

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Stroke is an important health issue in global health care because it is a major cause of morbidity and mortality, and it imposes a significant economic burden on patients (12). The risk of stroke varies with a number of factors. Regarding this issue, aging is the most important risk factor for stroke (3). The elderly's vulnerability to stroke is mainly attributable to the increasing incidences of comorbidities such as hypertension and corresponding vascular damage of other organs (4). Chronic kidney disease is also regarded as vascular damage and serves as a major cause of stroke (5). Specifically, end-stage renal disease (ESRD), the worst stage of kidney function, presents a risk of stroke approximately 5 to 10 times greater than normal kidney function (6). In accordance with the relationship between aging, kidney function, and stroke, elderly patients with ESRD deserve to receive the most attention, as the prevalence of both old age and ESRD has continued to increase (7). However, no active strategy to recover kidney function is circumscribed in elderly patients because they are less well suited to kidney transplantation than their younger counterparts due to their overall poor health status and several comorbidities. In this regard, it is necessary to identify and modify risk factors for stroke in this population before and after the initiation of dialysis, but studies that focus on this important concern are scarce.
Regarding elderly patients with ESRD, our previous work revealed that there was a discrepancy in length of survival between 2 dialysis modalities, hemodialysis (HD) and peritoneal dialysis (PD) (8). Both a meta-analysis and Korean results suggest a higher risk of death in elderly patients receiving PD than in those receiving HD. However, no information on the comparison of cardiovascular morbidities between the 2 modalities was provided. Because the dialysis modality acts as an interaction with the patient outcome, we first compared the risks of cardiovascular diseases, including ischemic heart disease and stroke, between HD and PD in elderly Korean patients. Accordingly, HD was a risk factor of stroke compared with PD. Subsequently, we traced factors predicting stroke occurrence using an independent prospective HD cohort from 31 dialysis centers and found 4 factors related with the stroke risk.
MATERIALS AND METHODS
Data collection from the Korean Health Insurance database
The data on elderly Koreans undergoing dialysis were obtained from the Korean Health Insurance database. The data from all elderly Koreans could be reviewed because Koreans are obliged to register with the national insurance system, which is composed of National Health Insurance and Medical Aid. In total, 35,422 patients with ESRD initiated dialysis between January 2005 and December 2008. From this group, 13,065 elderly patients aged 65 years or older (36.9%) were included in the present analysis.
Baseline parameters, including age, sex, type of insurance, and scale of the hospital (i.e., clinic, hospital or general hospital) were collected after assigning a unique de-identified number to each patient. Comorbidities, such as diabetes mellitus, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, connective tissue disease, peptic ulcer disease, liver disease, hemiplegia, and cancer, were identified by screening the medical history data from the year leading up to the initiation of dialysis therapy based on the International Classification of Diseases 10th revision (ICD-10) (9). Using these covariates, the Charlson comorbidity index (CCI) score for each patient was calculated (10). All patients were divided into 2 groups (HD vs. PD). If patients switched from one modality to the other within 1 month of initiating dialysis, those patients were classified and followed as a changed-modality group as long as no death event occurred within that month. There were no missing data in the variables of the Korean Health Insurance database, but the dataset did not provide detailed information, including biochemical and socioeconomic parameters.
Study patients were followed until kidney transplantation, death, or December 2009. If the dialysis modality changed, the patient was censored. The mortality data were obtained from the Certificate Database (i.e., listing of reasons for changes in eligibility for National Health Insurance or Medical Aid, including death or emigration) as well as through the National Health Insurance Claims Database. The primary outcome was the development of cardiovascular diseases, such as ischemic heart disease and stroke. These conditions were determined using insurance claims recorded in the Korean Health Insurance database.
Data collection from the multicenter cohort of patients with ESRD
To identify the risk factor of stroke in HD, we retrospectively analyzed the Clinical Research Center (CRC) registry for the ESRD cohort, an observational prospective cohort study conducted in Korea. The cohort was established in April 2009 and patients were enrolled from 31 dialysis centers. A total of 2,208 incidents and 2,991 prevalent patients were recruited until March 2015. Among them, 1,082 patients were 65 years old or older with chronic HD (≥ 3 months). We excluded patients for whom selected information, including laboratory and other parameters, were not available (n = 102). Finally, 980 elderly patients receiving chronic HD were analyzed. All of the patients who participated in the study provided informed consent and agreed with examinations in adherence with the study protocol.
