

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prognosis for glioblastoma multiforme (GBM) patients remains poor despite advances in surgical techniques, radiotherapy, and chemotherapy. The median overall survival (OS) is expected to be only 14.6 months after maximum safe resection and irradiation with concurrent and adjuvant temozolomide (TMZ) chemotherapy. In spite of multimodal therapies, most patients suffer recurrence and die within 40 weeks,12 and there is no consensus on treating recurrent and TMZ-refractory GBM. Bevacizumab, a humanized monoclonal antibody against vascular endothelial growth factor A, has shown significant biological activity in patients with recurrent GBM and has been under investigation with other target agents.3 Re-challenge with alternative-dose TMZ for recurrent GBM can be recommended even if the patient has a history of standard TMZ chemotherapy.45
Nitrosourea has become a second choice after TMZ for malignant gliomas.6 Retrospective and subgroup analyses suggest higher efficacy for procarbazine, CCNU (lomustine), and vincristine (PCV) chemotherapy than for TMZ in patients with anaplastic glioma, with good prognosis as well.78 With the PCV triple-drug regimen, CCNU (110 mg/m2, day 1) and procarbazine (60 mg/m2, days 8–21) are administered orally but vincristine is administered intravenously (maximum 2 mg, days 8 and 29). The molecular weight of vincristine is 825 daltons, so that it has less permeability through the blood-brain barrier.9 It is well-known that vincristine is associated with neurotoxicity and could impair the quality of life in brain cancer patients, and the number of outpatient visits will decrease by omitting intravenous administration of vincristine. Authors of one study reported that reducing CCNU dose by 30% reduced the hematological toxicity (grade 3/4) from 25.6% to 13%.10 Based on these findings, we designed a modified procarbazine and CCNU therapy protocol for treating recurrent GBM with O6-methylguanine-DNA-methyltransferase (MGMT) promoter methylation. The purpose of this study was to evaluate the feasibility of the procarbazine and CCNU chemotherapy for recurrent GBM with MGMT promoter methylation.
METHODS
Study population
We enrolled patients at least 20 years of age who had been diagnosed with pathologically confirmed GBM with MGMT promoter methylation, which we assessed by methylation-specific polymerase chain reaction (PCR); we allocated patients with recurrent GBM with an unmethylated MGMT promoter to another trial. Radiographically confirmed tumor progression by magnetic resonance imaging (MRI) following standard external beam fractionated radiotherapy and TMZ chemotherapy was required for enrollment, along with a minimum Karnofsky performance status of 60, adequate hematologic, hepatic, and renal function, and at least a two-week period from any prior surgery or other chemotherapy. The following patient groups were excluded: 1) those with other cancer history, 2) those who had been treated with CCNU or procarbazine, and 3) those with leptomeningeal seeding.
Treatment schedule
The patients had previously been treated with concurrent chemoradiotherapy (CCRT) with adjuvant TMZ following the initial diagnosis of GBM. We determined recurrence by MRI scans assessed using the Response Assessment in Neuro-Oncology criteria. CCNU (75 mg/m2) was administered on day 1 and procarbazine (60 mg/m2) was administered through days 11 and 24 every 4 weeks. Administration of CCNU and procarbazine was repeated every 28 days for up to 6 months. We evaluated all toxicities according to the Common Terminology Criteria for Adverse Events version 4.0. All patients underwent brain MRI at the baseline within two weeks of starting CCNU, and they were evaluated by laboratory examinations of blood and neurological evaluation every four weeks; they also underwent gadolinium-enhanced brain MRI after every two cycles of chemotherapy (i.e., every eight weeks). Specifically, we required stable or decreasing corticosteroid dose and stable or improved fluid-attenuated inversion recovery abnormality for a rating of complete response, partial response, or stable disease based on complete, partial, or no decrease in the enhancing tumor burden on standard post-gadolinium T1-weighted sequences.
Study design and statistical analysis
We calculated the sample size using the following formula:

where n is the required sample size, p is the known response rate, 0.15, q is 0.85 (1−p), α is 0.05, and d is the drop rate, 0.05. Approximately 52 patients needed to be enrolled for the study to achieve a difference from the historical control.
Progression-free survival (PFS) was the primary end point of this study. Secondary end points were OS using Kaplan-Meier estimation and safety of combining CCNU and procarbazine in patients with recurrent GBM.
We estimated PFS from the start of CCNU and procarbazine administration to tumor progression or dropout from the study and OS from the start of CCNU and procarbazine administration to the date of death, irrespective of its cause. We assessed PFS and OS by the Kaplan-Meier product-limit method for all patients using SPSS software version 18.0 (IBM Corp., Chicago, IL, USA).
RESULTS
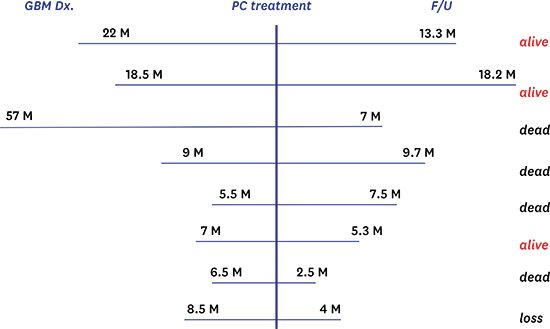
The patients were four males and four females with a median age of 56.5 years (range: 23–67), and their median Karnofsky performance scale at enrollment was 80% (range: 60–100). All patients had previously been treated with CCRT and adjuvant TMZ chemotherapy but no other chemotherapy or targeted agents. The median time between the initial GBM diagnosis and enrollment in the study was 8.75 months (range: 5.5–57).
The median cycle of CCNU and procarbazine was 3.5 (range: 2–6). Seven patients and one patient, respectively, achieved disease progression and stable disease following the administration of CCNU and procarbazine (Table 1).
Table 1
Patient characteristics

