

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The introduction of highly active antiretroviral therapy (HAART) for the treatment of human immunodeficiency virus (HIV) infection changed the characteristics of HIV infection, from a fatal disease to a chronic manageable infectious disease (1). However, as the life expectancy of HIV-infected patients increased, lifestyle-related comorbidities such as cardiovascular disease (CVD), diabetes, and hyperlipidemia began to emerge as a problematic issue and challenge in the treatment of HIV infection. Furthermore, antiretroviral drugs have the potential to induce many adverse drug reactions as well as drug-drug interactions with medications administered for the treatment of other comorbidities (2).
Long-term metabolic complications induced by antiretroviral drugs include osteoporosis, lipodystrophy, dyslipidemia, hyperglycemia, hypertension, and metabolic syndrome, among others. These complications may be risk factors for cerebral vascular disease and coronary artery disease, and may contribute to the morbidity and mortality of these diseases. Recent studies have reported a higher prevalence of these diseases in HIV-infected patients than in the general population (34).
Differences in the prevalence of these long-term metabolic complications have been observed across previous studies, because each of the studies was performed in a different population and used different diagnostic criteria (5). Choe et al. (6) published a study evaluating the incidence of metabolic complications in a Korean population of HIV-infected patients in 2004. The study analyzed 66 HIV-infected patients and found an incidence of metabolic complications of 20.3%. In detail, the incidence of hypertriglyceridemia, hypercholesterolemia, hyperglycemia, and diabetes was 12.3%, 5.8%, 1.4%, and 4.3%, respectively.
To date, several studies have investigated the prevalence of metabolic complications in HIV-infected patients in Korea. However, these studies were limited by small sample sizes, and each study did not analyze metabolic parameters comprehensively (67891011). The purpose of the present study was to identify the prevalence of and evaluate the risk factors for metabolic complications in HIV-infected patients in Korea.
MATERIALS AND METHODS
Study population and design
Participants in this prospective cross-sectional study were HIV-infected subjects who visited 19 hospitals affiliated with the Korean HIV/AIDS Cohort from December 2006 to July 2013. The study protocol was approved by the Institutional Review Board of each of the participating hospitals. All participants were older than 18 years and provided informed consent prior to enrollment. Data at entry to cohort were used for analyses. The prevalence of metabolic abnormalities was calculated, and the rates of metabolic abnormalities were compared with data reported for the general population. The rates of metabolic abnormalities were compared between treatment-naïve and treatment-experienced subjects. In addition, a case-control study was performed to identify risk factors for dyslipidemia.
Data collection
Demographic and clinical characteristics were obtained for all participants. Biologic data such as age, sex, race, body weight, body mass index (BMI), waist circumference (WC), waist/hip ratio, and blood pressure were collected. Regarding comorbidities, history of hypertension, diabetes, dyslipidemia, CVD, smoking history, and family history were collected. In terms of history related to HIV infection, sexual habits, history of exposure route of HIV, time of entry to cohort, time of diagnosis, clinical classification guided by the Centers for Disease Control and Prevention, baseline CD4+ T-cell counts, baseline HIV viral loads, antiviral treatment status, and antiretroviral regimen were collected. Laboratory data related to metabolic complications such as fasting glucose, total cholesterol, high-density lipoprotein (HDL)-cholesterol, low-density lipoprotein (LDL)-cholesterol, and triglycerides were evaluated. To assess cardiovascular risk, the Framingham risk score (FRS) was calculated (12).
Definitions
Hyperglycemia is defined as serum fasting glucose ≥ 126 mg/dL (13). Hypercholesterolemia is defined as serum total cholesterol ≥ 240 mg/dL. Hypoalphalipoproteinemia is defined as serum HDL-cholesterol < 40 mg/dL. Hyper LDL-cholesterolemia is defined as serum LDL-cholesterol ≥ 160 mg/dL. Hypertriglyceridemia is defined as serum triglycerides ≥ 200 mg/dL (14). High and low BMI are defined as BMI > 25 and < 18.5, respectively (15). Dyslipidemia was defined as the presence of one or more of hypercholesterolemia, hyper LDL-cholesterolemia, hypoalphalipoproteinemia, and hypertriglyceridemia (16). Lipodystrophy was defined as the presence of peripheral lipoatrophy or central fat accumulation subjectively measured by standardized physical examination procedure (17). The FRS is the most commonly used tool for prediction of cardiovascular risk, and is calculated using variables including age, sex, total cholesterol, HDL-cholesterol, hypertension, hypertension treatment, diabetes mellitus, and current smoking. Subjects were classified as having a very low, low, moderate, or high 10-year coronary risk in accordance with the Framingham equation (< 10%, 10%–15%, 16%–20%, and > 20%, respectively) (18).
Data analysis
Continuous variables were expressed as mean or median (interquartile range) and compared using Student's t-test if the variables followed a normal distribution. Continuous variables with skewed distribution were compared using the Mann-Whitney U test. Categorical variables were compared using the χ2 test. Variables with a P value less than 0.05 on univariate analysis were included in the logistic regression model for multivariate analysis for predicting risk factors for dyslipidemia. All statistical analyses were performed using SAS 9.2 (SAS Institute Inc., Cary, NC, USA). P values less than 0.05 were considered statistically significant.
