

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Since the introduction and establishment of highly active antiretroviral therapy (HAART) as the standard treatment for human immunodeficiency virus (HIV) or AIDS, marked improvement in survival has been seen in people with HIV or AIDS (PWHA) (12345678). Cancer is an important cause of morbidity and mortality in PWHA, but the patterns of cancer after the establishment of HAART is changing (910111213). Three decades ago when HAART was not well established, opportunistic cancers, known as AIDS-defining cancers (ADCs) such as Kaposi's sarcoma, non-Hodgkin's lymphoma, and cervical cancer were the most common types of cancers. However, since the introduction of HAART in 1996, rates of ADCs have decreased dramatically (1415). On the other hand, the burden of non-AIDS-defining cancers (NADCs) is increasing, accompanied by improved survival rates of PWHA (10).
The incidence of NADCs is higher in PWHA than in the general population (101516). In addition to higher incidence, NADCs in PWHA usually progresses more aggressively, is detected at a later stage, and recurs more frequently; PWHA have a worse prognosis than similar staged non-HIV-infected patients with the same cancers (1718). The type of malignancy and incidence of NADCs differs between countries, the difference mainly due to the genetics and socio-economic characteristics of the citizens (91519). It is important to make an appropriate screening plan for the early detection and early treatment of NADCs in PWHA. Therefore, we need to have information about trends of the common types and characteristics of cancers in Korean HIV-infected patients. Cancer epidemiology in Korean PWHA has not been studied since 2007 when 2 studies investigated trends of cancer in Korean PWHA (2021). The objective of this study was to investigate recent trends of cancer in Korean PWHA.
MATERIALS AND METHODS
Study design
A descriptive epidemiology study was conducted to assess the trend of malignancies among PWHA in Korea. All PWHA who visited Pusan National University Hospital from 2000 to 2014 were included in the study. Pusan National University Hospital is a 1,220 bed, university-affiliated teaching hospital and provides HIV care for PWHA in the southeastern area of Korea. Patients below 15 years of age who had no follow-up after their first visit were excluded. Patients who were diagnosed with cancer at least 3 years before diagnosis of HIV were excluded (9). The observation period for individual patients was from the first visit to the date of diagnosis of any cancer; death; transfer to another institute; or December 31, 2014. Demographical, epidemiological, and clinical data were obtained by a retrospective review of medical records. AIDS-defining illness and clinical categories were defined by the 1993 Centers for Disease Control and Prevention (CDC) classification criteria (22). Cancer was defined as such if the diagnosis of cancer was confirmed by histological examinations. Multiple diagnoses of cancers were allowed for a patient if the primary site of cancers were different. Kaposi's sarcoma, non-Hodgkin's lymphoma, and cervical cancer were categorized as ADCs, and all other types of cancers were categorized as NADCs according to the CDC classification criteria. To evaluate the trends in malignancies, we divided the overall observation period into 3 periods (period 1, 2000–2004; period 2, 2005–2009; period 3, 2010–2014) to observe how trends of cancer change every 5 years.
Statistical analysis
IBM SPSS statistics version 22, (IBM, Armonk, NY, USA) was used for all statistical analyses. Categorical variables were compared using Pearson's χ2 test or Fisher's exact test, whereas non-categorical variables were tested using the Mann-Whitney U-test or Kruskal Wallis test. Poisson regression was used to compare incidence rates according to periods. All tests of significance were 2-tailed; P < 0.05 was considered to be significant.
RESULTS
Characteristics of the patients
Nine hundred and fifty PWHA were enrolled into this study. Mean age of the patients was 42.4 ± 11.8 years; 836 (88%) were male and 378 (39.8%) were homosexual. The most common mode of transmission was sexual contact (94.2%), and only 13 patients (1.4%) had an intravenous drug use history. Mean CD4+ T cell count was 250.2 ± 220.9 cells/μL. Four hundred and fifty-nine patients (48.3%) had progressed to AIDS and 432 patients (45.5%) had CD4+ T cell counts of less than 200 when they were diagnosed with HIV infection.
Trends of cancer in PWHA
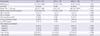
Nine hundred and fifty PWHA were observed for a total of 4,439.71 person-years and 48 episodes (5.05%) of cancer were diagnosed in 47 patients. Cancer incidence among PWHA was 10.8 (95% confidence interval [CI], 8.0–14.3)/1,000 person-years. The incidence of overall cancers and ADCs incidence decreased from 14.5 (95% CI, 0–5.34) and 6.4 (95% CI, 1.7–16.5), respectively in period 1 to 9.80 (95% CI, 6.0–15.2) and 3.0 (95% CI, 1.1–6.4), respectively in period 3, though the differences were not statistically significant. The trend of NADCs incidence remained relatively constant (Table 1). Among the cancers in PWHA, the ratio of NADCs to ADCs increased in the final period (Table 2).
Table 1
Incidence rates of malignancies (cases/1,000 person-years) in HIV-infected patients (95% CI)

