

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Living donor liver transplantation (LDLT) has been used to increase the donor pool and significantly reduce the waiting list mortality of patients in need of liver transplantation (LT) (1). This has been associated with an improved 5-year survival (2). However, the studies about the clinical manifestations, complications, and mortality based on the type of donor reported many different results. Some studies reported similar biliary complications between LDLT and deceased donor liver transplantation (DDLT) (34). Quintini et al. (5) found that LDLT is safe and, in select cases, offers advantages over DDLT. However, other studies have shown a higher risk of biliary complications and higher rates of post-transplant hospitalization in patients who underwent LDLT (678).
In Asian countries, where hepatocellular carcinoma (HCC) is endemic, LDLT is the primary treatment option currently available for HCC and end stage liver disease. Although LDLT accounts for the majority of LT cases in Asia (9), studies about the clinical differences according to the type of donors are mostly investigated in western countries with rare reports from Asian countries.
The main goals of this study are to evaluate the clinical impacts of the type of donor, and the predictors of 1-year mortality in patients who underwent LT, and to recognize the association between type of donor and mortality. Understanding the clinical effects of type of donor on LT and the predictors of mortality may improve the management before and after LT from donor selection to post operation follow up.
MATERIALS AND METHODS
Patients and population
This retrospective study was performed for liver transplant recipients between May 2010 and December 2014 at the Pusan National University Yangsan Hospital, a 1,200-bed teaching hospital. We included all recipients aged 18 years or older, and all patients had been followed from the date of transplantation until either death or up to 1-year post transplant. The demographic data, the baseline characteristics, the outcomes, and the infectious complications were gathered. All the medical records were reviewed for the time the patient underwent LT. The following data was recorded for each patient: age, gender, the cause of liver disease, model for end-stage liver disease (MELD) score, Child-Pugh score, type of donor (living donor or deceased donor), pre-operative laboratory findings (alkaline phosphatase [ALP], C-reactive peptide [CRP], brain natriuretic peptide [BNP], international normalized ratio [INR]), infectious complications, bleeding, rejection, the duration of intensive care unit (ICU) admission, the hospital admission days, needs of extracorporeal membrane oxygenation (ECMO)/mechanical ventilation (vent care), and the 1-year mortality.
Statistical analysis
Statistical analysis was done using SPSS version 20.0 (SPSS Corp., Chicago, IL, USA). The descriptive analysis consisted of the mean, percent and range of the various parameters. The differences between living donor and deceased donor were compared using the χ2 test for the categorical variables, and the t-test or the rank-sum test was used for the numerical variables. Logistic regression analysis was performed to determine the predictors that were independently associated with 1-year mortality. P values < 0.05 were considered to be statistically significant.
RESULTS
Demographic features
A total of 185 recipients who underwent LT were analyzed. The median age was 52.4 years. The ratio was 131 men (70.8%) and 54 women (29.1%).
Of the 185 recipients, 109 (58.9%) belonged to the LDLT group. Compared with DDLT, LDLT recipients had a higher percentage of patients who were diagnosed as HCC (62.4% vs. 21.1%, respectively; P = 0.001) and liver cirrhosis associated hepatitis B virus (71.6% vs. 39.5%, respectively; P = 0.001). They also had a lower level of creatinine, ALP, INR, BNP, CRP, and count of platelet at pre-operative laboratory findings. LDLT recipients had a significantly lower average MELD score (mean ± standard deviation [SD], 12.5 ± 8.3 vs. 24.9 ± 11.7, respectively; P < 0.001) and Child-Pugh score (mean ± SD, 3.6 ± 3.2 vs. 6.1 ± 3.9, respectively; P < 0.001).
There were no significant differences in age and gender between LDLT and DDLT groups. The demographic characteristics of the recipients with LT are shown in Table 1.
Table 1
The demographics of the recipients with LT
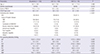
Values are presented as mean ± SD or number (%).
LT = liver transplantation, LDLT = living donor liver transplantation, DDLT = deceased donor liver transplantation, MELD = model for end-stage liver disease, HCC = hepatocellular carcinoma, HBV = hepatitis B, HCV = hepatitis C, ALT = alanine transaminase, Cr = creatinine, ALP = alkaline phosphatase, INR = international normalized ratio, PLT = platelet, CRP = C-reactive peptide, BNP = brain natriuretic peptide, SD = standard deviation.
*Others: 1 sclerosing cholangitis, 1 primary pulmonary hypertension, 1 Klatskin tumor, 2 Wilson's disease.
![]()
Clinical outcome and complications
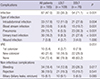
The recipients of DDLT group showed higher 1-year mortality (27.6% vs. 11.0%, respectively; P = 0.004) and post operation 100-days mortality (23.7% vs. 5.5%, respectively; P < 0.001). They also showed longer duration of ICU care (mean ± SD, 23.0 ± 13.8 vs. 10.8 ± 8.8, respectively; P < 0.001), mechanical ventilation care (mean ± SD, 14.1 ± 12.1 vs. 4.3 ± 6.1, respectively; P < 0.001), and hospital admission days (mean ± SD, 52.1 ± 35.4 vs. 32.3 ± 20.7, respectively; P < 0.001).
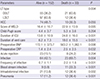
Of the 185 patients enrolled, 87 (47.0%) experienced 173 infectious episodes. Bacterial infections were the most common infectious complications (n = 157, 90.7%), followed by fungal infections (n = 10, 5.7%), viral infections (n = 4, 2.3%), and tuberculosis (n = 1, 0.6%). Enterococcus spp. (31.6%) were the leading pathogens, followed by E. coli (11.1%) and Klebsiella pneumoniae (10.2%).
