

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Overactive bladder (OAB) syndrome is a condition that accompanies urgency, with or without urge incontinence, frequently with increased daytime frequency and nocturia (1). Urgency, the main symptom of OAB, seems to affect nocturia and incontinence (2). The International Continence Society defines nocturia as waking to void one or more times during the night (3). Nocturia is the most common storage symptom in the general population (4). Nocturia is due to nocturnal polyuria, a decreased nocturnal bladder capacity, or a mixture of these 2 terms (5). Various duplicating factors for nocturia have been reported, including pathological conditions such as diabetes, lower urinary tract disorder, cardiovascular disease, primary sleep disorders, and sleep apnea (6). Nocturia can significantly influence quality of life, efficiency, vigor, and awareness of health, primarily due to sleep disruption (78). Thus, the feasibility for the betterment of nocturia may increase sleep quality. Moreover, urgency, which is a key symptom of OAB, is also a significant factor for sleep disruption (9).
Antimuscarinic drugs, the most appropriate treatment for OAB, improve urination urgency and frequency and effectively reduce involuntary contractions and increase bladder capacity in patients with storage symptoms (101112). Solifenacin succinate (Vesicare; Astellas Pharma Co. Ltd., Tokyo, Japan) is a once-daily oral agent that is particularly effective in the bladder (13). In phase 2 and 3 trials, solifenacin has shown significantly decreased frequency and significantly increased voiding volume in symptomatic OAB patients (1415).
Solifenacin is an antimuscarinic drug that is indicated for the treatment of OAB. OAB symptoms respond to extended-release solifenacin. Peak plasma concentrations of solifenacin are reached 3–8 hours after absorption from the gut (13). Thus, nighttime dosing with solifenacin would more effectively improve nighttime symptoms such as nocturia. Moreover, the nighttime dosing of antimuscarinic drugs may improve tolerance compared with daytime dosing (1617). Although several recent studies reported the efficacy of antimuscarinic agents on nocturia and sleep disturbances, these analyzed efficacy regardless of administration time (181920). Therefore, we compared changes in nocturia and sleep-related parameters between daytime and nighttime solifenacin dosing in patents with OAB-associated nocturia.
MATERIALS AND METHODS
Study design and participants
We performed comparative analyses of data from a 12-week prospective, open-label multicenter, randomized study (Ulsan University Hospital, Samsung Changwon Hospital, Kosin University Gospel Hospital, Dong-A University Hospital, and Pusan National University Hospital). All patients were assessed by a disease-specific self-reported questionnaire including the International Prostate Symptom Score (IPSS), Overactive Bladder Symptom Score (OABSS), and Athens Insomnia Scale (AIS). OABSS is obtained as the total of 4 symptom scores that address frequency in daytime, frequency in night time, urgency, and urgency incontinence. The maximum scores for each component were defined as 2, 3, and 5, respectively (21). The AIS is a self-administered questionnaire consisting of 8 items. Each item on the AIS can be rated from 0 (no problem at all) to 3 (very serious problem) (22). The study criteria were follows: nocturia ≥ 2 (times per night), OABSS scale 2 ≥ 2, OABSS scale 3 ≥ 2, and AIS ≥ 6. Patients with urethral stricture, severe bladder outlet obstruction, bladder stones, active urinary tract infection, or chronic bacterial prostatitis were excluded from the study.
All 127 patients who presented to 5 centers in Korea for the treatment of OAB with nocturia between January 2011 and December 2013 were enrolled in this study. All patients took solifenacin 5 mg once per day for > 12 weeks. Participants were then randomly assigned in a 1:1 ratio to group 1, daytime dosing; and group 2, nighttime dosing. Daytime dosing occurred after breakfast, while nighttime dosing occurred after dinner. We evaluated the changes of each parameter before and 12 weeks after daytime or nighttime solifenacin administration. This analysis of nocturia data included patients who completed a bladder diary for 3 consecutive days, whose voiding frequency and voided volume were recorded, and who voided at least once during the night with a mean of 2 nighttime records at baseline. The analysis included patients who continued treatment during the study period and those who completed efficacy and symptom assessments at baseline as well as at 12 weeks.
