

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Respiratory distress syndrome (RDS), a clinical condition of pulmonary insufficiency due to lack of surfactant, is the most important factor in mortality and morbidity of preterm infants. Due to the common use of exogenous pulmonary surfactant as the treatment for RDS, there has been a significant reduction in mortality, pneumothorax, pulmonary interstitial emphysema (PIE), and the combined outcome of bronchopulmonary dysplasia (BPD) or death in preterm infants (123). However, there are still controversies on the strategy of surfactant treatment, especially regarding the optimal timing of surfactant administration. The results of a recent meta-analysis showed that early surfactant treatment was more effective compared with delayed selective surfactant treatment with regard to the risk of pneumothorax, PIE, neonatal mortality, and chronic lung disease (4). Furthermore, many studies have shown that prophylactic surfactant administration to infants born at less than 30 weeks gestation could reduce mortality, the frequency and severity of RDS, air leak, and the combined outcome of BPD and death compared with infants who receive placebo or rescue surfactant (5678).
According to these references, prophylactic surfactant replacement therapy was approved by the national health insurance in 2011 in Korea, to the preterm infants born at < 30 weeks of gestation or with birth weight ≤ 1,250 g within 2 hours after birth regardless of respiratory status. From 2011 onward, many neonatal intensive care units (NICUs) in Korea have used prophylactic surfactant for preterm infants born at < 30 weeks of gestation or with birth weight ≤ 1,250 g.
On the contrary, prophylactic surfactant administration has a disadvantage in that it requires intubation and can lead to over-treatment of preterm infants who may not be prone to developing RDS. According to increased utilization of antenatal steroids and early stabilization on continuous positive airway pressure (CPAP) in the delivery room, an updated meta-analysis reported that the benefit of prophylactic surfactant administration is no longer clear (9). Thus, we compared neonatal outcomes of preterm infants in the period of prophylactic surfactant therapy with those of preterm infants in the period of early selective surfactant therapy to evaluate the advantages and disadvantages of prophylactic surfactant therapy.
MATERIALS AND METHODS
Study population and study design
Inclusion criteria were infants born at gestational age of 25–30 weeks or with birth weight ≤ 1,250 g who were born and admitted to the NICU at Samsung Medical Center (SMC) from June 2008 to October 2014. We excluded the infants born in 2011 because, although prophylactic surfactant treatment was performed in Korea from 2011 on, it was applied in practice at SMC from 2012. Patients were divided into 2 groups based on the study period: period 1 (from June 2008 to December 2010) and period 2 (from January 2012 to October 2014). Data collection was conducted retrospectively in period 1, and the Institutional Review Board (IRB) allowed a waiver of informed consent for this retrospective chart review. On the contrary, in period 2, data were prospectively collected, and informed consent was obtained from both parents per the requirement of the IRB.
Exclusion criteria were as follows: 1) infants who expired in the delivery room; 2) infants having potentially life-threatening congenital malformation; and 3) infants whose parents did not provide consent in period 2. Antenatal steroid exposure was defined as maternal receipt of betamethasone at least once during the admission for delivery.
Surfactant policies
In period 1, the surfactant was administered to infants who met all of the following criteria: 1) clinical evidence of respiratory difficulties; 2) radiologic evidence of RDS (diffuse granular opacities or air bronchogram in both lung fields); and 3) need for mechanical ventilation with fraction of inspired oxygen (FiO2) exceeding 40% to sustain optimal blood O2 saturation (50–80 mmHg). Early selective surfactant administration was performed within the first 3 hours of life.
In period 2, prophylactic surfactant was administered to all preterm infants born at < 30 weeks of gestation or with birth weight ≤ 1,250 g in the delivery room immediately after birth regardless of respiratory status. Newborns whose body weight was not clear at birth or who were born in an emergency situation without enough time to prepare the surfactant received prophylactic surfactant as soon as possible after admission to the NICU.
In both groups, Newfactan® (Yuhan Corporation, Seoul, Korea) at a dose of 120 mg/kg was administered after endotracheal intubation. The tube position was confirmed by chest X-ray in period 1 and by auscultation in period 2. The surfactant was administered via a plastic catheter loaded in an endotracheal tube. During surfactant administration, infants were manually ventilated. After administration, patients were supported with mechanical ventilation. Utilization of CPAP in the delivery room was not done in our unit during study period.
