

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Upper gastrointestinal (UGI) bleeding is defined as gastrointestinal blood loss proximal to the Treitz ligament (1). The prevalence of acute UGI bleeding is approximately 160 cases per 100,000 people in the United States, which amounts to over 400,000 people per year (1). About 80%–90% of acute UGI bleeding is due to nonvariceal causes, and the most common cause is gastro-duodenal peptic ulcer (20%–50%) (23). Gastroduodenal erosions, Mallory-Weiss tears, and arterio-venous malformation can also cause acute UGI bleeding (3). The mortality rate associated with nonvariceal bleeding is high. In the United Kingdom, the in-hospital mortality rate is reported to be as high as 9.6%, and is especially high in the elderly (24). In Korea, the rate of rebleeding after a successful endoscopic hemostasis for peptic ulcer disease is 17.8%, and the 30-day mortality rate is reported as 2.15%, and it is as high as 7.65% in patients older than 80 years old (567).
In cases of UGI bleeding, early upper endoscopy is recommended within 24 hours of presentation for both diagnostic and treatment purposes, and in most cases the bleeding is managed by endoscopic hemostasis such as sclerotherapy, thermocoagulation, and hemoclipping (8). However, in some cases, rebleeding occurs after endoscopic hemostasis, usually within the first 7 days after the procedure, and the risk varies according to age, size, depth, concurrent comorbidities, and presentation with shock (910). When rebleeding occurs, repeated endoscopic hemostasis, transcatheter arterial embolization (TAE), or surgery can be attempted. However, to our knowledge, research on outcome of TAE in Korea was scanty, and there was a study about factors associated with rebleeding after TAE in nonvariceal UGI bleeding recently, such as coagulopathy and number of embolization territories (11). Here, we report 8 cases of TAE performed for nonvariceal UGI bleeding.
CASE DESCRIPTION
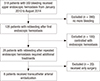
We performed a retrospective analysis on 518 patients who had received upper endoscopic hemostasis procedures from January 2010 to August 2014 in a single tertiary hospital. We reviewed clinical data (age, gender, underlying disease, drug causing bleeding, patient status, and laboratory findings), endoscopic data (bleeding site, Forrest classification), and angiographic data (site of embolization, procedural outcome, material used for embolization). In 128 (24.7%) patients, rebleeding occurred after first endoscopic hemostasis, and in 28 (5.4%) patients, rebleeding occurred after repeated endoscopic hemostasis, which was followed by additional treatments such as surgery or TAE. Among these patients, TAE was performed in 8 (1.5%) patients (Fig. 1).
Of the 8 cases analyzed in this study, 4 represented gastric ulcer bleeding, 3 were duodenal ulcer bleeding, and one was duodenal gastrointestinal stromal tumor (GIST) bleeding identified by surgery. We reviewed one case of gastric ulcer bleeding and GIST bleeding each in detail.
Case 1
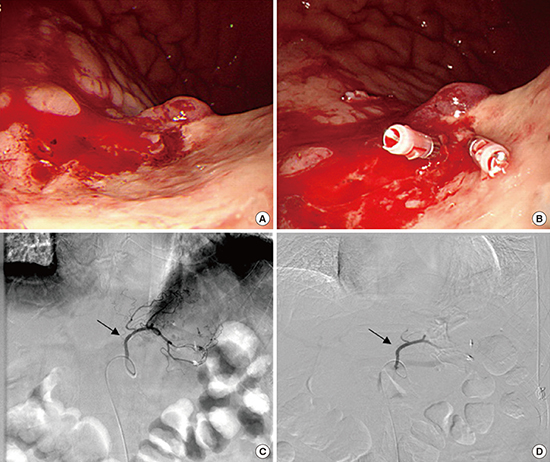
A 75-year-old man visited the emergency room after experiencing syncope and history of melena on August 7, 2014. He had underlying hypertension, a history of single vessel coronary artery occlusion disease, end-stage renal disease managed with hemodialysis, and was taking aspirin regularly. His vital signs were stable and his hemoglobin level was decreased to 3.9 g/dL. Emergency esophagogastroduodenoscopy (EGD) was performed, and a huge ulcer with blood oozing was found at the posterior wall of the midbody. Sclerotherapy was performed but the oozing continued, and hemoclipping also failed (Fig. 2A and B). Therefore, emergency TAE was performed on the same day. Celiac artery angiogram showed no extravasation, and empirical embolization of the left gastric artery (LGA) was performed (Fig. 2C and D). The patient did not experience more bleeding, and was discharged without any complications.
Fig. 2
EGD and angiographic findings of case 1. (A) There is a 2.5-cm sized huge ulcer with blood oozing at the posterior wall of midbody. (B) Blood oozing is still observed after sclerotherapy and hemoclipping. (C) Selective angiogram of LGA (arrow) shows no definite extravasation. (D) After embolization at the LGA using absorbable gelatin sponge particles, LGA angiogram shows near complete obstruction of the distal branches of the LGA.
EGD = esophagogastroduodenoscopy, LGA = left gastric artery.

