were limited because of the small sample size. A larger sample size may be needed to identify a meaningful difference between TH and control groups. Third, despite well-designed neurocritical care treatment guidelines, a hidden bias may exist between TH and control groups in critical care because the treating physicians were not double blinded. Fourth, the induction time of TH was confined after successful intervention. Fifth, the different use of cooling devices was not reflected in TH group.
In conclusion, in this prospective pilot study, mild TH can be feasible and safely used in patients with poor-grade SAH. The rate of adverse events during TH was similar to standard care of poor grade SAH, therefore TH is an acceptable treatment. We also found that mild TH after successful intervention may reduce the risk of vasospasm and DCI, and lead to improved functional outcomes and reduced mortality in patients with poor-grade SAH. In the future, larger randomized controlled studies should be conducted to determine the safety and clinical impact of TH in poor-grade SAH patients following successful intervention.
 XML Download
XML Download