Baseline clinical parameters, such as age, sex, dialysis duration, cause of ESRD, body mass index (BMI), systolic blood pressure (SBP) and diastolic blood pressure (DBP) before HD, comorbidities (e.g., diabetes mellitus, cardiovascular disease including ischemic heart disease, chronic heart failure, stroke, peripheral vascular disease, arrhythmia, chronic lung disease, connective tissue disease, peptic ulcer disease, liver disease, and malignancy), the use of anti-hypertensive drugs (e.g., angiotensin converting enzyme inhibitor, angiotensin receptor blocker, diuretics, beta blocker, and calcium channel blocker), anti-coagulant drugs (e.g., aspirin, warfarin, ticlopidine, and clopidogrel), vitamin D, iron supplements, and erythropoietin-stimulating agents, and the type of vascular access. Using the comorbidity parameters, the CCI score and the Davies index were calculated (1011). In accordance with the study questionnaire, patients reported the status of the following factors: smoking, current working, presence of spouse, absolute dependence on family or social support (which included both emotional and economic support), educational level, ambulation, visual acuity, and feeding. Laboratory parameters included whole blood cell counts, hemoglobin, calcium, phosphorus, uric acid, albumin, blood urea nitrogen (BUN), creatinine, sodium, potassium, total cholesterol, triglyceride, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterols, intact parathyroid hormone, ferritin, iron, transferrin saturation, hepatitis B surface antigen, and anti-hepatitis C antibody. The single-pool Kt/V was determined by 2-point urea modeling based on the intradialytic reduction in blood urea and intradialytic weight loss (12).
Elderly patients with HD were followed until dropouts, death, or December 2015. The causes of dropouts included refusal to participate in the study during follow-up, kidney transplantation, and the loss to follow-up. If there were hospitalizations or death, the date and causes were registered at the given institutions. Based on these registrations, we identified the development of stroke-related hospitalizations or deaths as a primary outcome.
Statistical analysis
The data are presented as the means ± standard deviation for continuous variables and as proportions for categorical variables. The χ2 test and Student's t-test were used to compare the categorical variables and continuous variables, respectively. Survival curves were drawn using the Kaplan-Meier method. To compare the survival curves between the groups, the log-rank test was initially applied. To calculate the hazard ratios (HRs) of the outcomes, the Cox proportional hazard model was used, with and without adjustments for the covariates. To identify the risk factors of stroke in the CRC registry, we included age, sex, and parameters with P < 0.1 in the univariate analysis in the multivariate model. To prevent co-linearity among significant risk factors, the backward stepwise selection method was used. A P value of less than 0.05 was considered significant for the estimated HRs. All of the analyses and calculations were performed using SPSS (SPSS version 21.0; IBM, Armonk, NY, USA) and STATA (STATA version 12.0; StataCorp LP, College Station, TX, USA).
Ethics statement
The current study protocol complies with the Declaration of Helsinki and received full approval from the Institutional Review Board at the Seoul National University Hospital (No. 1601-008-729). The CRC registry from a multicenter cohort was approved by the Institutional Review Boards at each center. The Institutional Review Boards are described in the Supplementary 1. All of the patients in the CRC registry provided written informed consent and agreed with the study protocol.
RESULTS
Baseline characteristics of elderly Korean patients receiving dialysis
Table 1 shows the baseline characteristics of elderly Korean patients who began dialysis between January 2005 and December 2008. The mean age was 72.2 years. The number (proportion) of participants in each age category was as follows: 65–69 years, 4,939 (37.8%); 70–79 years, 6,650 (50.9%); 80–89 years, 1,418 (10.9%); and ≥ 90 years, 58 (0.4%). Comorbidities, such as diabetes mellitus, myocardial infarction, and congestive heart failure, were more frequent in PD than in HD; but, other comorbidities, such as cerebrovascular disease, dementia, chronic pulmonary disease, liver disease, hemiplegia, and cancer, were more common in HD than in PD. The patients were followed for a mean duration of 1.8 ± 1.3 years and a maximum of 5 years.
