

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Primary immune thrombocytopenia (ITP) is a common acquired bleeding disorder that presents with isolated thrombocytopenia12; and autoantibody-mediated platelet destruction is the mainstay of its pathogenesis.3 The majority of antibodies in ITP are of the immunoglobulin (Ig) G type, and IgG-attached platelets become susceptible to complement opsonization and phagocytosis by the reticuloendothelial system.3 Ig therapy using intravenous immunoglobulin (IVIg) has been used to treat ITP based on the notion that it blocks the phagocytosis of autoantibody-coated platelets by saturating macrophage Fc receptor in spleen. Other immune-modulating activities of IVIg, such as inhibition of antibody production and binding, inflammatory cytokine suppression, and inhibition of complement activation, may also increase platelet counts in patients with ITP.4 In previous studies, IVIg at 1 g/kg/day for two consecutive days resulted in rapid and sufficient increases in platelet counts and thus, this has become one of the preferred schedules of IVIg administration.2567
IVIg preparations are supplied as either lyophilized powder or ready-to-use solutions of varying concentrations, usually 5% or 10%.8 These preparations have somewhat different IgG origins, manufacturing procedures, chemical characteristics, and types and amounts of excipients.8 Furthermore, because IVIg preparations are derived from human plasma, they present risk of blood-borne viral transmission and the transmission of other infectious diseases.9 Therefore, strict precautions are taken during the manufacture of these preparations to inactivate viruses and remove microorganisms. In addition, to address the risk of anaphylactic reaction to IgA, a low IgA content is important for patients with anti-IgA antibodies,10 and because several impurities may have thrombotic effects, impurity removal procedures are required.11
The 10% IVIg formulation has a faster infusion speed than the 5% IVIg formulation, and thus, reduces hospital stays.7 Green Cross (Korea) recently developed a 10% IVIg-SN from human plasma using Cohn fractionation and column chromatography purification procedures. The manufacturing procedure also includes two inactivation processes (solvent/detergent inactivation and nanofiltration) to address the risk of blood-transmitted infections and minimize thrombotic impurities.
This multi-center prospective clinical trial was conducted to investigate the efficacy and safety of IVIg-SN 10% in patients with primary ITP.
METHODS
Patients selection
Patients were eligible if they; 1) were aged 19 years old or more, 2) had been diagnosed with primary ITP, and 3) had a platelet count of < 20 × 109/L by screening complete blood cell count (CBC) performed within 2 weeks of study commencement. Patients receiving corticosteroids were eligible, but only patients on ≤ 20 mg/day of prednisone or other corticosteroids of equivalent dose without any change in dose over the 2 weeks prior to study commencement were enrolled. Patients that had previously received another treatment for ITP were eligible only if > 30 days had passed from last administration of another IVIg formulation or anti-D, > 60 days had elapsed after splenectomy, and > 90 days had passed after the use of immunosuppressants, such as rituximab, vincristine, vinblastine, danazol, or azathioprine, or of thrombopoietin receptor agonists.
The exclusion criteria applied were as follows; a history of hypersensitivity reaction or shock to IVIg, planned splenectomy or another elective surgery, a pregnant or lactating status, or significantly impaired organ function. In addition, patients with secondary ITP, Evans syndrome, or congenital or acquired hemorrhagic diseases other than ITP, were excluded. Patients with abnormal serum Ig (IgG, IgA, or IgM) were not included. Patients who received medications containing aspirin, clopidogrel, none-steroidal anti-inflammatory drugs (NSAIDs), gingko extract, or other substances capable of causing bleeding diathesis were also excluded unless a 2-week washout period had elapsed prior to study commencement.
Study design and endpoints
The study was conducted using a non-randomized, open-label, single-arm, multi-center prospective design (ClinicalTrials.gov identifier: NCT02063789). Response was defined as the achievement of a platelet count of ≥ 50 × 109/L at day 8. The primary endpoint was response after treatment. The null hypothesis was that rate of response to the study drug was inferior to rate of response of historical data determined from previous studies,67 70%. The one-sided 97.5% lower confidence interval (CI) for the gap between rate of response to the study drug and the predefined rate of the response based on the historical data was calculated. If the 97.5% lower CI would be bigger than the predefined non-inferiority margin, −20%, the null hypothesis would be rejected, and non-inferiority of the study drug would be demonstrated. Using a power of 90%, with a one-sided test significance level of P = 0.025, and δ = −0.2, a minimum of 56 patients were needed. Accordingly, assuming a 20% dropout rate, we planned to recruit at least 70 patients.
