

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
High heart rate (HR) is known to be associated with increased cardiovascular events and mortality in populations of various diseases, such as hypertension,1 coronary artery disease,2 and heart failure (HF).34 In particular, since the publication of the results of the systolic heart failure treatment with the If inhibitor ivabradine trial (SHIFT),5 resting HR as a modifying risk factor of HF has been highlighted. As a main HR-lowering agent, a beta blocker is the mandatory medication in the management of heart failure with reduced ejection fraction (HFrEF) along with angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs). Although various aspects of pleiotropic benefits of a beta blocker had been suggested,6 a recent meta-analysis showed that the benefit of beta blockers in the management of HFrEF is mainly related to the reduction of HR.7 In addition, the magnitude of HR reduction in patients with HFrEF receiving beta blockers showed close correlation with improvement of all-cause mortality and left ventricular ejection fraction (LVEF).8
Although lowering the HR is considered to be very important, baseline high HR — which has a large portion of HR reduction — consistently showed an association with increased mortality in large randomized controlled studies, even after treatment with maximal tolerable doses of beta blockers.23 However, these trials were mainly conducted in western patients who are known to be less sensitive to beta blockers than Asian patients in terms of blood pressure (BP) and HR.910 Therefore, we hypothesized that Korean patients with HFrEF — who are known to be more sensitive to bisoprolol than western patients — would show more favorable outcomes in terms of left ventricular reverse remodeling (LVRR) when they achieved maximal HR reduction with high baseline HR (≥ 75 beats per minute [bpm]) after treatment with maximal tolerable doses of bisoprolol. Also, we compared the values of N-terminal prohormone brain natriuretic peptide (NT-proBNP) and global assessment score (GAS) according to baseline HR 75 bpm after treatment with bisoprolol.
METHODS
Study design and population
This is a prospective, multi-center, and observational study, conducted in 11 university hospitals in Korea. Ambulatory patients with new-onset HF were eligible for inclusion if they 1) were older than 18 years and younger than 80 years, 2) had symptoms of New York Heart Association functional class II–IV and 3) LVEF < 40% by modified Simpson's method. We excluded patients with grade II or III atrioventricular block, resting HR < 60 bpm, systolic BP < 100 mmHg, serum creatinine > 2.0 mg/dL, decompensated HF, myocardial infarction or cerebrovascular disease within three months, percutaneous coronary intervention or coronary artery bypass surgery within 6 months, serious valvular heart disease, heart transplantation, chronic obstructive pulmonary disease, contraindications to a beta blocker, and other serious systemic diseases.
Treatment protocol
Study patients received optimal treatment for HF (defined as any combination of diuretics and an ACE inhibitor/ARB) before starting bisoprolol. Cardiac glycosides could also be prescribed. As shown in Fig. 1, patients visited each hospital at an interval of two weeks and bisoprolol was up-titrated according to a pre-set schedule of 10 weeks. Bisoprolol was initially prescribed from 1.25 mg/day and increased by 1.25 mg at each visit up to 5 mg/day, and then by 2.5 mg until reaching a target dose of 10 mg/day. Dose titration of bisoprolol was monitored by other coordinating investigators, and if there was no contraindication to increasing bisoprolol dose (hypotension, bradycardia, dyspnea, or weakness), dose of bisoprolol was increased to the next dosage by the other coordinating investigators. During the phase of up-titration or maintenance, bisoprolol dose could be reduced when systolic BP was lower than 80 mmHg or HR less than 50 bpm, or if the patients developed decompensated HF.
 | Fig. 1Preset schedule of dose titration of bisoprolol. Bisoprolol was initially prescribed from 1.25 mg/day and increased by 1.25 mg at each visit up to 5 mg/day, and then by 2.5 mg until reaching a target dose of 10 mg/day. If there was no contraindication to increasing bisoprolol dose (hypotension, bradycardia, dyspnea, or weakness), bisoprolol was increased to the next dosage.NT-proBNP = N-terminal prohormone brain natriuretic peptide, GAS = global assessment score.