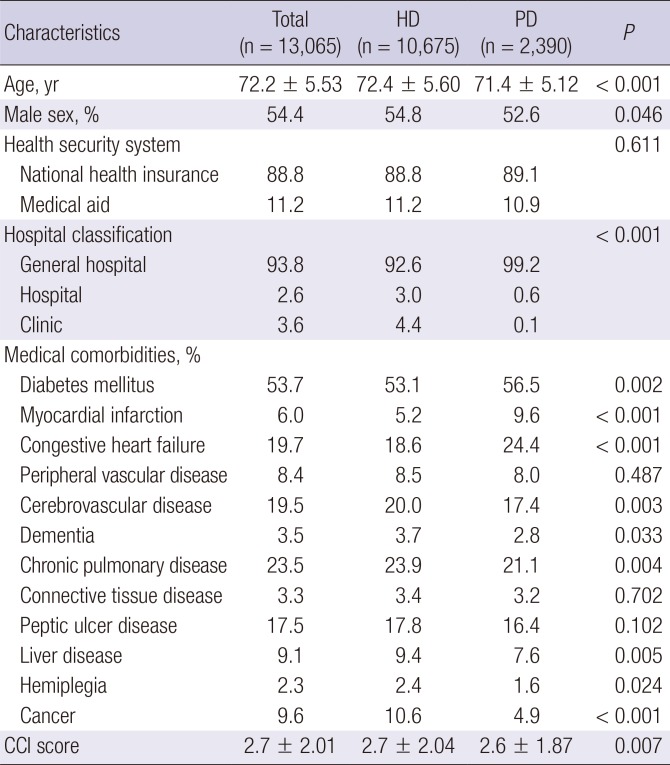
Table 1
Baseline characteristics of elderly Korean patients undergoing dialysis
Statistical differences between dialysis modalities were calculated.
HD = hemodialysis, PD = peritoneal dialysis, CCI = Charlson comorbidity index.
![]()
Cardiovascular disease according to the dialysis modalities
During the follow-up period, cardiovascular disease events occurred in 3,382 patients (25.9%): ischemic heart disease, in 1,307 (10.0%); stroke, in 2,375 (18.2%); and both, in 300 (2.3%). Incidence rates (1,000 patient-year) of cardiovascular disease, ischemic heart disease, and stroke events were 178.7, 60.6, and 117.8, respectively.
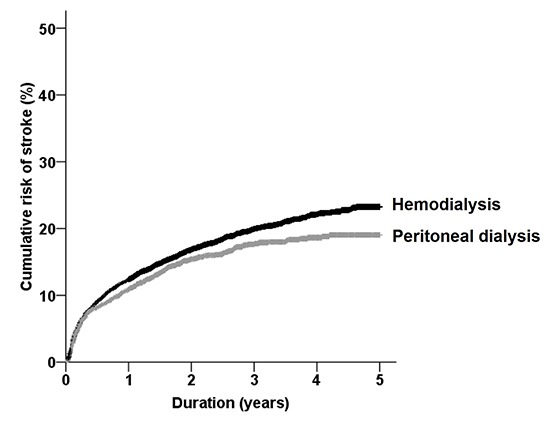
Table 2 shows the cardiovascular event number and rates according to the dialysis modality. Fig. 1 shows the crude cumulative rates of cardiovascular diseases in HD and PD patients. The overall rates of cardiovascular diseases did not differ between 2 modalities (P = 0.090) (Fig. 1A). When the analysis was conducted separately by the subtype of disease, the rates of ischemic heart disease were similar between 2 modalities (P = 0.308) (Fig. 1B), but the rates of stroke differed, as high risk was conferred to HD patients (P = 0.007). Subsequently, we adjusted all the covariates (as shown in Table 1) in the comparison analyses (Table 3), and the difference between the 2 modalities remained also significant in terms of stroke, but not ischemic heart disease.
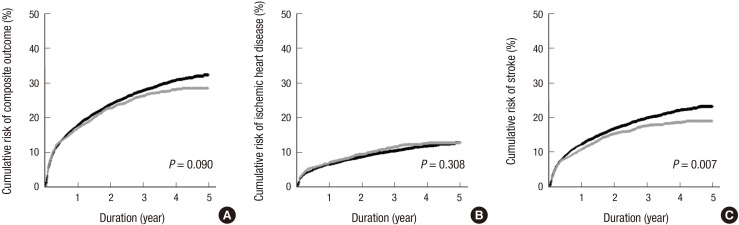
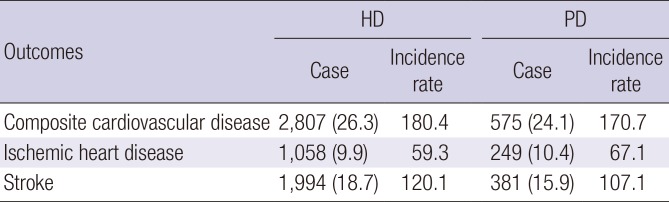

Fig. 1
Cumulative risk of cardiovascular disease according to the dialysis modalities. (A) Composite cardiovascular disease; (B) ischemic heart disease; and (C) stroke. Black and gray lines represent HD and PD, respectively.