Table 2
Trend of NADC vs. total cancer ratio in HIV-infected patients (%)

Characteristics of cancers
Baseline characteristics of PWHA were comparable between with and without cancers, except for age and hepatitis B virus (HBV) co-infection (Table 3). Mean age of patients with cancer was 47.9 ± 9.9 years, and 44 (93.6%) were male. About 20% of patients with cancer were co-infected with HBV.
Table 3
Baseline demographical and clinical characteristics of the enrolled HIV-infected patients

Of 48 episodes of cancer, 20 (42%) episodes were ADCs and 28 (58%) were NADCs. Among the 20 ADCs, non-Hodgkin's lymphoma (5 episodes) and Kaposi's sarcoma were most common malignancies. Among the 28 NADCs, lung cancer (5 episodes) and hepatocellular carcinoma (5 episodes) were most common. However, various types of NADCs such as gastric cancer, colon cancer, and skin cancer were also diagnosed in PWHA (Table 4).
Table 4
Prevalence of malignancies in 950 study patients, 2000 to 2014

HAART = highly active antiretroviral therapy, ADCs = AIDS-defining cancers, CNS = central nervous system, NADCs = non-AIDS-defining cancers.
*Five lung cancers, 5 hepatocellular carcinomas, 4 gastric cancers, 2 colorectal cancers, 2 skin cancers, 2 tonsil cancers, 1 vocal cord cancer, 1 thyroid cancer, 1 bladder cancer, 1 angiosarcoma, and 2 metastases with unknown primary site were included.
Comparison between ADC and NADC
The median age of the patients was 47 (interquartile range [IQR], 40.3–55) years in ADCs and 53 (IQR, 47.3–61.8) in NADCs (P = 0.015). The median CD4+ T cell counts were higher in NADCs group (ADCs 22 [IQR, 9–274] vs. NADCs 389 [IQR, 144–549.3], P < 0.001). Twelve patients (42.9%) among NADCs group and 3 patients (15%) among ADCs group were well adherent to receiving HAART care (P = 0.040). Cancers were detected in 2 of 3 patients with ADCs in the early phase of HAART (1.05 and 1.40 years) in spite of good adherence to care. One-year and 5-year survival rates in PWHA with cancer were 39.5% (ADCs 35.7% vs. NADCs 41.7%, P = 0.717) and 28.1% (ADCs 30.7% vs. NADCs 26.3%, P > 0.999), respectively (Table 5).
Table 5
Characteristics of malignancy patients among HIV infected patients
Values are expressed as number (%) or number (IQR).
HIV = human immunodeficiency virus, ADC = AIDS-defining cancer, NADC = non-AIDS-defining cancer, HBV = hepatitis B virus, HCV = hepatitis C virus, LTF = lost to follow-up, HAART = Highly active antiretroviral therapy, CDC = Centers for Disease Control and Prevention, IQR = interquartile range.
DISCUSSION
Since the introduction of HAART in the mid-1990s, the outcome of PWHA patients who are well adherent to care has improved markedly and the life expectancy has also extended markedly (72324). Before the establishment of HAART, AIDS defining diseases, mainly opportunistic infections, and malignancies were important causes of death. ADCs such as Kaposi's sarcoma and lymphoma were important causes of death among PWHA (37). After the establishment of HAART, AIDS-related deaths gradually decreased and the trends of malignancies in PWHA changed in many countries (91225). The decrease of ADCs and increase of NADCs in PWHA have been described previously in Western countries and in Taiwan (9161925). Along with the accumulation of experience with HAART, non-AIDS-related deaths, i.e., liver disease and cardiovascular disease, are decreasing (26). However, NADCs are increasing and have become a leading non-AIDS-related cause of death among PWHA (26). In Korea, 2 previous studies in 2006 and 2009 that investigated trends of cancer in PWHA showed no increase in NADCs and no decrease in ADCs (2021). Since then, there have been no studies to investigate cancer among PWHA in Korea. Therefore, our findings can provide useful information to improve care among HIV-infected patients.
