

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Patients with gastric cancer have been reported to be at risk of synchronous second cancers in other organs (12). Colorectal cancer (CRC) is one of the most frequently detected primary cancers in patients with gastric cancer (3456). Previous studies have demonstrated that the prevalence of synchronous or metachronous CRC in patients with gastric cancer is approximately 0.7%–1.5% (3478), and patients with gastric cancer have a substantially increased risk of CRC (910). Accordingly, several researchers recommend that patients with gastric cancer should undergo screening colonoscopy (910). Moreover, recent studies have reported an increased risk of colorectal adenoma as well as CRC in patients with gastric adenoma, as well as those with gastric cancer (111213). A recent meta-analysis also showed that patients with gastric neoplasm were at increased risk of colorectal neoplasia (CRN), and recommended that screening colonoscopy should be considered for patients with gastric adenoma as well as gastric cancer (14). Although the exact biologic mechanisms underlying the development of synchronous gastric neoplasm and CRN have not been fully elucidated, the sharing of common genetic abnormalities and environmental risk factors are thought to be potential mechanisms linking gastric neoplasm and CRN (141516).
However, in the previous studies investigating the relationship between synchronous gastric neoplasm and CRN, the majority of study participants were over 50 years of age, while data concerning the risk of CRN in young patients aged < 50 years with gastric neoplasm are extremely limited. To date, no studies regarding this issue have focused specifically on the young population. Considering that current guidelines recommend that persons at average risk of CRC begin to undergo screening colonoscopies at the age of 50 years, and the risk of CRN increases in patients with gastric neoplasm, it is obvious that patients, aged ≥ 50 years, with gastric neoplasm, should undergo colonoscopy preferentially. However, it remains unclear whether young patients with gastric neoplasm should also undergo colonoscopy to detect CRN. To obtain a more reliable answer to this issue, we compared the risk of CRN risk between patients with gastric neoplasm and those without gastric neoplasm in a very large sample of asymptomatic young subjects aged < 50 years.
MATERIALS AND METHODS
Study population
We retrospectively analyzed data obtained from a prospectively established cohort. The present study population consisted of asymptomatic participants who had undergone both esophagogastroduodenoscopy (EGD) and colonoscopy as part of a comprehensive health screening program at Kangbuk Samsung Hospital, Seoul and Suwon, Korea, from 2010 to 2014 (n = 153,515). The purpose of the screening program was to promote health through a regular health checkup and to enhance early detection of existing diseases. In Korea, the Industrial Safety and Health Law requires employees to participate in annual or biennial health examinations. About 80% of participants were employees of various companies and local governmental organizations and their spouses, with the remaining participants registering individually for the program. Prior to the performance of endoscopy, interviews by general practitioners were conducted to ensure that all participants were asymptomatic (i.e., no abdominal pain, melena, or hematochezia). Individuals with overt intestinal symptoms were urged to seek medical care.
For the present analysis, the exclusion criteria were as follows: a history of CRC or colorectal surgery (n = 528), a history of gastric neoplasm or gastric surgery (n = 511), poor bowel preparation (n = 14,088), failure of an adequate biopsy (polypoid lesions detected during colonoscopy were not biopsied) (n = 229), and age under 30 years (n = 5,803). Ultimately, the total number of eligible study subjects was 131,888 (Fig. 1). Poor bowel preparation was defined as “large amounts of solid fecal matter found, precluding a satisfactory study; unacceptable preparation; < 90% of mucosa seen” (17).

Measurements and definitions
Data on medical history and health-related behaviors were collected through a standardized, self-administered questionnaire, whereas physical measurements such as height and weight were assessed by a trained staff member. Participants' smoking status was categorized as never, formerly, or currently. Family history of CRC or gastric cancer was defined as CRC or gastric cancer in one or more first-degree relatives at any age. Self-reported use of nonsteroidal anti-inflammatory drugs (NSAIDs) (regular use over the previous month) was also assessed.
Hypertension was defined as systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, or current use of antihypertensive medication. Diabetes mellitus was defined as a fasting blood glucose ≥ 126 mg/dL, hemoglobin A1c ≥ 6.5%, or current use of insulin or antidiabetic mediations. Obesity was defined as body mass index (BMI) ≥ 25 kg/m2, which is the proposed cut-off for the diagnosis of obesity in Asians (18). BMI was calculated by dividing the measured weight (kg) by the square of the height (m2).