HD = hemodialysis, PD = peritoneal dialysis.
![]()
Table 2
Case number and incidence rate (1,000 patient-year) of cardiovascular disease according to the dialysis modality
![]()
Table 3
HRs of cardiovascular outcomes in the HD group compared with the PD group
HD = hemodialysis, PD = peritoneal dialysis, HR = hazard ratio, CI = confidence interval, CCI = Charlson comorbidity index.
*Adjusted for age, sex, health security system, hospital classification, comorbidities including diabetes mellitus, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, connective tissue disease, peptic ulcer disease, liver disease, hemiplegia, cancer, and CCI score.
![]()
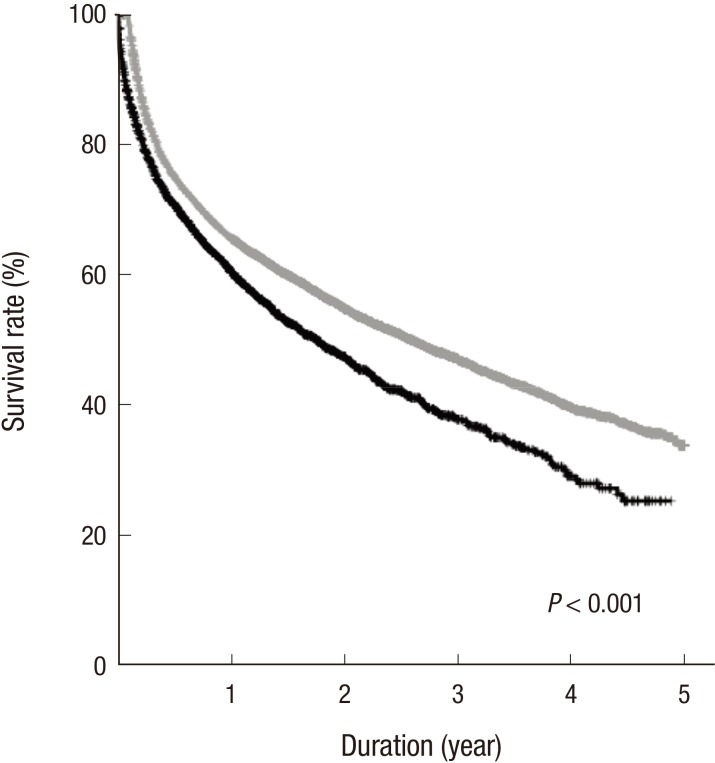
Stroke and subsequent all-cause mortality outcome
Fig. 2 shows the survival curves between the groups with and without stroke. The crude mortality rates of 2 groups were significantly different (P < 0.001). When all the variables were adjusted, the HR in the stroke group was 1.24 (1.165–1.327) compared with the non-stroke group (P < 0.001). When the analyses were separately conducted by dialysis modality, mortality rates (1,000 patient-year) were 288.3 in HD without stroke, 541.6 in HD with stroke, 314.4 in PD without stroke, and 710.3 in PD with stroke. Compared with the groups without stroke, the adjusted HRs of mortality were 1.19 (1.109–1.282) and 1.63 (1.394–1.894) in HD and PD with stroke, respectively (P < 0.001). These data indicated that the subsequent development of stroke was linked to poor survival of elderly dialysis patients.
Risk factor of stroke in HD
Based on the above relationship between HD and stroke risk of elderly patients, we sought to address which factors were responsible for the high risk of stroke in HD. Because the various clinical and laboratory parameters were not available in the Health Insurance database, we reviewed and analyzed 980 elderly patients with HD, all of whom were recruited between April 2009 and March 2015 from 31 dialysis centers. Their baseline characteristics (e.g., socioeconomic parameters, laboratory findings, and the use of medications) are shown in Table 4. The mean age was 72.0 years. The patients were followed for a mean duration of 2.6 ± 2.1 years and a maximum of 7 years. During the following period, 42 patients (4.3%) had stroke events.