Secondary endpoints regarding efficacy were to assess time to achievement of platelet count of ≥ 50 × 109/L after treatment, duration of platelet count of ≥ 50 × 109/L, and changes of platelet counts estimated during the first 4 weeks. In addition, response (RIWG) and complete response (CRIWG) according to the International Working Group (IWG) criteria were also investigated.12 According to the criteria, RIWG is defined as platelet count ≥ 30 × 109/L and at least 2-fold increase from the baseline; and CRIWG is defined as platelet count ≥ 100 × 109/L. For the estimation of RIWG and CRIWG, platelet counts should be confirmed on at least 2 separate occasions that are at least 7 days apart and the patients should have no bleeding after treatment. If the increase of platelet count seemed to be a spontaneous regression rather than a response to the study drug, it was not regarded as response to the treatment.
Secondary endpoints regarding safety were to assess adverse events (AEs), viral safety, and frequency and severity of hemorrhagic complications as determined using the ITP Bleeding Scale (IBLS).13
Treatment and evaluation of patients
All patients who satisfied the eligibility requirements were allocated to a single treatment arm and administered IVIg-SN 10% at 1 g/kg/day on two consecutive days. Infusion was started at 0.01 mL/kg/min for 15 minutes, and in the absence of infusion-related reactions, the infusion rate was then doubled every 30 minutes up to 0.08 mL/kg/min. AEs were estimated during every visit of the study; day 0 (baseline), day 1 (the first day of infusion), day 2 (the second day of infusion), day 4, day 6, day 8 (the day of the analysis of the primary endpoint), day 11, day 15, day 22, day 29, and day 85 (the day of the end-of-trial visit).
AEs were recorded and classified as detailed by the Medical Dictionary for Regulatory Activities (MedDRA) version 15.1. AE grades were classified using the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE, v.4.03). Platelet counts and IBLS scores were assessed from day 0 to day 29 and blood chemistry was tested at days 0, 2, 8, and 29. Studies on hepatitis A, hepatitis B, hepatitis C, and human immunodeficiency virus were conducted at days 0, 29, and 85.
Pharmacokinetic (PK) analysis
Blood samples for PK analysis were collected 30 minutes before and after IVIg-SN 10% infusion on days 1 and 2, respectively, followed by once a day at days 4, 8, 15, 29, and 85. Non-compartmental analysis was performed on the plasma concentrations from 25 patients who successfully completed the study without major protocol violation or early termination. The PK data were analyzed using validated software (Phoenix WinNonlin® version 6.4; Pharsight Corporation, Mountain View, CA, USA). Plasma maximum concentration (Cmax) and time to reach Cmax (tmax) were determined directly from the observed values. The individual area under the concentration time curve (AUC) and area under the concentration time versus time curve (AUMC) from time zero to the time of last measurable concentration was estimated by linear trapezoidal summation in the ascending period and by log/linear trapezoidal summation in the descending period. Clearance (CL) was computed as dose/AUC. The rate constant of the terminal phase (λz) was calculated by linear regression of the slope of the terminal portion of the log-transformed serum concentration versus time curve. Volume of distribution based on λz (Vz) was calculated as CL/λz, and steady state volume of distribution (Vss) as dose*(AUMC/AUC2). Mean residence time (MRT) was calculated as AUC/AUMC. Terminal elimination half-life (t1/2β) was calculated as ln(2)/λz, and effective half-life (t1/2, eff) was as ln(2)*MRT.
Data analysis and statistics
To evaluate treatment efficacy, intent-to-treat (ITT) analysis was conducted on patients who were all administered the study drug on at least on occasion (the ITT set). In the ITT set, patient number was calculated with multiple imputations for missing values of platelet counts and written to the first decimal place. The per-protocol (PP) set included patients who successfully completed the study without major protocol violation or early termination. Safety was evaluated in patients who received at least one dose of the study drug (the safety set).
For the primary endpoint, rate of response, the one-sided 97.5% lower CI of the difference between the study drug and historical data was calculated. Time to response was calculated using the Kaplan-Meier method. The χ2 test or Fisher's exact test was used to compare group proportions and the t-test or Mann-Whitney U test was used to compare group means. Except analysis for the primary endpoint, all analyses were two-sided at the level of P < 0.05.
Ethics statement
This study was reviewed and approved by the Institutional Review Board (IRB) of each participating institution (CHA Bundang Medical Center, IRB No. 2004-01-005) and conducted in accordance with the principles expressed in the Declaration of Helsinki. Written informed consent was obtained from all study subjects.