|
Outcome measurements
We performed paired 2D echocardiography and also evaluated NT-proBNP and GAS of HF at baseline and 6 months. We observed whether LVRR occurred at six months or not and compared baseline characteristics of patients with LVRR with those of patients without LVRR. We also compared values of NT-proBNP and GAS at baseline with those at 6 months. LVRR was defined as an increase in LVEF from ≥ 10% to a final value of > 35%, accompanied by a decrease in left ventricular end-diastolic dimension (LVEDD) ≥ 10% as assessed by echocardiography at six months. GAS was evaluated using a prepared questionnaire consisting of six points: markedly improved (5), moderately improved (4), mildly improved (3), no change (2), worsened (1), and unassessable (0).1112 In addition, we analyzed prognostic value of predetermined baseline HR (75 bpm) in terms of LVRR and also compared characteristics of patients with high baseline HR (≥ 75 bpm) with low baseline HR (< 75 bpm).
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) and compared by using t-test or Wilcoxon's rank-sum test. Categorical data was expressed as frequencies and percentages and compared by using χ2 test or Fisher's exact test. Continuous variables were compared using student t-test or by the nonparametric Mann-Whitney U test. In univariate analysis, variables that differed significantly between groups with and without LVRR were entered into a stepwise logistic regression analysis for identification of independent predictors of LVRR at baseline. To address the risk of overfitting in a multivariate logistic regression model, univariate logistic regression was performed for all variables included in the model, and two multivariate models were created using five predictors of LVRR with the best F statistic at baseline or five significant predictors of LVRR in previous stepwise logistic regression analysis. For all tests, a probability value of P < 0.05 was considered significant. All statistical analyses were performed using the statistical software SPSS (SPSS Inc., Chicago, IL, USA) version 19.0.
RESULTS
From October 2010 to August 2012, 186 patients with HFrEF were identified. However, a total of 157 patients were included in the analysis after several violation cases were excluded (Fig. 2). Baseline characteristics of patients are shown in Table 1. Mean age of study patients was 59 years old and 73% of patients were men. Patients with ischemic etiology of HF were 19% and approximately 90% of patients were taking ACE inhibitor or ARB at baseline. Mean value of LVEF was 28%.
 | Fig. 2Flow diagram of study patients. A total of 157 patients were included in the analysis after exclusion of several violation cases were excluded. Finally, 112 patients with high baseline HR (≥ 75 bpm) and 45 patients with low baseline HR (< 75 bpm) were compared in the analysis.HR = heart rate, bpm = beats per minute, AV = atrioventricular.
|
Table 1
Baseline characteristics of study patients
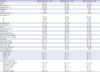
Values are expressed as mean ± SD or number (%). Data of patients with LVRR were compared with the remaining individuals at baseline.
LVRR = left ventricular reverse remodeling, COPD = chronic obstructive pulmonary disease, NYHA = New York Heart Association, GAS = global assessment score, ACE = angiotensin-converting enzyme, ARB = angiotensin receptor blocker, BMI = body mass index, BP = blood pressure, bpm = beats per minute, LVEDD = left ventricular end-diastolic dimension, LVESD = left ventricular end-systolic dimension, LVEF = left ventricular ejection fraction, LA = left atrium, NT-proBNP = N-terminal prohormone brain natriuretic peptide, BUN = blood urea nitrogen, SD = standard deviation.
P values for comparison between patients with and without LVRR are aP < 0.05; bP < 0.01; and cP < 0.001.
![]()
LVRR was identified in 49 patients (32%). Baseline characteristics related to the subsequent LVRR in the univariate analysis were as follows: young age, non-ischemic cause, favorable GAS, use of anti-aldosterone agent, high dose of bisoprolol, high diastolic BP, and high baseline HR (≥ 75 bpm). In multivariate analysis, five clinical variables showed independent predictive values for LVRR: use of anti-aldosterone agent, young age, high diastolic BP, favorable baseline GAS, and high baseline HR (≥ 75 bpm; Table 2). Notably, high dose of bisoprolol (≥ 3.75 mg/day) was eventually eliminated statistically in the multivariate analysis and was not related to LVRR.
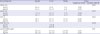
Table 2
Independent predictors for LVRR


Multivariate logistic regression of five predictors with statistical significance in stepwise logistic regression. Variables included in stepwise logistic regression: age, ischemic etiology, baseline GAS, anti-aldosterone agent, bisoprolol dose, diastolic BP, and HR ≥ 75 bpm.