Adverse events (AEs) were assessed for patients who took at least 1 dose of solifenacin. AEs reported in response to general and non-specific questioning by the researcher or self-reported by the patient were described with severity at each visit. Safety evaluation at weeks 4, 8, and 12 included vital sign, physical examination finding, and AE recordings. The postvoid residual volume was measured by bladder scanning at the start and end of the 12-week treatment period.
Statistical analysis
The 2 groups were compared in terms of clinical characteristics using Pearson's χ2 test for categorical variables and Student's t-test for continuous variables. The quantitative data are expressed as mean and standard deviation. The number of voiding episodes per night, nighttime voided volume, AIS, IPSS, and OABSS were compared between baseline and 12 weeks after administration in each patient group. Efficacy measured between the groups included the mean change from baseline to 12 weeks in the number of voiding episodes per night, nighttime voided volume, AIS, IPSS, and OABSS. Pearson correlation testing was used to examine the correlation among AIS, OABSS, and nocturia. All statistical tests were 2-sided, and values of P < 0.050 were considered significant. The data were analyzed using IBM SPSS Statistics version 21 (IBM, Somers, NY, USA).
RESULTS
The mean age of the entire cohort was 59.2 years; and all patients presented for treatment of OAB with nocturia. Of these patients, 62 (48.8%) with daytime dosing were assigned to group 1 and 65 (51.2%) with nighttime dosing were assigned to group 2. The descriptive characteristics by group are presented in Table 1. Baseline data, which included sex, age, BMI, AIS, total IPSS, and OABSS did not differ between the 2 groups. Mean nocturia before treatment of the whole cohort was 2.4 ± 1.0 episodes per night, but no difference was noted between groups 1 and 2 (2.4 ± 0.8 vs. 2.3 ± 1.1; P = 0.895).
Table 1
Baseline demographic and clinical characteristics
Data are shown as mean ± standard deviation or number (%).
BMI = body mass index, AIS = Athens Insomnia Scale, IPSS = International Prostate Symptom Score, OABSS = Overactive Bladder Symptom Score.
![]()
Table 2 shows changes from baseline after 12 weeks of solifenacin in each group. Total AIS significantly improved from 11.6 at baseline to 7.2 at 12 weeks in group 1 and from 10.4 to 6.4 in group 2 (P < 0.001). The OABSS significantly improved from 8.8 at baseline to 4.6 at 12 weeks in group 1 and from 8.1 to 4.6 in group 2 (P < 0.001). Total IPSS and nocturia also significantly improved after solifenacin administration regardless of administration timing (P < 0.001). Although there were no statistically significant differences, mean nocturia volume also improved from 406 mL at baseline to 213 mL after 12 weeks in group 1 (P = 0.325) and from 442 mL to 268 mL in group 2 (P = 0.204). Postvoid residual urine volume increased from 20.3 mL at baseline to 32.4 mL at 12 weeks in group 1 and from 15.9 mL to 32.3 mL in group 2, but there were no significant differences.
Table 2
Outcome measures among treatment groups

Data are shown as mean ± standard deviation.
AIS = Athens Insomnia Scale, IPSS = International Prostate Symptom Score, OABSS = Overactive Bladder Symptom Score.
![]()
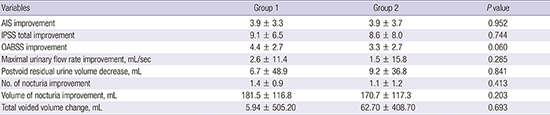
Between groups, there was no statistically significant difference in change of total AIS, IPSS, OABSS, and nocturia before treatment and after 12 weeks of solifenacin (Table 3). Although almost every category except residual urine improved at 12 weeks after solifenacin administration, and there were no significant differences by administration timing. We also assessed the correlation between improved AIS and OABSS and decreased nocturia. We found a correlation between AIS improvement and decreased nocturia from the patient's record (r = 0.303; P = 0.023) and between OABSS improvement and decreased nocturia (r = 0.146; P = 0.383).
Table 3
Comparison of treatment outcomes by medication timing
Data are shown as mean ± standard deviation.