RESULTS
Patients
One hundred and five patients were screened, and 81 patients were enrolled from June 2014 to January 2016 and the follow-up of enrolled patients was completed on April 2016. The final analysis of this study was conducted in August 2016. Those 81 patients satisfied with the definition of the ITT set as well as the safety set. Twenty-one of the study subjects were excluded from the PP analysis because of major protocol violations; these 60 patients constituted the PP set. The reasons of these violations were summarized in Fig. 1. Twenty-five patients in the PP set participated in the PK analysis. Women predominated among the 81 study subjects. Median age of study subjects was 55 years (range 21 to 93). The detailed characteristics of the 81 patients are summarized in Table 1.
 | Fig. 1Diagram of study flow.
ITT = intent-to-treat, PK = pharmacokinetic, PP = per-protocol, Ig = immunoglobulin, ITP = immune thrombocytopenia, AE = adverse event.
|
Table 1
Patient characteristics

![]()
Efficacy
In the ITT set, 61.3 patients (75.7%) responded to IVIg-SN 10%. Because the 97.5% lower CI for the gap between the rate of response of the ITT set and the predefined response rate (70%) was −3.90, non-inferiority of the study drug was demonstrated. The lower 97.5% CI obtained by analysis of the PP set was −4.04, which also showed non-inferiority of efficacy (Table 2).
Table 2
Numbers and percentages of patients who achieved a platelet count of ≥ 50 × 109/L within 7 days after treatment
Data shown are patient number or patient number (%).
ITT = intent-to-treat, CI = confidence interval, PP = per-protocol.
aIn case of the ITT set, patient number was calculated with multiple imputations for missing values and reported the first digit after the decimal point.
![]()
Rate of response was not dependent on the phase of ITP. In the ITT set, 20.5 of 31 patients (66.1%, 95% CI, 48.8%–83.4%) with newly diagnosed ITP (diagnosed within 3 months), 6 of 7 patients (85.7%, 95% CI, 42.1%–99.6%) with persistent ITP (diagnosed within 3 to 12 months), and 34.8 of 43 patients (80.9%, 95% CI, 69.0%–92.8%) with chronic ITP (diagnosed at ≥ 12 months prior to study commencement), achieved response (P = 0.143). Previous splenectomy did not impact response to the study drug. In the ITT set, 5 of 6 splenectomized patients achieved response (83.3%, 95% CI, 35.9%–99.6%) whereas 56.3 of 75 un-splenectomized patients achieved response (75.1%, 95% CI, 65.0%–85.1%; P = 1.000). Response was not dependent on whether patients had previously received steroids and/or immunosuppressant. In the ITT set, 47.8 of 65 patients who had previously received medication achieved response (73.5%, 95% CI, 62.7%–84.3%), whereas 13.5 of 16 patients who had not previously received medication achieved response (84.4%, 95% CI, 64.4%–104.4%; P = 0.505).
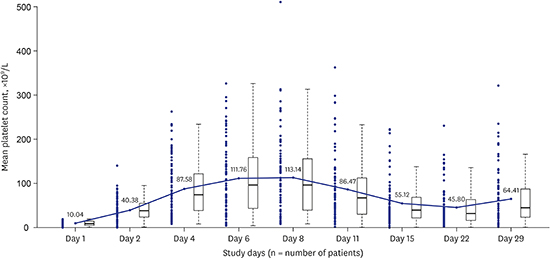
Among responders, most patients exhibited a rapid increase in platelet count after IVIg-SN 10% administration and the median time to a platelet count of ≥ 50 × 109/L post-treatment was 2 days in the ITT (Fig. 2) set and PP set, respectively. Mean duration of a platelet count of ≥ 50 × 109/L was 9.13 ± 8.40 days (95% CI, 7.08–11.19 days) in the ITT set. Among responders estimated platelet counts were highest at days 6 and 8 (Fig. 3).
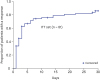 | Fig. 2Kaplan-Meier curves for time to response (platelet count of ≥ 50 × 109/L in 7 days) in the ITT set (n = 81).
ITT = intent-to-treat.
|
 | Fig. 3Changes of platelet counts during the study period in the ITT set (n = 81). Platelet count showed continuous increase from the baseline through day 6, then tend to decrease. Among responders, estimated platelet counts were highest at days 6 and 8.