Outcomes
The primary outcome was BPD or death. BPD was defined by Jobe and Bancalari criteria (10) as a need for supplemental oxygen or positive pressure ventilator including nasal CPAP at a postmenstrual age of 36 weeks. Secondary outcomes were the number of infants who received surfactant or were intubated, number of surfactant doses, duration of mechanical ventilation including CPAP, duration of endotracheal intubation, duration of oxygen supplement by nasal cannula after extubation or removal of CPAP, the rate of early extubation, the rate of extubation failure, use of postnatal steroids, and pneumothorax.
We defined early extubation as extubation within 2 hours after intubation and extubation failure as reintubation within 48 hours after extubation for any reason. Pneumothorax was diagnosed using chest radiography, and only cases that required chest tube insertion were identified, while those that occurred associated with surgery were excluded.
We also compared the incidence of mortality and common complications of prematurity including BPD, intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), retinopathy of prematurity (ROP), necrotizing enterocolitis (NEC), patent ductus arteriosus (PDA), and sepsis. IVH was defined as a diagnosis of higher than grade III on cranial ultrasonography by classification according to Papile et al. (11), and PVL was defined as cranial ultrasound findings of increased echogenicity and cystic lesions in the periventricular white matter. PDA was evaluated by echocardiography within 10 days of age. ROP was defined as higher than stage III according to international classification (12). NEC was defined as a diagnosis of higher than stage II according to the modified Bell's staging criteria (13). Sepsis was defined by clinical findings and the presence of bacteria or fungus in the blood culture.
Statistical analysis
Comparisons of categorical variables were performed using the χ2 test, and comparisons of continuous variables were evaluated using Student's t-test. Logistic regression analysis was performed to compare risk factors and morbidities of the study groups. Odds ratio (OR) with 95% confidence intervals (95% CIs) for composite morbidity were calculated. SPSS version 19 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses, and P < 0.05 was considered statistically significant.
Ethics statement
The present study protocol was reviewed and approved by the IRB of Samsung Medical Center (IRB No. 2011-10-106). Data collection was conducted retrospectively in period 1, and the IRB allowed a waiver of informed consent for this retrospective chart review. On the contrary, in period 2, data were prospectively collected, and informed consent was obtained from both parents per the requirement of the IRB.
RESULTS
Baseline characteristics
A total of 396 preterm infants at more than 25 weeks and less than 30 weeks of gestation or with birth weight ≤ 1,250 g were born and admitted to the NICU at SMC from June 2008 to October 2014, excluding those in year 2011. In period 1, 193 infants were enrolled; in period 2, 191 infants were enrolled (Fig. 1). During the period from June 2008 to December 2010, despite acceptance of a rescue surfactant treatment protocol, surfactant was administered as prophylaxis in the delivery room in 2 patients who were expected to develop severe RDS after birth. These cases were excluded from this study.

Because there were more small for gestational age (SGA) infants in period 2 (P = 0.031), the mean birth weight of the infants in period 2 (978 ± 260 g) was significantly lower than that of the infants in period 1 (1,042 ± 237 g) (P = 0.011), although the gestational ages of the 2 groups were similar. There were more male infants in period 2 than period 1 (P = 0.014). The rate of premature rupture of membrane (PROM) > 24 hours was higher in period 1 than period 2 (P = 0.049), but the rate of pathologic chorioamnionitis was not different between the 2 groups. Other demographics and population characteristics were similar in the 2 groups (Table 1).
Table 1
Demographic and baseline characteristics of the study population
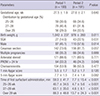
Data are shown as mean ± SD or number (%).
SGA = small for gestational age, PROM = premature rupture of membrane, SD = standard deviation.
![]()
Surfactant administration
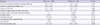
Time from birth to the first surfactant administration was 59.3 ± 41.7 minutes in period 1 and 7.7 ± 15.4 minutes in period 2 (P < 0.001). In period 1, 34 (17.6%) infants managed without intubation, and 51 infants (26.4%) did not receive any surfactant. These numbers are significantly higher compared to those in period 2, when all infants were intubated and administered prophylactic surfactant (P < 0.001). Even though surfactant was used as a prophylaxis in period 2, the use of multiple doses of surfactant in period 2 was significantly higher than in period 1 (28.8% vs. 15.0%, P = 0.001) (Table 2, Fig. 2).
Table 2
Intubation and surfactant use in accordance with gestational age

![]()
 | Fig. 2Distribution of the study population with regard to intubation and surfactant use in accordance with gestational age.
GA = gestational age.