LVRR = left ventricular reverse remodeling, OR = odds ratio, CI = confidence interval, BP = blood pressure, HR = heart rate, GAS = global assessment score.
![]()
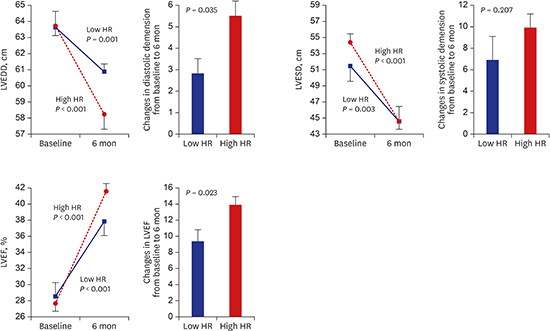
When compared according to baseline HR 75 bpm, only baseline systolic BP and the magnitude of HR reduction at 10 weeks and six months differed between high HR (≥ 75 bpm) group and low HR (< 75 bpm) group. Notably, resting HR achieved after 6-month bisoprolol treatment did not differ statistically between the two groups (67 vs. 71 bpm). Favorable effect of high HR in terms of LVRR seemed to be due to great magnitude of HR reduction in patients with high HR (≥ 75 bpm) after treatment with bisoprolol (Δ HR after 6 months: 1 vs. 18 bpm, P < 0.001; Table 3). LVRR occurred significantly more in the high HR group compared with low HR group. (37.5 vs. 15.6%, P = 0.008) after bisoprolol treatment. Although both low and high HR groups showed improved echocardiographic parameters — such as LVEDD, left ventricular end-systolic dimension, and LVEF — after bisoprolol treatment, more favorable morphologic improvement, including LVRR, was observed in high HR group which showed greater magnitude of HR reduction (Table 4, Fig. 3).
Table 3
Characteristics of the study patients according to baseline HR

Values are expressed as mean ± SD or number (%). Data of patients with high baseline HR (≥ 75 bpm) were compared with the remaining individuals at baseline.
HR = heart rate, COPD = chronic obstructive pulmonary disease, NYHA = New York Heart Association, ACE = angiotensin-converting enzyme, ARB = angiotensin receptor blocker, BMI = body mass index, BP = blood pressure, BUN = blood urea nitrogen, bpm = beats per minute, SD = standard deviation.
P values for comparison between patients with high (≥ 75 bpm) and low (< 75 bpm) heart rate are aP < 0.05; bP < 0.01; and cP < 0.001.
![]()
Table 4
Changes of echocardiographic parameters, log NT-proBNP, and GAS after 6-month treatment of bisoprolol
NT-proBNP = N-terminal pro b-type natriuretic peptide, GAS = global assessment score, HR = heart rate, LVEDD = left ventricular end-diastolic dimension, LVESD = left ventricular end-systolic dimension, LVEF = left ventricular ejection fraction, LVRR = left ventricular reverse remodeling.
![]()
 | Fig. 3Changes of echocardiographic parameters after 6-month treatment of bisoprolol. Although both low and high HR groups showed improved echocardiographic parameters, more favorable morphologic improvement was observed in high HR group. Vertical bars mean standard error of the mean.HR = heart rate, LVEDD = left ventricular end-diastolic dimension, LVESD = left ventricular end-systolic dimension, LVEF = left ventricular ejection fraction.
|
In terms of NT-proBNP and GAS, beneficial effects of bisoprolol were also indicated only in patients with high baseline HR (≥ 75 bpm; Table 4, Fig. 4). In patients with low baseline HR (< 75 bpm), the extent of improvement in terms of NT-proBNP and GAS was not statistically significant.
 | Fig. 4Improvement of NT-proBNP and GAS after treatment with bisoprolol according to baseline HR 75 bpm. Improvements of log NT-proBNP and GAS were only indicated in patients with high baseline HR.NT-proBNP = N-terminal prohormone brain natriuretic peptide, GAS = global assessment score, HR = heart rate, bpm = beats per minute.