ITT = intent-to-treat.
|
In the ITT set, rate of RIWG was 46.5% (37.7/81; 95% CI, 35.6%–57.5%) and rate of CRIWG was 17.2% (13.9/81; 95% CI, 8.8%–25.5%). Mean duration of RIWG and CRIWG were 17.2 ± 7.5 days (95% CI, 14.7–19.8 days) and 12.1 ± 5.3 days (95% CI, 9.0–15.2 days), respectively.
Safety and hemorrhagic severity rating scale
In the safety set, 283 AEs were reported in 73 patients, irrespective of casualty. Of these, 113 AEs in 46 patients were thought (either definitely or suspected) to be drug-related. Frequently reported drug-related AEs are summarized in Table 3. Most drug-related AEs were manageable and resolved without sequelae. Severe AEs (SAEs) occurred in 5 patients. Of drug-related AEs, 94 AEs in 33 patients occurred within 72 hours of infusion and were regarded as infusion-related. All infusion-related AEs were well controlled by reducing infusion rate or by temporary cessation but one patient with SAEs of G3 dizziness, G3 headache, and G2 vomiting during infusion. Other SAEs form 4 of the 5 patients were G4 vomiting, G4 gingival bleeding, G4 cerebral hemorrhage, and G4 thrombocytopenia. All 5 patients that experienced SAEs recovered without sequelae. Viral serology studies showed no significant change suggestive of a new episode of viral transmission during the study period. The frequency of mucocutaneous bleeding decreased during the study period, as determined using the IBLS (Supplementary Fig. 1). No newly detected viral infection or thromboembolic event was reported in the study population.
Table 3
Frequently reported drug-related AEs

![]()
PK outcomes
PK data from the 25 patients (10 males and 15 females) were analyzed. Mean baseline concentration of endogenous IgG before administration of the study drug was 11.9 g/L (range, 7.6–15.3 g/L) and PK analysis was conducted for the baseline corrected IgG concentrations. Mean AUC from zero time to day 29 (AUCD0–29) and Cmax were 377.5 g∙day/L (148.4–517.5 g∙day/L) and 34.6 g/L (23.3–46.2 g/L), respectively. Mean terminal elimination half-life was 28.9 days (range, 3.03–193.85 days). The PK results are summarized in Table 4.
Table 4
Results of non-compartmental PK analysis of IV-globulin 10%, 2 mg/kg in 25 patients
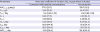
PK = pharmacokinetic, IV = intravenous, AUCD0–29 = area under the plasma concentration-time curve from zero time to day 29, Cmax = maximal concentration, Tmax = time to reach Cmax, Vz = volume of distribution during the terminal phase, Vss = volume of distribution at steady state, CL = clearance, t1/2β = terminal elimination half-life, t1/2β, eff = effective half-life, MRT0–∞ = mean residence time.
aMedian and range are presented.
![]()
DISCUSSION
In this study, response rate of IVIg-SN 10% was 75.7% in the ITT set, which are not inferior to those of other previously reported IVIg preparations.671415161718 Although there is a heterogeneity in defining response in previous studies of IVIg preparations, a cut-off platelet count of ≥ 50 × 109/L was used in the majority of studies,71516171819 and the response was defined at around one week after administration.71617 It is because response duration of IVIg is usually limited, and one of the main purposes of IVIg treatment is to stop bleeding or to reduce the risk of bleeding caused by severe thrombocytopenia.20 Therefore, in studies on IVIg, achieving response in early time is crucial. Although RIWG adapted more loose cut off for platelet count (≥ 30 × 109/L vs. ≥ 50 × 109/L) for defining a response, the estimated rate of RIWG in our study was lower than the early response rate. The result suggests that RIWG better reflects the sustainability of platelet count elevation rather than early response, because IWG criterion obligates the maintenance of platelet count ≥ 30 × 109/L on two separate occasions at least 7 days apart from each other. Another reason why we used increase of platelet counts ≥ 50 × 109/L in 7 days as primary endpoint is that there is a scarce of historical data regarding RIWG in previous studies of IVIg formulations. Moreover, a notable disadvantage of the IWG criteria is that the response rate may be fluctuated according to the frequency of platelet count measurement. For the very accurate estimation of RIWG and CRIWG, even daily measurement of platelet counts may be required.16 Accordingly, for the estimation of the efficacy of IVIg formulations, we believe that the response criterion we used would be a more realistic primary endpoint than the criterion for response recommended by the IWG at the Vicenza Consensus Conference.12
ITP is now classified into three phases based on time from diagnosis to reflect the possibility of spontaneous remission.112 In adults with newly diagnosed ITP, some may have a self-limited disease course, as in childhood ITP secondary to viral illness.21 Although patients with persistent ITP failed to achieve spontaneous remission or maintain response after therapy cessation between 3 to 12 months after diagnosis, they have chance of remission without more aggressive treatment, such as splenectomy.12 In the studies on IVIg treatment for ITP, inclusion criteria differ widely between studies, for example, some studies enrolled pediatric or adolescent patients as well as adults,616 and others excluded patients with newly diagnosed ITP.61718 In this study, we included all phases adult ITP and found no significant difference of response according to ITP phase. Furthermore, the receipt of previous corticosteroid and/or immunosuppressant treatment was not associated with rate of the response. However, because of limited sample size, this topic requires further evaluation.