Case 2
A 74-year-old man visited the emergency room with melena on April 16, 2012. He had underlying hypertension, a history of myocardial infarction and cerebrovascular accident (CVA), and was taking warfarin. He was transferred to our hospital after EGD and hemoclipping for duodenal Dieulafoy's lesion bleeding at another hospital 2 days ago. His initial vital signs were stable, and hemoglobin level was decreased to 8.2 g/dL. Levin tube irrigation was negative, and digital rectal examination suggested melena. The patient was admitted, treated with intravenous proton pump inhibitors. One day later, follow-up EGD was performed and hemoclips were observed near the protruded mass at the second portion of the duodenum without active bleeding. Two days later, he experienced syncope and presented 1,000 mL of melena with a systolic blood pressure (BP) of 50 mmHg and a pulse rate over 120, and was transferred to the intensive care unit. Emergency EGD was performed. A protruded mass with minor blood oozing was observed, and sclerotherapy was performed. However, his hemoglobin level did not recover despite transfusion, and follow-up EGD was performed again the next day. Blood spurting was observed at the center of the mass, and hemoclipping was performed. However, blood oozing continued (Fig. 3). The patient was referred to the radiology department for TAE. Angiographic findings showed focal nodular hypervascular staining in the second portion of the duodenum. Embolization of the superior pancreaticoduodenal artery (SPDA) was performed (Fig. 4). His hemoglobin level was still low with hematochezia, and surgery was performed. Mass excision was performed at the second portion of the duodenum, and the pathologic findings revealed a 2.1 × 1.4 cm sized benign GIST. The patient was discharged without complications.
Fig. 3
EGD findings of case 2. (A) On the next day of admission, about 2 cm sized protruded mass with hemoclipping is observed. (B) On the mass, surface ulceration with minor blood oozing is observed on 3 days after admission. (C) Four days after admission, blood spurting is observed at the center of mass, but (D) blood oozing still remains despite application of hemoclips.
EGD = esophagogastroduodenoscopy.

Fig. 4
Angiographic findings of case 2. (A) Celiac artery angiogram shows no definite extravasation, but a focal nodular hypervascular staining (arrow) in the second portion of the duodenum suggesting hypervascular tumor staining. (B) After superselection of the feeding artery, the SPDA, with microcatheter tip (arrowhead), embolization is performed using absorbable gelatin sponge particles. The arrow indicates the same blood vessel in A. (C) GDA angiogram shows no further focal hypervascular staining (dotted arrow) in the duodenum, and the distal branches of GDA are normal.
SPDA = superior pancreaticoduodenal artery, GDA = gastroduodenal artery.