RESULTS
A total of 1,096 patients were eligible for inclusion in this study. The median age of participants was 46 years, and the proportion of men was 92.8%. Almost all participants were Korean (99.1%), and the most frequent exposure route of HIV infection was sexual contact (87%). The proportion of intravenous drug use was 0.4%. The median baseline CD4+ T-cell count of participants was 235 cells/μL, and the proportion of treatment-naïve patients was 35.5%. The most commonly used antiretroviral regimen was a protease inhibitor (PI)-based regimen (40.4%) (Table 1).
Table 1
Baseline characteristics of HIV-infected patients in this study

HIV = human immunodeficiency virus, IDU = intravenous drug use, CDC = Centers for Disease Control and Prevention, NRTI = nucleoside analogue reverse transcriptase inhibitor, PI = protease inhibitor, NNRTI = non-nucleoside reverse transcriptase inhibitor, II = integrase inhibitor.
![]()
The prevalence of metabolic complications in all HIV-infected patients in the cohort was as follows. The prevalence of obesity based on BMI, obesity based on waist/hip ratio (waist/hip ratio ≥ 1 in men, ≥ 0.85 in women), hyperglycemia, hypercholesterolemia, hypoalphalipoproteinemia, hyper LDL-cholesterolemia, and hypertriglyceridemia were 16.4%, 19.0%, 10.4%, 6.0%, 44.2%, 5.5%, and 32.1%, respectively (Table 1). Among metabolic parameters, median serum total cholesterol (155 [48–297] vs. 176 [11–364] mg/dL; P < 0.001), HDL-cholesterol (38 [4–137] vs. 45 [10–177] mg/dL; P < 0.001), and triglycerides (155 [14–636] vs. 202 [18–1,040] mg/dL; P < 0.001) were significantly higher in treatment-experienced patients (Table 2). Additionally, the proportion of hypercholesterolemia (2.7% vs. 7.7%; P = 0.008) and hypertriglyceridemia (23.7% vs. 37.2%; P < 0.001) were significantly higher in treatment-experienced patients than in treatment naïve patients. Other metabolic parameters did not show statistically significant differences between the 2 patient groups.
Table 2
Comparisons of metabolic parameters between treatment-naïve patients and treatment-experienced patients

The data were expressed as median (interquartile range) or number (percentage).
BMI = body mass index, WC = waist circumference, HDL = high-density lipoprotein, LDL = low-density lipoprotein, CVD = cardiovascular disease, FRS = Framingham risk score.
*Mann-Whitney U-test, median (interquartile range); †Pearson's χ2-test.
![]()
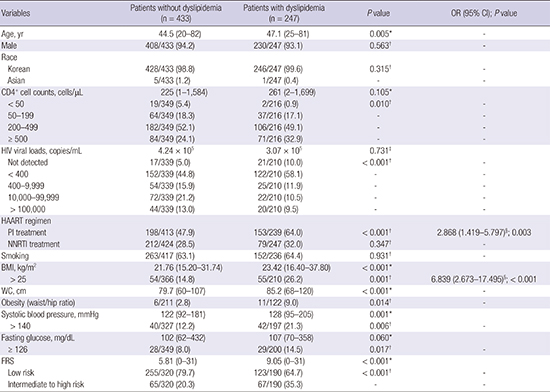
To analyze the risk factors for dyslipidemia in HIV-infected patients, univariate and multivariate analyses were performed. Comparison of the patient group without dyslipidemia and the patient group with dyslipidemia showed that the dyslipidemia group had older age (47.1 vs. 44.5 years; P = 0.005), higher proportion of high CD4+ T-cell counts (P = 0.010) and low HIV viral loads (P < 0.001); higher proportion of PI-based regimen (64.0% vs. 47.9%; P < 0.001); higher BMI (23.42 vs. 21.76 kg/m2; P = 0.001); larger WC (85.2 vs. 79.7 cm; P < 0.001); and higher rate of obesity (9.0% vs. 2.8%; P = 0.014) and high systolic blood pressure (21.3% vs. 12.2%; P = 0.006) than the group without dyslipidemia. However, high BMI (odds ratio [OR], 6.839; 95% confidence interval [CI], 2.673–17.495; P < 0.001) and the use of PI-based regimen (OR, 2.868; 95% CI, 1.419–5.797; P = 0.003) were significant risk factors for dyslipidemia in multivariate analysis (Table 3).
Table 3
Comparison and multivariate analysis of risk factors for dyslipidemia in HIV-infected patients

The data were expressed as median (interquartile range) or number (percentage) or mean.
HIV = human immunodeficiency virus, OR = odds ratio, CI = confidence interval, HAART = highly active antiretroviral therapy, PI = protease inhibitor, NNRTI = non-nucleoside reverse transcriptase inhibitor, BMI = body mass index, WC = waist circumference, FRS = Framingham risk score.
*Mann-Whitney U-test, median (interquartile range); †Pearson's χ2-test; ‡Student's t-test; §Logistic regression analysis.