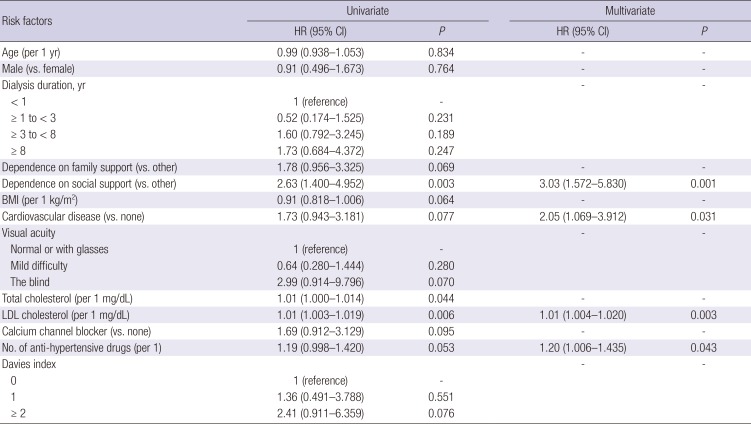
Table 4
Risk factors for the risk of stroke in 980 HD patients from 31 dialysis centers
HD = hemodialysis, HR = hazard ratio, CI = confidence interval, BMI = body mass index, LDL = low-density lipoprotein.
![]()
Supplementary Table 1 shows the baseline difference between the stroke and non-stroke groups irrespective of the timeframe of stroke. Compared with non-stroke patients, the patients with stroke had the following characteristics: longer dialysis duration (P = 0.021); higher absolute dependence on social support (P = 0.001); high LDL cholesterol levels (P = 0.013); and use of high number of anti-hypertensive drugs (P = 0.027). We additionally grouped the continuous variables according to the tertiles or commonly-used criteria, and determined the relationship with stroke (Supplementary Table 2). As a result, the tertiles of LDL cholesterol significantly discriminated the stroke events (P = 0.012), but other continuous variables did not.
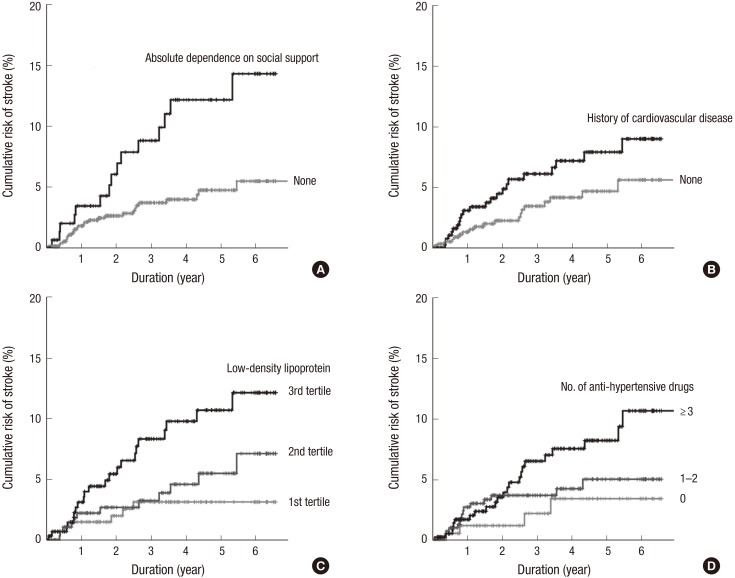
Subsequently, we considered the stroke timeframe by applying Cox proportional hazard models to the parameters with P < 0.100 in the above analyses (Table 4). Univariate analyses were similar to the previous results shown in Supplementary Tables 1 and 2. However, the multivariate analysis finally determined the independent risk factors of stroke as follows: absolute dependence on social support; a previous history of cardiovascular disease; high LDL cholesterol levels; and the use of a high number of anti-hypertensive drugs. Their corresponding risk curves are shown in Fig. 3.
DISCUSSION
The cardiovascular morbidity and mortality of elderly dialysis patients are important issues due to the high incidence of disease with older age, but older patients' choices for active management are limited compared with their younger counterparts. The present study firstly addressed the relationship between modality and cardiovascular risk in a subset of elderly Korean ESRD patients. Accordingly, patients who started with HD had a higher risk of subsequent cardiovascular diseases than those who started with PD. In particular, the risk discrepancy was prominent in stroke events, and these events significantly aggravated all-cause mortality of patients. We additionally addressed the risk factors related to stroke in an HD cohort. The results for certain factors (e.g., history of cardiovascular diseases, hypercholesterolemia, and severe hypertensive state) supported previous findings in the literature, while other results (e.g., absolute dependence on social support) provide new information to the knowledge base in this field.