Endoscopy and histologic examination
All EGDs and colonoscopies were performed by experienced board-certified endoscopists, using a GIF-H260 esophagoduodenoscope (Olympus Medical Systems, Tokyo, Japan) and EVIS Lucera CV-260 colonoscope (Olympus Medical Systems), respectively. All participants ingested 4L of polyethylene glycol solution for bowel preparation. EGD was performed first, immediately followed by colonoscopy in all cases.
All endoscopically abnormal lesions were biopsied or removed. Histopathological findings for all specimens obtained from biopsy or polypectomy were evaluated by experienced gastrointestinal (GI) pathologists.
Advanced adenoma was defined as the presence of one of the following features: ≥ 10 mm diameter, tubulovillous or villous structure, and high-grade dysplasia (HGD) (19). High-risk adenoma was defined as advanced adenoma or 3 or more adenomas (19). CRN was defined as a cancer or any adenoma, and advanced colorectal neoplasia (ACRN) was defined as a cancer or advanced adenoma (20). Intramucosal cancer was included in the definition of CRC. Serrated adenoma was defined as sessile serrated adenoma or traditional serrated adenoma.
For patients with multiple neoplasms, the most advanced lesion was reported (e.g., adenoma with the greatest diameter or the most serious histology). Gastric neoplasm was defined as a gastric cancer or adenoma.
Statistical analysis
Data are expressed as mean ± standard deviation or frequency (%). Baseline characteristics and colorectal lesions were compared between subjects with and without gastric neoplasm using a χ2 analysis or Fisher's exact test for categorical variables and using the Student's t-test for continuous variables.
A multivariate logistic regression analysis was performed to determine whether the presence of gastric neoplasm independently increases the risk for CRN. We estimated the adjusted odds ratio (aOR) with 95% confidence intervals (CIs) for the association of gastric neoplasm with the risks of CRN after adjusting for potential confounding variables including age, sex, smoking status, family history of CRC, history of colon polyps, use of NSAIDs, obesity, hypertension, and diabetes mellitus. All reported P values are 2-tailed, and P values < 0.05 were considered statistically significant. SPSS Version 18 (IBM Corp., Armonk, NY, USA) was used for statistical analyses.
RESULTS
Baseline characteristics of the study population
In total, 131,888 subjects were eligible for analysis (Fig. 1). Among these, 106,981 (81.1%) were under the age of 50 and 24,907 (18.9%) were aged 50 or more. Among subjects aged < 50 years, 70 (0.07%) had gastric neoplasm (45 gastric cancers, 1 gastric adenoma with HGD, and 24 gastric adenoma with low-grade dysplasia [LGD]). Among subjects aged ≥ 50 years, 112 (0.45%) had gastric neoplasm (59 gastric cancers, 5 gastric adenoma with HGD, and 48 gastric adenoma with LGD).
Comparisons of baseline characteristics of the study population according to the presence of gastric neoplasm in subjects aged < 50 years and subjects aged ≥ 50 years, respectively, are summarized in Table 1. Among subjects aged < 50 years, the mean age was higher in subjects with gastric neoplasm than in those without gastric neoplasm (41.3 vs. 38.7 years, P < 0.001). There were no significant differences between the 2 groups in other baseline characteristics including sex, smoking status, family history of CRC, family history of gastric cancer, history of colon polyps, use of NSAIDs, BMI, hypertension, and diabetes mellitus.
Table 1
Baseline characteristics of study population according to presence of gastric neoplasm
Values are presented as mean ± standard deviation or percentage.
CRC = colorectal cancer, NSAIDs = nonsteroidal anti-inflammatory drugs, BMI = body mass index.
![]()
Among subjects aged ≥ 50 years, patients with gastric neoplasm had a higher mean age (60.8 vs. 56.8 years, P < 0.001); and there was a higher proportion of men (80.4% vs. 58.1%, P < 0.001), current or ex-smokers (63.0% vs. 46.9%, P = 0.002), patients with a family history of CRC (9.8% vs. 5.1%, P = 0.026), NSAID use (10.7% vs. 4.7%, P = 0.003), and hypertension (46.4% vs. 32.9%, P = 0.002), compared with subjects without gastric neoplasm. There were no significant differences in other baseline characteristics including family history of gastric cancer, history of colon polyps, BMI, and diabetes mellitus between the 2 groups.