DISCUSSION
In cases of UGI bleeding, the rate of rebleeding after early endoscopic hemostasis is about 10%–30%, and in 5%–10% of cases, endoscopic procedures fail and require TAE or surgery (1213). In this report, the rate of rebleeding after early endoscopic hemostasis was 24.7% (128/518) and 5.4% (28/518) of the patients underwent TAE or surgery due to rebleeding after repeated endoscopic hemostasis, which is similar to the rates reported by previous studies.
We reviewed 8 rare cases in which TAE was performed for nonvariceal UGI bleeding. Among these cases, there were 4 males, the mean age was 74.00 ± 8.25 years, and most of the patients were taking drugs known to cause bleeding, such as aspirin, or warfarin (Table 1). All patients had at least one underlying disease. The initial hemoglobin levels of all patients were below 9 g/dL, prothrombin time (PT) was prolonged in 4 patients, and initial systolic BP of 3 patients was under 90 mmHg. Initial endoscopic findings revealed gastric origin bleeding in 4 cases and duodenal origin bleeding in the other 4 cases. Forrest classification Ia with spurting hemorrhage and Ib with oozing hemorrhage were also found in 4 cases each. Hemoclipping or sclerotherapy was performed in initial endoscopic hemostasis. In 3 cases, TAE was performed due to rebleeding despite successful primary hemostasis, and in 5 cases, TAE was performed after failure of primary endoscopic hemostasis. Regarding angiographic findings, extravasation was observed in 2 cases out of 8 cases, and embolization was performed at the arterial bleeding site. In the other 6 cases, empirical embolization was performed. The major limitation of TAE is that if it is not performed at the time of bleeding, it is difficult to identify the bleeding vessel because the injected contrast is not extravasated into the bowel lumen, and in this situation, empirical embolization is performed based on the patient's clinical signs, endoscopic findings, and imaging findings (14). Of the 8 cases of embolization observed in this study, 4 were successful, but the other 4 cases showed rebleeding within 48 hours after the procedure. Among the cases with rebleeding, 1 patient was successfully managed with endoscopic hemostasis, and 3 patients eventually received surgery. TAE procedures showed a 50% success rate, but the other 50% of the cases resulted in rebleeding which required additional endoscopic hemostasis or surgery. Several studies have reported that the rebleeding rate of TAE in nonvariceal UGI bleeding ranges from 9%–47%, and this may be due to the varying severity and etiology of the patients' conditions (15). In this study, the patients who received TAE were old aged with medical comorbidities and drug history known to cause bleeding, which may have led to a higher clinical failure rate. In patients who experienced rebleeding after TAE, more patients showed initial coagulopathy (3/4 vs. 1/4), duodenal origin bleeding (3/4 vs. 1/4), and spurting hemorrhage (3/4 vs. 1/4), compared to the patients who had successful TAE.
Table 1
Baseline and clinical characteristics for each case undergoing TAE

TAE = transcatheter arterial embolization, Hb = hemoglobin, PLT = platelets, PT = prothrombin time, BP = blood pressure, F = female, HTN = hypertension, DM = diabetes mellitus, NSAIDs = nonsteroidal antiinflammatory drugs, GDA = gastroduodenal artery, M = male, IHD = ischemic heart disease, CKD = chronic kidney disease, LGA = left gastric artery, CVA = cerebrovascular accident, SPDA = superior pancreaticoduodenal artery, PAOD = peripheral artery occlusive disease, NBCA = N-butyl cyanoacrylate.
TAE is performed in cases of refractory acute UGI bleeding, which is not well controlled by endoscopic procedures, or in cases of massive bleeding or hemodynamic compromise (15). There are no absolute contraindications, but cases with renal insufficiency, contrast allergy or uncorrectable coagulopathy are considered as relatively contraindicated (15). Most of the patients who failed endoscopic hemostasis or had rebleeding after hemostasis were old aged (≥ 70 years old) with comorbidities. These patients were at high risk for complications under general anesthesia, and also were taking antiplatelets or anticoagulants. Therefore, bleeding may have occurred at the incision site after surgery. In some studies, TAE is reported to be associated with fewer complications related to underlying conditions compared to surgery, but the rate of rebleeding is known to be higher (161718). TAE is thought to be relatively safe, but the possibility of complications such as access site hematoma, arterial dissection, contrast nephrotoxicity, and bowel ischemia should also be considered (14). In UK guidelines, it is recommended to repeat endoscopy when rebleeding occurs after endoscopy for initial treatment of UGI bleeding, and to perform TAE or surgery when repeated endoscopy also fails (19). Several studies claimed that success rates and complication rates of TAE and surgery are similar, whereas in some studies TAE is reported to be better than surgery in terms of success and complication rates, therefore, more prospective studies are required in the future (1617181920).
In conclusion, in cases of refractory UGI bleeding after endoscopic hemostasis, treatment plans should be decided based on the patient's condition and the characteristics of the bleeding lesions after discussions between the relevant endoscopists, interventional radiologists, and surgeons. TAE may be attempted prior to surgery when a radiology expert is immediately available, especially in old aged patients with high comorbidity who have high operation risk.
 XML Download
XML Download