![]()
DISCUSSION
As the life expectancy of HIV-infected patients is increasing, metabolic complications are emerging as an issue of concern in managing HIV infections. This study evaluated the prevalence and characteristics of metabolic complications in HIV-infected Koreans.
As mentioned above, the prevalence of obesity based on BMI, obesity based on waist/hip ratio, hyperglycemia, hypercholesterolemia, hypoalphalipoproteinemia, hyper LDL-cholesterolemia, and hypertriglyceridemia were 16.4%, 19.0%, 10.4%, 6.0%, 44.2%, 5.5%, and 32.1%, respectively. These results are similar to the findings of a recent study conducted in an Asian population (19), but, compared to a previous Korean study (6), the prevalence of metabolic complications was relatively high. This difference seems to be the result of the difference in the study period between our study and the former study. Over a decade, there have been many changes in treatment trends; therefore, characteristics of HIV-infected patients have changed. When comparing the metabolic parameters between patient groups depending on the presence or absence of antiretroviral treatment, median total cholesterol, HDL-cholesterol, and triglyceride levels were high among patients who received antiretroviral therapy. Furthermore, the prevalence of dyslipidemia and lipodystrophy among comorbidities were also significantly high in the patients receiving antiretroviral treatment. This result is similar to previous study findings. Jantarapakde et al. (19) reported a higher prevalence of lipodystrophy and median total cholesterol, HDL-cholesterol, and triglycerides in patients who had received antiretroviral therapy. Moreover, increases in mean total cholesterol, HDL-cholesterol, and triglyceride levels were observed as the duration of antiretroviral therapy increased in previous studies in Asian patients (2021). Therefore, in consideration of these studies, it can be presumed that antiretroviral therapy influenced the prevalence of metabolic complications.
This is thought to be the result of the combination of the catabolic characteristics of HIV infection, lipodystrophy due to antiretroviral treatment, and the effects on metabolic profiles of antiretroviral therapy. In this cohort, 38.4% of the patients were not undergoing treatment for HIV infection at entry into the cohort, but some antiretroviral regimens such as PIs could cause dyslipidemia.
In comparison of the patient groups depending on the presence or absence of dyslipidemia, high BMI and the use of a PI-based regimen as antiretroviral therapy were significant risk factors for dyslipidemia on multivariate analysis. BMI is associated with the prevalence of dyslipidemia; and a Japanese study conducted by Ishikawa-Takata et al. (22) showed Japanese had a higher prevalence of dyslipidemia than Caucasian, even with low BMI. Since this study was also conducted on Asian, the results can also be referred to the Japanese study. The association between metabolic syndrome and PI exposure was frequently mentioned in previous studies (2324). In addition, dyslipidemia might be associated with lipodystrophy in HIV-infected patients. Fat accumulation, a type of lipodystrophy, can be induced by PI treatment (25). However, the results of a recently reported randomized controlled study indicated that there was no difference in the appearance of fat accumulation between treatment with PIs and other classes of antiretroviral drugs (26). In our cohort, other classes of antiretroviral drug such as non-nucleoside reverse transcriptase inhibitors (NNRTIs) did not show a significant correlation with the appearance of dyslipidemia. However, because about 40% of HIV-infected patients were receiving PI-based regimens, and the percentage of those receiving ritonavir-boosted lopinavir (22.1%), which is well known to induce dyslipidemia, was relatively high, the difference between the previous study and this study can be explained through this factor (data not shown).
CVD is an important predictor of mortality in the general population, and dyslipidemia is an important risk factor for the occurrence of CVD (27). In a previous cohort study of 4,061 patients, dyslipidemia in HIV-infected patients was found to be a major risk factor for CVD (28). Therefore, dyslipidemia caused by HIV infection and antiretroviral agents increases long-term mortality by increasing the risk of CVD. Additionally, HIV infection itself is a risk factor for the development of CVD (3).
This study has some limitations. First, the number of patients was small, and it limits our study results. Second, because of the cross-sectional design of this study, we could not evaluate the incidence of and associated factors for metabolic complications. Third, the distribution of antiretroviral regimens was not even because of the observational study design. Additionally, because we analyzed data from 2006 to 2013, this study could not reflect the current situation of Korea. Especially, single tablet regimens with integrase strand transfer inhibitor are introduced into Korea in 2014, and HAART regimens including integrase strand transfer inhibitor are more commonly used. That might change the prevalence of metabolic complications in Korea since 2014. Finally, there were significant missing values for some important variables such as FRS, smoking history, and so on.
In conclusion, HIV-infected Koreans had higher serum triglyceride levels compared to the general population; however, the prevalence of other metabolic abnormalities was not high. Analysis of patient groups based on the presence or absence of dyslipidemia revealed that antiretroviral therapy contributed to abnormality of lipid profiles; in particular, high BMI and the use of a PI-based regimen were statistically significant risk factor in multivariate analysis. To improve long-term cardiovascular outcomes in HIV-infected Koreans, clinicians should be vigilant regarding the proper management of metabolic abnormalities in these patients.
 XML Download
XML Download