Rapid time to achieving platelet count of ≥ 50 × 109/L, mean 9.13 days of maintaining a platelet count of ≥ 50 × 109/L suggest that our study drug would be effective at treating patients with ITP. Mean platelet count at day 29 was slightly higher than that at day 22 possibly because of the inclusion of some late responders or patients with acute ITP that underwent spontaneous remission.112
We thoroughly investigated AEs during the study period and less than half of the 283 identified AEs were definitely or probably drug-related. As observed for other preparations, the AEs of IVIg-SN 10% were manageable, and most were transient and of medium severity. Because the use of IVIg-SN 10% did not significantly increase the risk of infusion-related AEs or SAEs compared to other 5% IVIg preparations, IVIg-SN 10% is probably more convenient because its higher concentration would reduce infusion times. As has been reported previously,671617 headache is the most common AE and affects more than 40% of patients. However, headaches are not clinically significant because they are easily controlled with acetaminophen and/or antihistamines. SAEs occurred in 5 patients, and only one was drug-related. The incidences of SAEs and the two hemorrhagic SAEs encountered in the present study suggests that our cohort included severe thrombocytopenic patients. Nonetheless, because they were not drug-related and all patients with SAE recovered without sequelae, we believe IVIg-SN 10% is a safe preparation. Furthermore, most drug-related AEs occurred within 72 hours, which suggests the majority of drug-related AEs were infusion-related or caused by early reaction.
The benefit of ITP treatment can be assessed by recovery from bleeding or the risk of bleeding as well as by measuring platelet count increases. Although estimations of the severity of bleeding are inevitably subjective, objective tools132223 can be used to determine actual clinical benefit. In the current study, we used the IBLS13 and found that bleeding, especially mucocutaneous bleeding was effectively reduced after administering IVIg-SN 10%.
Because the study drug was IVIg, non-compartmental analysis may not have accurately estimated volume of distribution. One of the assumptions of non-compartmental PK analysis is that the study drug is eliminated in central compartments, such as, in plasma.24 However, the assumption is not valid for macromolecules like IVIg. Overall our PK data showed that IVIg-SN 10% has the PK characteristics expected of an effective IVIg formulation. Furthermore, its estimated in vivo half-life of 28.9 days suggests that IVIg-SN 10% has a long-lasting therapeutic effect.
The present study is limited by a relatively high screening failure rate (22.8%). One of the reasons for this is that we excluded patients without baseline serum IgG, IgA, and IgM level results. However, these tests could not be performed within 24 hours in most institutions, and thus, some patients did not obtain results before study drug infusion. Although it is important that patients with IgA deficiency be excluded to prevent anaphylaxis, it is well known that Asians have significantly lower prevalence of IgA deficiency than Caucasians.252627 In the present study, only one patient was excluded from PP analysis after IVIg infusion because of an IgA level slightly lower than normal. Nonetheless, no infusion-related AE occurred in this patient. IVIg infusion is often indicated to achieve a rapid increase of platelet count in emergent situations to avoid hemorrhagic risk. Based on our results, in regions with a low epidemiologic incidence of IgA deficiency, it may be reasonable to administer IVIg without waiting for confirmation of no IgA deficiency.
Compared to other IVIg formulation, IVIg-SN 10% has advantages of convenience of infusion by reducing infusion time, safety from infection and thromboembolism through viral inactivation/elimination procedures and purification using cold ethanol precipitation and chromatographic steps. IVIg-SN 10% has higher pH (4.8) compared to previous 5% IVIg solutions, which enables better stability. IVIg-SN 10% used glycine as a stabilizer instead of maltose, which may cause acute kidney injury.8
In conclusion, the IVIg-SN 10% formulation was found to be effective, safe, and convenient for the treatment of adult patients with primary ITP.
 XML Download
XML Download