Regarding which modality may be most suitable for elderly patients, a randomized trial that controls for all possible confounders is not feasible (13). The current knowledge is obtained from several observational studies, and there were controversial results regarding the survival benefits between 2 modalities. One meta-analysis of 8 studies published before the year 2000 reported similar mortality results for both modalities (14). Our recent meta-analysis from 15 cohort studies published after the year 2000 preferred HD to PD, particularly in subgroups that had diabetes mellitus, had long dialysis durations (> 1 year), or contained cohorts that began dialysis in the 1990s (8). Nevertheless, studies that have focused on the risk of cardiovascular disease, not all-cause mortality, in the 2 modalities are scarce (15161718). Some studies definitely preferred PD (1618), but others favored HD (17). Additionally, a study including elderly patients showed that the HD group exhibited worsened cardiovascular parameters (e.g., left ventricular mass index, left ventricular wall thickness, intima media thickness, and intima media area) after 4 years compared with the PD group (16). The present study revealed that the discrepancy of risk was dependent on the type of disease: stroke, not ischemic heart disease, was more common in the HD group than the PD group. Possible mechanisms for the higher presentation of cardiovascular disease in HD include the nature of dialysis regarding rapid loss of residual kidney function and hemodynamic instability compared with PD (1920). We acknowledge that all of these observational results cannot provide clues regarding the preference between HD and PD. However, these studies, including the present results, may be helpful to raise the awareness of modality selection, particularly in terms of the characteristics of each modality.
Several traditional and non-traditional factors are responsible for stroke events in dialysis patients (2122). We identified severe hypertension (i.e., indicated by high number of the anti-hypertensive drugs used) and a previous history of cardiovascular disease as risk factors for stroke in elderly patients receiving HD. In addition to the general mechanism on the relationship between hypertension and stroke (23), HD and hypertension can synergistically increase the stroke risk throughout dialysis-induced ischemia and hemodynamic instability due to ultrafiltration in a short time period (20). Uremic conditions during the non-HD period can further mediate the development of stroke (24). A previous history of cardiovascular disease indicates remnant vascular sequelae and calcification; these vulnerable vessels are also common in the dialysis state or in the elderly population compared with the counterparts (2526). Thus, the cardiovascular history can aggravate the risk of stroke in this subset.
Findings on the relationship between hypercholesterolemia and stroke risk supports the current knowledge (27). However, this positive relationship is applied only to the case of ischemic stroke, not hemorrhagic stroke, wherein high cholesterol levels seem to protect the hemorrhagic stroke (28). The higher incidence of ischemic stroke relative to hemorrhagic stroke might be why hypercholesterolemia was selected as a risk factor (29). Unfortunately, the current CRC-ESRD registry did not provide the subtype of stroke; therefore, this limitation may hamper the conclusions about hypercholesterolemia. Particularly, the great concern about lipid-lowering therapy in dialysis patients has not been fully established (3031).
We found that absolute dependence on social support was strongly associated with stroke risk. This parameter included both emotional and economic supports; thus, the patients who gave a positive answer might have low self-management or low income status. Although subsequent studies will validate our results and their clinical implications, the present results from elderly patients supports the previous concept about the relationship between psychosocial or economic status and the risk of cardiovascular disease (32).
Although the present results are informative, this study has some limitations. The observational study design limits the establishment of any conclusions of causality or underlying mechanisms. Because we primarily considered elderly Korean patients with ESRD, the application of our results to other clinical settings should be performed carefully. Furthermore, other missing or unidentified parameters (e.g., the severity of stroke or the purpose of drug use) could act as confounding factors in the present correlations.
The present study addresses a high risk of stroke in HD and its responsible risk factors in elderly Korean patients with ESRD. Elderly patients with dialysis exhibit a high risk of stroke and subsequent disability or mortality. In this regard, the present study will enrich the present awareness of the elderly patients' vulnerability and form the basis of the future studies to address whether the monitoring and management of factors confirmed here can constitute a strategy to reduce the stroke risk in elderly patients receiving dialysis.
 XML Download
XML Download