AIS = Athens Insomnia Scale, IPSS = International Prostate Symptom Score, OABSS = Overactive Bladder Symptom Score.
![]()
There were no cases of discontinuation because of AEs. The overall AE incidence was 13.3% (17/127). The percentages of AEs were 14.5% (9/62) and 12.3% (8/67) in groups 1 and 2, respectively (P = 0.797). Among the treatment groups, the incidence of the most common AE, dry mouth was similar for the 2 groups (11.2% in group 1 and 7.7% in group 2, P = 0.458). Constipation, which was mainly mild in all cohorts, occurred in 3.2% of patients in group 1 and 4.6% of patients in group 2. The incidence of constipation was not statistically different between the groups (P = 0.696).
DISCUSSION
This study is the first to evaluate the influence of daytime or nighttime solifenacin dosing in patients with OAB and nocturia. A strict definition of nocturia was used as the inclusion criterion in this study; only patients with ≥ 2 episodes of nocturia were enrolled. Moreover, urgency is the main condition of OAB; therefore, patients who also had urgency (OABSS scale 3 ≥ 2) were enrolled. As a result, our data advocated that solifenacin had the possibility to improve OAB symptoms and sleep quality of patients with sleep disruption and nocturia, which coincides with previous solifenacin clinical studies (1819). Both nocturia and urgency are significant factors for sleep disruption. Thus, using antimuscarinic agents to improve urgency may increase bladder stability and improve sleep quality (9).
The AIS is a self-rating inventory consisting of 8 objectives (2223). The first 5 assess difficulty falling asleep, awakening during the sleep, early morning awakening, total sleep duration, and overall sleep quality, which are representative of nocturnal AIS. The last 3 items are related to the daytime consequences of insomnia. This study also showed that AIS improvement after treatment was related to decreased nocturia. We expect that the decrease in nocturia by solifenacin may improve bladder capacity and reduce contractions. Solifenacin acts as a muscarinic receptor antagonist. Inhibited bladder stimulation may originate a decrease of drive to the brain stem. One paper reported that solifenacin significantly improves nocturnal polyuria and nocturia (24). Although no statistically significant differences were detected, the mean nocturia volume was also reduced in our study. This means that anticholinergic drug use decreases the nocturnal urine volume.
Solifenacin is an excellent drug with few AEs associated with the treatment of OAB with daytime dosing (1819). The results from our study proved that the 24-hour clinical effect of solifenacin persisted with nighttime dosing. A significant reduction in OAB symptoms, nocturia, and sleep disturbances was achieved regardless of administration time. The nighttime dosing of antimuscarinic drugs may improve tolerance compared with daytime dosing (1617). In our study, the overall incidence of AEs was 13.3%, similar between the 2 groups. Although the study populations were different, the lower AE rates in other studies suggest that, in addition to continuing 24-hour efficacy, nighttime dosing may further reduce the AEs related to antimuscarinic therapy (1625). The maximum serum solifenacin concentration is reached 3–8 hours after absorption from the gut (13), and the maximum concentration is likely associated with anticholinergic AEs. Therefore, lower AE rates related with nighttime dosing may be related to the maximum serum concentrations being reached while the patients were sleeping.
Our study has some limitations. First, it was not a placebo-controlled study, so we could not investigate the placebo effect. We also did not conduct urodynamics studies in our patients; rather, we diagnosed OAB using a questionnaire. Furthermore, we could not identify the direct relationship between urgency and sleep quality. Finally, although daytime or nighttime dosing of the anticholinergic drug solifenacin improved OAB symptoms and sleep disturbance, we could not know whether the small reduction in nocturia and the increase in sleep may actually improve patient satisfaction or quality of life. A further study that includes more patients is needed to solve these problems.
In conclusion, our study confirmed that the improved urgency and nocturia by solifenacin administration may also improve sleep quality. However, there were no significant differences by administration timing. Although there are various causes of nocturia, this antimuscarinic drug may not only improve storage symptoms by decreasing urgency and nocturia but also improve sleep disruption for OAB patients with sleep disruptions.
 XML Download
XML Download