Risk of colorectal neoplasm according to presence of gastric neoplasm
The prevalence of CRN according to the presence of gastric neoplasm in subjects aged < 50 years is presented in Table 2. The prevalence of all colorectal lesions, including any adenoma (8.6% vs. 13.2%, P = 0.254), advanced adenoma (0.0% vs. 1.2%, P = 0.351), high-risk adenoma (1.4% vs. 1.7%, P = 0.864), CRC (0.0% vs. 0.03%, P = 0.878), overall CRN (8.6% vs. 13.2%, P = 0.251), ACRN (0.0% vs. 1.3%, P = 0.345), and non-ACRN (8.6% vs. 12.0%, P = 0.382), did not significantly differ according to the presence of gastric neoplasm among subjects aged < 50 years.
Table 2
Prevalence of colorectal neoplasm according to presence of gastric neoplasm in subjects aged < 50 years
Values are presented as number and percentage.
LGD = low-grade dysplasia, HGD = high-grade dysplasia, TVA = tubulovillous adenoma, VA = villous adenoma, CRN = colorectal neoplasia, ACRN = advanced colorectal neoplasia.
![]()
The prevalence of CRN according to the presence of gastric neoplasm in subjects aged ≥ 50 years is presented in Table 3. Subjects aged ≥ 50 with gastric neoplasm had a significantly higher proportion of any adenoma (47.3% vs. 31.5%, P < 0.001), advanced adenoma (11.6% vs. 4.3%, P < 0.001), high-risk adenoma (17.0% vs. 7.3%, P < 0.001), overall CRN (48.2% vs. 31.7%, P < 0.001), ACRN (12.5% vs. 4.5%, P < 0.001), and non-ACRN (35.7% vs. 27.2%, P = 0.044), compared with those without gastric neoplasm. However, the prevalence of tubulovillous or villous adenoma, serrated adenoma, 3 or more adenomas, and CRC was not significantly different according to the presence of gastric neoplasm.
Table 3
Prevalence of colorectal neoplasm according to presence of gastric neoplasm in subjects aged ≥ 50 years
Values are presented as number and percentage.
LGD = low-grade dysplasia, HGD = high-grade dysplasia, TVA = tubulovillous adenoma, VA = villous adenoma, CRN = colorectal neoplasia, ACRN = advanced colorectal neoplasia.
![]()
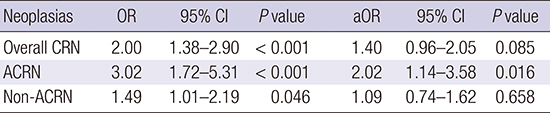
We further performed multivariate logistic regression analysis to identify whether the presence of gastric neoplasm was independently associated with the risk of CRN in subjects aged ≥ 50 years (Table 4). In the multivariate analysis adjusted for confounding factors including age, sex, smoking status, family history of CRC, history of colon polyps, NSAID use, obesity, hypertension, and diabetes mellitus, the presence of gastric neoplasm was identified to be significantly associated with the risk of ACRN (aOR, 2.02; 95% CI, 1.14–3.58). In addition, gastric neoplasm tended to be associated with the risk of overall CRN, although the result was not statistically significant (aOR, 1.40; 95% CI, 0.96–2.05).
Table 4
Risk of CRN in patients with gastric neoplasm (vs. controls) aged ≥ 50 years
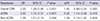
Values were adjusted for age, sex, smoking status, family history of CRC, history of colon polyps, NSAID use, obesity, hypertension, and diabetes mellitus.
OR = odds ratio, aOR = adjusted odds ratio, CI = confidence interval, CRN = colorectal neoplasia, ACRN = advanced colorectal neoplasia, CRC = colorectal cancer, NSAID = nonsteroidal anti-inflammatory drug.
![]()
DISCUSSION
This large-scale study evaluated whether subjects with gastric neoplasm have a higher risk of CRN compared to those without gastric neoplasm in a young population aged < 50 years. To the best of our knowledge, this is the first study to focus on comparison of the risk of CRN between subjects with and without gastric neoplasm in a young population aged < 50 years. We also investigated the risk of CRN according to the presence of gastric neoplasm in subjects aged ≥ 50 years. We found that the prevalence of CRN did not differ according to the presence of gastric neoplasm among subjects aged < 50 years. However, among subjects aged ≥ 50 years, the prevalence of overall CRN, ACRN, and non-ACRN was higher in patients with gastric neoplasm than in those without gastric neoplasm. Moreover, the presence of gastric neoplasm was identified to be independently associated with the risk of ACRN after adjusting for confounding factors among subjects aged ≥ 50 years. Our findings suggest that colonoscopy is necessary for patients with gastric neoplasm if they are over 50 years old, but not if they are under 50 years old.