*P < 0.05.
|
In the subgroup analysis of infants in period 1 according to gestational age, in the infants at 25 to 26 weeks gestation, there were no infants who managed without intubation and only 2 infants (3.4%) did not receive any surfactant. The use of multiple doses of surfactant in period 1 was significantly lower than that in period 2 (15.3% vs. 36.4%, P = 0.008). On the other hand, in the infants at 27 to 28 weeks gestation, 13 (16.7%) managed without intubation, and 22 (28.2%) did not receive any surfactant. The use of multiple doses of surfactant in period 1 was significantly lower than that in period 2 (17.9% vs. 34.4%, P = 0.026) (Table 2, Fig. 2). Of infants born at or later than 29 weeks gestation, 21 (37.5%) managed without intubation, and only 29 (51.8%) received surfactant. In the infants born at or later than 27 weeks gestation, the rate of intubation and surfactant use showed a statistically significant difference between the 2 groups (P < 0.001) (Table 2, Fig. 2).
Neonatal outcomes
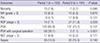
There was no significant difference in duration of mechanical ventilation (including CPAP) between the 2 groups, even though the length of CPAP was significantly shorter in period 2 than period 1 (P = 0.009). Duration of oxygen supply by nasal cannula after extubation or removal of CPAP was shorter in period 2 than period 1 (P = 0.006). There was no infant in period 1 who could be extubated within 2 hours after intubation. On the other hand, significantly more infants (n = 19, 9.9%) in period 2 could be extubated within 2 hours (P < 0.001). However, the rate of reintubation within 48 hours after extubation was also higher in period 2 than period 1 (9.4% vs. 3.1%, P = 0.011). The incidence of pneumothorax was significantly higher in period 2 compared with period 1 (5.2% vs. 0.5%, P < 0.001), but that occurred within 3 days after birth had no statistically difference between the 2 groups (0.5% vs. 2.1%, P = 0.173) (Table 3).
Table 3
Comparison of respiratory outcomes between period 1 and period 2
Data are shown as mean ± SD or number (%).
CPAP = continuous positive airway pressure, SD = standard deviation.
![]()
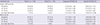
Other outcomes including grade 3 or 4 IVH, cystic PVL, ROP, PDA, NEC, and sepsis were comparable between the groups. Although the rate of PDA with surgical treatment decreased significantly in period 2 compared with period 1 (P < 0.001) (Table 4).
Table 4
Comparison of neonatal morbidity between period 1 and period 2
Values are presented as number (%).
IVH = intraventricular hemorrhage, PVL = periventricular leukomalacia, ROP = retinopathy of prematurity, PDA = patent ductus arteriosus, NEC = necrotizing enterocolitis.
![]()
After adjustment for gender, SGA, Cesarean section, the number of surfactant doses, and PDA with surgical treatment, BPD or death was not significantly different between the 2 groups. After subgroup analysis, according to gestational age, the result did not change. On the other hand, PDA treatment with surgical ligation revealed an increasing factor of BPD or death (OR, 3.90; 95% CI, 1.83–8.33) (Table 5).
Table 5
Death or BPD at 36 weeks
Adjusted OR was adjusted for SGA, gender, Cesarean section, number of surfactant doses, and PDA with surgical treatment.
BPD = bronchopulmonary dysplasia, OR = odds ratio, CI = confidence interval, SGA = small for gestational age, PDA = patent ductus arteriosus.
![]()
DISCUSSION
Several meta-analyses have shown that prophylactic surfactant treatment is preferable to selective surfactant treatment for reducing mortality, pneumothorax, PIE, and the need for mechanical ventilation (56). Contrary to these studies, our study showed that prophylactic surfactant administration to preterm infants born at < 30 weeks of gestation or with birth weight ≤ 1,250 g immediately after birth was not superior to early selective surfactant treatment in reducing BPD or death or in improving other clinical outcomes. As in our study, the efficacy of combining prophylactic Curosurf® (poractant alfa; Chiesi USA, Inc., Cary, NC, USA) with early nasal CPAP in delivery room (CURPAP) trial (14), an international randomized controlled trial to evaluate the efficacy of combining prophylactic surfactant and early nasal CPAP in very preterm infants, concluded that prophylactic surfactant was not superior to nasal CPAP or early selective surfactant in decreasing the incidence of main morbidities of prematurity in spontaneously breathing very preterm infants. The reason for this difference is that previous studies of meta-analyses were performed when prenatal steroid use was very low (–30%) compared with 90% in our study and 96% to 98% in the CURPAP trial. This increased use of prenatal steroids may be one of the reasons why there was no difference between prophylactic surfactant treatment and early selective surfactant treatment.