|
DISCUSSION
In the management of patients with HFrEF, HR reduction and target dose of beta blocker have been one of the main concerns. Although most of HF guidelines recommend titration of beta blocker dose up to target dosages based on the pivotal clinical trials of beta blockers,1314 some reports have suggested that the main benefits of beta blockers might result from HR reduction, not dose of beta blocker.715 Meanwhile, although patients with a high baseline HR have a larger portion of achievable HR reduction than patients with low baseline HR, they have been consistently associated with increased adverse cardiovascular outcomes even in clinical trials in which a maximal tolerable dose of beta blockers was used.23416 This finding might result from insufficient HR reduction in spite of target dose of beta blocker and also insensitivity to beta blockers in some western patients with HFrEF. Additional HR reduction in HFrEF patients with treatment of beta blockers has already been shown to be beneficial in terms of mortality in the clinical trial, evaluating a heart-rate modifying agent, ivabradine.5 In addition, most of landmark clinical trials regarding beta blockers rarely included any Asian patients with HF, who might have different genetic inheritances to beta blockers.1718
Asian people are known to be more sensitive to beta blockers in terms of HR and BP than western people.9 In the SHIFT study, Asian patients showed an association with not being on a beta blocker or being on a low dose of beta blocker.10 Besides, in real world practice, frequency of beta blocker use in Korean patients with HF was consistently lower (44%) than that of western patients.10192021 These reports highlight the difficulty of beta blocker use and high sensitivity to beta blockers in Korean HF patients. On the basis of this evidence, high baseline HR in Korean patients with HFrEF seems to have different clinical significance in the management of HFrEF. In the current study, high baseline HR, not achieved HR at 10 weeks or 6 months, showed independent association with LVRR after maximal tolerable dose of bisoprolol treatment. This is clearly contrasted with previous reports, which consistently showed an association of high baseline HR with adverse cardiovascular outcomes in HF patients.234 However, in the SHIFT trial, patients with baseline HR higher than the median received greater event-reducing benefit from ivabradine than those with HR lower than the median.5 Therefore, we could assume that more cardiovascular events in western patients with high baseline HR might be due to insufficient reduction of HR. We could also presume that Korean patients with HFrEF and high baseline HR, who are more sensitive to bisoprolol, had a more beneficial effect in terms of LVRR after bisoprolol treatment because they mostly achieved maximal magnitude of HR reduction.
The advantages of high HR reduction in Korean HF patients, on condition of maximal tolerable dose of bisoprolol, encompassed not only LVRR but also NT-proBNP and GAS. NT-proBNP values improve with treatment of chronic HF,2223 with lowering levels of time correlating with improved clinical outcomes.2425 In addition to LVRR, which represents morphologic changes, NT-proBNP and GAS showed significant improvement in patients with high baseline HR (≥ 75 bpm) and high HR reduction. This finding also supports the favorable effects of high baseline HR (≥ 75 bpm) and HR reduction in Korean HF patients, in that greater morphologic, functional, and symptomatic improvements were achieved.
Lastly, although the low HR group, which showed only 1 bpm HR-lowering with bisoprolol treatment, had a trend to take low dose bisoprolol compared to the high HR group, they were very insensitive to bisoprolol in terms of HR. This finding tells us that there is heterogeneous response to bisoprolol in Korean HF patients who might have different levels of sympathetic nervous activity.
This study has several limitations. First, this study used surrogate markers of HF, such as LVRR and NT-proBNP. Therefore, direct comparison of the current study with large clinical trials, in which the primary endpoint was cardiovascular mortality, might be inappropriate. However, improvement of surrogate markers of HF such as LVEF or NT-proBNP showed consistent benefit of cardiovascular mortality and morbidity in previous clinical trials.122627 Second, reliability of regression analysis is driven by the number of events, multivariate models including more than five independent variables for prediction of 49 events might be inaccurate. Also, other clinical variables that were not included in the analysis could influence the result. Finally, the ischemic origin of HF patients was slightly lower (19%) compared with other cohorts of HFrEF.34 Due to different characteristics of current study patients, it could be inappropriate to generalize the results of the current study to other HF patients.
In conclusion, high baseline HR (≥ 75 bpm) showed an association with LVRR and improvement of NT-proBNP and GAS in patients with HFrEF after treatment with bisoprolol. This seems to be due to a large HR reduction in Korean HF patients. This finding supports the current concept of importance of HR reduction in management of patients with HFrEF.
 XML Download
XML Download