CCRT = concurrent chemoradiotherapy, TMZ = temozolomide, KPS = Karnofsky performance scale, F/U = follow-up, PD = progression of disease, SD = stable disease.
![]()
The median PFS for CCNU and procarbazine therapy to treat recurrent GBM was eight weeks (range: 5–73). PFS rates were 25% and 12.5% at 16 and 30 weeks, respectively, and the median OS from the start of CCNU and procarbazine administration to death was 9.7 months (95% confidence interval: 6.7–12.7, Fig. 1). The median OS from the initial diagnosis was 40 months. Serious adverse events are summarized in Table 2. Grade 3 toxicities including elevated hepatic enzyme and leukopenia developed in two patients, but they recovered following the delay of CCNU and procarbazine administration. In one patient, generalized muscle weakness developed and recovered without delay of the chemotherapy schedule. One patient had disseminated intravenous coagulation three times during follow-up period and was given conservative care.


DISCUSSION
In this study, the median PFS was two months in recurrent and TMZ-refractory GBM patients treated with modified CCNU and procarbazine chemotherapy; all patients had received radiotherapy with concomitant TMZ and cyclic TMZ therapy but no other cytotoxic agents or target therapies. CCNU is increasingly considered an alternative chemotherapeutic agent for GBM treatment because no other treatment has yielded better results in a controlled clinical trial, but PFS rates at six months are only in the range of 15%–25% with CCNU therapy.1112 The first randomized trial of PCV versus TMZ in chemotherapy-naïve patients with recurrent malignant glioma found that median PFS was 3.6 months with PCV and 4.7 months with TMZ (P = 0.229). In one study,13 the proportions of patients with at least one grade 3/4 adverse event were 9.2% and 12.2% in the PCV and TMZ arms (P = 0.40), respectively, and in a single-institution analysis, grade 3/4 hematological toxicity occurred in 25.6% of patients with recurrent GBM during traditional PCV chemotherapy.10
The characteristics of our protocol were that we omitted vincristine administration and we reduced the CCNU dose to increase the treatment's tolerability. Vincristine adds toxicity and CNS penetration is suboptimal,141516 and a retrospective analysis of CCNU and procarbazine versus PCV for grades 2 and 3 oligodendrogliomas presented no differences in PFS or OS.1718 A greater proportion of patients experienced neutropenia with PCV, but only those who received vincristine experienced neurotoxicity (14% vs. 0%). The NOA-05 multicenter trial analyzed the efficacy of traditional CCNU and procarbazine chemotherapy in patients with gliomatosis cerebri, and these patients achieved median PFS of 14 months. During 124 cycles of chemotherapy, authors observed grade 3/4 hematological toxicity in 15% of patients.19
There are no clinical publications that address whether CCNU and procarbazine can be substituted for PCV for newly diagnosed or recurrent GBM. We here attempted to assess the feasibility of modified CCNU and procarbazine chemotherapy for recurrent, TMZ-refractory GBM. We searched for clinical articles using the keywords “recurrent,” “glioblastoma,” “chemotherapy,” and “Korea” in PubMed (Table 3).20212223 We excluded articles about radiation therapy or radiosurgery. TMZ and the combination of ACNU and cisplatin were analyzed in three reports and one report, respectively. ACNU and cisplatin regimen had myelosuppression issues.20 Two reports analyzed the efficacy of continuous low-dose TMZ administration for recurrent and TMZ-refractory GBM. They showed different outcomes in terms of PFS and OS.2223 In the phase II RESCUE study (continuous TMZ 50 mg/m2/d), six-month PFS was 23.9% in patients with recurrent GBM.24 The efficacy of modified CCNU and procarbazine chemotherapy could be comparable with that of continuous low-dose TMZ therapy as a salvage therapy for recurrent GBM.
Table 3
Summary of clinical trials for recurrent glioblastoma treated with chemotherapeutic agents in Korea

![]()
It cannot yet be determined whether the dose reduction decreased hematological toxicities because of the small number of patients and the short follow-up. Although PCV increased survival among selected patients, its toxic effects led to many dose delays and reductions during the course of treatment, whereas during a total of 30 cycles of modified CCNU and procarbazine chemotherapy, only one cycle was delayed due to leukopenia.
This is the first prospective, multicenter clinical trial for GBM approved by the Korean Food Institute Institutional Review Board. The limitation of the study is the small number of patients. Following the statistic calculation, 52 patients needed to be enrolled to achieve a difference from the historical control; however, this trial terminated before the expected end date because of the progressive deterioration of patients with recurrent GBM and slow candidate enrollment. These experiences and information should encourage clinicians and clinical researchers to suggest more challenging clinical trials in the future.
In conclusion, our findings show marginal efficacy of modified CCNU and procarbazine chemotherapy. This clinical trial suggests the need to develop treatment strategies beyond CCNU and procarbazine for recurrent, TMZ-refractory GBM.
 XML Download
XML Download