Other surfactant trials that compared prophylaxis and selective treatment during an era of high antenatal steroid use have shown that 40% to 50% of infants born at 29 to 30 weeks gestation, 20% to 35% of infants born at 27 to 28 weeks gestation, and 8% to 10% of infants born at or earlier than 26 weeks gestation could be managed with no surfactant replacement (115). Our data demonstrating that 48.2% infants born at over 29 weeks gestation and 28.2% of infants born at 27 to 28 weeks gestation managed with no surfactant replacement in period 1 is comparable to those studies. But only 3.4% of infants born at 25 to 26 weeks gestation could be managed with no surfactant replacement. A possible reason why our study showed a higher rate of surfactant replacement in infants born at 25 to 26 weeks gestation than other studies is that utilization of CPAP in the delivery room was not common in our unit in this study period.
Unlike previous studies in which prophylactic surfactants provided a decreased risk of pneumothorax and PIE (6), our study showed that pneumothorax was significantly increased with prophylactic surfactant treatment. It is thought that intubation and positive pressure ventilation through an endotracheal tube in infants with normal compliant lung rather than surfactant administration, contributed pulmonary injury and the development of pneumothorax. And because this study was performed over a long period of time, there may have been unmeasured changes in ventilator management that could have affected the rate of pneumothorax.
In the comparison of neonatal morbidity between the 2 groups, only PDA treatment with surgical ligation was significantly decreased in period 2, while other outcomes revealed no difference between groups. It may be that prophylactic surfactant treatment decreased the development of hemodynamically significant PDA that needed surgical ligation. However, during the long study period, the PDA management protocol of our unit changed to a less aggressive strategy. Therefore, the rate of PDA treatment with surgical ligation was decreased in period 2 not because of prophylactic surfactant treatment, but rather because of changes in protocol to treat PDA with conservative management and medical management. In the multivariable regression analysis to identify predicting factors affecting BPD or death, PDA treatment with surgical ligation was revealed as a risk factor. Recent studies have shown that surgical intervention to close the ductus arteriosus is an independent risk factor for the development of BPD and mortality (161718). The main limitation of this study is that the intention to reduce surgical ligation in period 2 would act as a confounder on the respiratory outcome.
According to the common use of antenatal corticosteroids in women at risk of preterm labor and greater utilization of CPAP in the delivery room to stabilize infants, recent studies have not demonstrated the benefits of prophylactic surfactant and suggest that stabilization using CPAP and surfactant treatment only for preterm infants who develop respiratory problems may be more effective than a more aggressive approach (9). Updated European guidelines suggest that CPAP should be preferentially started from birth in all babies at risk of RDS (babies usually < 30 weeks gestation) until their clinical status can be assessed. In addition, they recommend suspending prophylactic surfactant to babies at earlier gestational ages and administering early surfactant based on gestational age and FiO2 requirement (babies < 26 weeks with > 0.3 FiO2 and > 26 weeks with > 0.4 FiO2) (19).
Kim et al. (20) previously reported a retrospective multi-center study comparing the outcomes of early prophylactic vs. late selective pulmonary surfactant therapy in preterm infants born at < 30 weeks of gestation or with birth weight ≤ 1,250 g in Korea. They reported a significant decrease in overall mortality and the occurrence of morbidities including PIE, PDA, BPD, persistent pulmonary hypertension of newborn (PPHN), pneumonia, and cholestasis with use of early prophylactic surfactant treatment. However, these findings were not observed in our study. The cause for this discrepancy is considered to be the difference between the times when the surfactant was administered. In that study, early prophylactic surfactant was administered at 0.6 ± 0.0 hours after birth, and late selective surfactant was administered at 2.9 ± 0.2 hours after birth. However, in our study, prophylactic surfactant was administered at 7.7 ± 15.4 minutes after birth, and selective surfactant was administered at 59.3 ± 41.7 minutes after birth. As our results show, if selective surfactant is used as soon as possible, there will be no difference in neonatal mortality and morbidities between prophylactic surfactant treatment and early selective rescue treatment.
There are some limitations to our study. The study was conducted over a relatively long period of time, and some other factors in addition to the different management strategies, such as the trend toward less aggressive management of neonatal care during the study period, might have influenced the incidence of mortality and morbidity between the periods.
In conclusion, the benefit of prophylactic surfactant therapy in infants treated under current practices is no longer clear compared to early selective surfactant therapy in preterm infants born at < 30 weeks gestation or with birth weight ≤ 1,250 g. Tailored surfactant strategies are required to achieve the benefit of early treatment and simultaneously avoid the risk of unnecessary intubation and invasive mechanical ventilation.
 XML Download
XML Download