The most common infections were intraabdominal (17.8%) and urinary tract infection (16.2%), followed by pneumonia (15.7%) and blood stream infections (10.8%). Infectious complications were more frequently observed in DDLT group (71.1% vs 30.3%; P < 0.001). Tables 2 and 3 show the clinical outcome and complications in the patients with LT, according to type of donor.
Table 2
Clinical influence of type of donor in patients with LT

Values are presented as mean ± SD or number (%).
LT = liver transplantation, LDLT = living donor liver transplantation, DDLT = deceased donor liver transplantation, ICU = intensive care unit, ECMO = extracorporeal membrane oxygenation, SD = standard deviation.
![]()
Table 3
Infectious and non-infectious complications according to type of donor in patients with LT
Values are presented as number (%).
LT = liver transplantation, LDLT = living donor liver transplantation, DDLT = deceased donor liver transplantation, VRE = vancomycin resistant enterococcus
![]()
One-year mortality
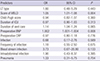
The 1-year mortality rate was 17.8%. Higher mortality rate was seen in recipients with DDLT (P = 0.004), high MELD score (P = 0.005), longer ICU stay (P < 0.001), longer vent care (P < 0.001), higher preoperative BNP (P = 0.008)/CRP (P = 0.032), more frequent infectious complications (P < 0.001) including blood stream infection (P < 0.001), intraabdominal infection (P = 0.002) and pneumonia (P < 0.001). Table 4 shows the differences between the survivors and the non-survivors. According to multi-logistic regression analysis of the predictors of 1-year mortality, MELD score (relative risk [RR], 1.07; 95% confidence interval [CI], 1.04–1.10, P = 0.005), preoperative BNP (RR, 1.02; 95% CI, 1.00–1.19; P = 0.019) were independently associated with 1-year mortality (Table 5).
Table 4
Simple logistic regression analysis of the potential independent risk factors for 1-year mortality
Values are presented as mean ± SD or number (%).
LT = liver transplantation, DDLT = deceased donor liver transplantation, LDLT = living donor liver transplantation, HCC = hepatocellular carcinoma, MELD = end-stage liver disease, ICU = intensive care unit, BNP = brain natriuretic peptide, CRP = C-reactive peptide.
![]()
Table 5
Multiple logistic regression analysis of the potential independent risk factors for 1-year mortality
OR = odds ratio, CI = confidence interval, LT = liver transplantation, MELD = model for end-stage liver disease, ICU = intensive care unit, BNP = brain natriuretic peptide, CRP = C-reactive peptide.
![]()
DISCUSSION
Many patients with end stage liver disease die of disease aggravation while on the waiting list for transplantation. However, the waiting time has been shortened and survival has improved with the advent of LDLT. Living donors provide a large pool of organs, and LDLT seems to be the only immediately available alternative to DDLT (12). In Asian regions such as Japan, Korea, Hong Kong, and Taiwan, where HCC is endemic, LDLT is the main currently available treatment option for HCC and end stage liver disease (101112). Although there have been great advances in LDLT, the studies about the clinical impact of LDLT compared with DDLT is rare in Asian countries.
In this study, we evaluated mortality, days of admission, duration of ICU/ventilator care, infection, and non-infection complications. Compared with DDLT recipients, LDLT recipients had lower MELD score, better liver function and had more advanced HCC. In complication and clinical outcomes, LDLT recipients showed shorter ICU/vent care days, post-operative admission days, and lower mortality. Bleeding and infectious complications were less in LDLT recipients. However, there was no difference in the 2 donor types for biliary complications and rejection (Table 3). Contrary to this study, many other western studies showed higher complication and readmissions in LDLT recipients (6714). Samstein et al. (13) also reported LDLT recipients had a significantly higher probability of technical complications, including bile leaks, biliary strictures and biliary tree infections, but they found a decreasing trend in the probability of biliary stricture in centers performing the highest number of LDLTs per year.
This suggests that greater experience may play a role in considerably lowering the technical complication rates in LDLT recipients (13). Similar biliary complications between LDLT and DDLT recipients in this study seems to be due to the experience gained by performing the LDLT more frequently.
We hypothesized that mortality is affected by type of donors and evaluated the risk factors of 1-year mortality after LT. Recipients with DDLT (P = 0.004) showed higher mortality in univariate analysis. But in the multi-logistic regression analysis, only higher MELD score and higher preoperative BNP were associated with 1-year mortality (Table 5).
Several studies have shown the mortality to be similar in DDLT and LDLT (2101112). Ping et al. (12) did a meta-analysis with 19 published clinical cohort studies, and they reported that perioperative mortality after LT was not significantly different between LDLT and DDLT recipients. We found preoperative BNP was a significant predictor of mortality. Recently, Toussaint et al. (15) reported that recipients with MELD score exceeding 25 and pre-LT serum BNP level less than 155 pg/mL survived, whereas patients combining MELD score exceeding 25 and pre-LT BNP concentration exceeding 155 pg/mL had a 27% ICU mortality rate. Further larger studies about BNP as predictor of mortality are needed.
This study may be affected by all of the limitations of the study's retrospective design. Therefore, further prospective large multi-centered studies are required to provide more accurate results in the Asian region. Cumulative data may help to improve the management before and after LT from donor selection to post operation follow up.
 XML Download
XML Download