The exact biologic mechanisms underlying the development of synchronous or metachronous cancers of the stomach and colorectum remain unclear, but several hypothesis have been proposed. First, the presence of common genetic abnormalities may affect the development of both gastric and CRC (15212223242526272829). Gastric cancer and CRC are known to share the same changes in the same genes, such adenomatous polyposis coli (APC), K-ras, deleted in colorectal cancer (DCC), and p53 (15212223242526293031). Genetic mutation of hMSH1 or hMSH2, which is one of the base-pair mismatch repairing proteins, has also been implicated in the pathogenesis of both gastric cancer and CRC (27). Additionally, microsatellite instability resulting from abnormal DNA mismatch repair pathways is thought to play an important role in development of multiple primary GI cancers including gastric cancer and CRC (272829). Second, environmental factors such as smoking, obesity, hyperglycemia, and hyperinsulinemia can act as a common contributor to the development of both gastric cancer and CRC (16323334). Sharing common environmental risk factors, genetic alterations, or both of these factors may contribute to the development of synchronous gastric cancer and CRC.
Several previous studies have shown that patients with gastric cancer have an increased risk of colorectal adenoma as well as CRC (935). Additionally, patients with gastric adenoma have been reported to have a significantly higher risk of colorectal adenoma as well as CRC (11121335). Recently, a meta-analysis of 11 case-control studies also demonstrated that the risk of CRN is significantly increased in patients with gastric neoplasm (odds ratio [OR], 1.72; 95% CI, 1.42–2.09) (14). However, in previous studies, the majority of study participants were over 50 years of age, which is an appropriate study population for CRC screening, while there have been very limited data regarding the risk of synchronous CRN in young patients aged < 50 years with gastric neoplasm.
To date, only 2 studies have examined the prevalence of synchronous CRN in young patients, aged < 50 years, with gastric cancer (3637). One case-control study showed that among subjects, aged < 50 years, the prevalence of synchronous CRN in the gastric cancer group and the control group was 24.0% (6/25) and 16.0% (8/50), respectively, yielding an OR (95% CI) of 1.77 (0.42–7.56), whereas the prevalence among subjects, aged ≥ 50 years, was 38.8% (38/98) and 18.4% (36/196), respectively, yielding an OR (95% CI) of 3.54 (1.80–6.98) (36). Therefore, the study suggested that patients with gastric cancer should be regarded as a high-risk group for CRN, and screening colonoscopy is needed in patients diagnosed with stomach cancer, especially in subjects aged ≥ 50 years (36). Another case-control study reported that a significantly higher risk of CRN was found in the gastric cancer group than in the control group among subjects aged < 50 years (3.4% [4/119] vs. 0% [0/242] for CRC and 26.9% [32/119] vs. 12.0% [19/242] with OR [95% CI], 3.09 [1.1–5.92] for colorectal adenoma) (37). The authors suggested that screening colonoscopy should be recommended for all patients with gastric cancer, including young patients, aged < 50 years (37). However, the aforementioned 2 studies investigated the risk of CRN only in patients with gastric cancer, whereas our study assessed the risk of CRN in patients with gastric adenoma as well as gastric cancer. Our study showed that the presence of gastric neoplasm was associated with an increased risk of CRN in patients aged ≥ 50 years, but not in patients aged < 50 years. Based on our results, young patients aged, < 50 years, with gastric neoplasm, do not appear to require colonoscopy. On the other hand, patients aged, ≥ 50 years, with gastric neoplasm, should be considered a higher priority for colonoscopy.
The present study is the first to evaluate the necessity for colonoscopy in young patients with gastric neoplasm. Nonetheless, there are several limitations in this study. First, this was a retrospective study with a corresponding potential bias in design. However, we think that there was minimal selection bias, because our cohort was established prospectively. Second, our study was hospital-based rather than population-based, and our cohort was recruited at 2 medical centers in Korea. Therefore, there may be some degree of selection bias. Finally, some possible confounding factors, such as Helicobacter pylori infection, which could affect the prevalence of both gastric neoplasm and colorectal adenoma (38), were not investigated.
In conclusion, the presence of gastric neoplasm was associated with an increased risk of CRN in patients aged ≥ 50 years, but not in patients aged < 50 years. Our findings suggest that young patients aged < 50 years with gastric neoplasm do not need to undergo colonoscopy, whereas patients aged ≥ 50 years with gastric neoplasm should be considered a higher priority for colonoscopy.
 XML Download
XML Download