Firstly, our study showed increasing trends and changing patterns of NADCs among PWHA. In our study, 47 of 950 PWHA patients contracted cancer and the incidence rate of cancer was 10.8/1,000 person-years. There were 8 more cases of NADCs compared to ADCs among the 950 PWHA, and there was a trend of increasing ratio of NADCs development to ADCs development in the last 5 years, though there were no statistically significant differences. The risk of developing NADCs was higher in older patients and on HAART. Lung cancer and hepatocellular carcinoma were followed by gastric cancer, colorectal cancer as the most common NADCs among PWHA in our study. Our data showed a high proportion of hepatocellular carcinoma among PWHA, similar to a previous study, and suggested a high co-infection rate of HIV and HBV in Korean PWHA (27). Interestingly, the proportion of lung cancer among NADCs in our study was markedly increased while the 2 previous studies reported no lung cancer patients among PWHA, and gastric cancer and colorectal cancer were the third and fourth most common cancers (2021). These findings suggested that the pattern of cancer development among Korean PWHA is similar to that of the general population, along with the extension of life expectancy of PWHA due to the advent of HAART (28). However, the 5-year survival rate of PWHA and NADC was less than 30% and it was markedly lower than the 70.3%, 5-year survival rate of the general Korean population (28). The poor prognosis of cancer patients in PWHA suggested that the cancers were detected at advanced stages. Therefore, cancer screening of PWHA on HAART can be improved, even though the patients have good compliance to HAART.
Secondly, our study showed that ADCs still posed a problem in Korea, especially among late presenters or patients with poor adherence to care. In Western countries and Taiwan, incidence rates of ADCs decreased gradually (9151925). In our study, the incidence of ADCs decreased slightly in the last 5 years of the study, although it was not significant, and the proportion of ADCs among cancers of PWHA decreased gradually. However, the incidence rate of ADCs was still higher and around 50% of cancers in PWHA were ADCs when patients initially presented with cancer or revisited after loss to follow-up. Among the patients who retained care and continued HAART for longer than 1 year, 3 patients were diagnosed as ADCs (lymphoma). However, 2 patients were diagnosed immediately after 1 year (1.45 year and 1.05 year after HAART initiation). Therefore, our findings support the need to develop strategies to reduce the number of late presenters and to increase retention to care for improving long-term outcomes of PWHA in Korea (29).
This study has some limitations. First, this study is a hospital-based observational study and we estimated the incidence rates using follow-up periods of our hospital. Furthermore, we defined development of cancer if the cases were histologically confirmed. Therefore, the incidence rate could have been underestimated in this study. Second, our study could not investigate the association between smoking and drinking alcohol, and cancer. Third, our study was conducted at a single center in the southeastern region of Korea although our institute is one of the largest HIV and AIDS care centers in southeastern region of Korea. Therefore, our study should be applied to other regions of the country with caution.
In conclusion, the incidence rate of cancer in Korean PWHA was 10.8/1,000 person-year; 4.5 for ADCs vs. 6.3 for NADCs. The 5-year survival of Korean PWHA with cancer was 28.1%. The ratio of NADCs to ADCs in the patients exhibited increasing trends. The incidence rate of ADCs was still higher, especially among late presenters and patients lost to follow-up. Our findings suggest that effective strategies for detecting HIV infection at an early stage, retaining the patients in care after initiating HAART, and screening NADCs with caution to improve the outcomes of cancer among PWHA in Korea are required.
 XML Download
XML Download