

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Streptococcus pneumoniae are encapsulated bacteria characterized by a polysaccharide (PS) capsule, which is a major virulence factor (1). S. pneumoniae is a predominant cause of many diseases, including meningitis, sepsis, pneumonia, and otitis media in young infants and the elderly (12). With the significant increase in multi-drug resistant S. pneumoniae worldwide, many efforts have been made to promote prevention of the disease and development of effective vaccines.
The 14-valent pneumococcal PS vaccine (PPSV) was licensed in 1977 (3) and thereafter, the 23-valent PPSV was developed in 1983. These vaccines induce T-cell-independent immune responses and are more effective in adults than in young children, who are the highest risk population for pneumococcal infection (4). To induce immunity in young children, the 7-valent pneumococcal conjugate vaccine (PCV7) containing serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F was developed. PCV7 was shown to be highly effective for the prevention of invasive pneumococcal disease in infants and children (56).
The efficacy of a vaccine is determined by the difference in the incidence of specific diseases among vaccinated and unvaccinated subjects for the disease. However, once a vaccine is proven to be effective, efficacy trials are no longer ethical or feasible to perform. Since protection against pneumococcal infection is mediated by antibodies specific to the capsular PS serotype, an enzyme-linked immunosorbent assay (ELISA) that measures immunoglobulin G (IgG) levels is used in the evaluation of pneumococcal vaccines as a surrogate assay. The World Health Organization (WHO) has provided a laboratory guideline for the ELISA to quantify IgG antibodies specific to pneumococcal PS (PnPS) since 2000 (78). In addition, the National Institute for Biological Standards Control (NIBSC) in the UK assembled 12 calibration serum samples with assigned antibody titers to assist laboratories working on the evaluation of pneumococcal vaccines (9).
The goal of this study was to validate the WHO ELISA for the serotype-specific anti-pneumococcal IgG at the Ewha Center for Vaccine Evaluation and Study. The results were anticipated to serve as evidence of the capability and accuracy of the evaluation of pneumococcal vaccines at our center.
MATERIALS AND METHODS
Materials
Study design
This was a validation study of the WHO ELISA for the detection of the serotype-specific anti-pneumococcal IgG at the Ewha Center for Vaccine Evaluation and Study.
Study supplies
The serum reference assay standard, 89-SF, was obtained from Dr. C. Frasch (Center for Biologics Evaluation and Research, Food and Drug Administration, Bethesda, MD, USA). The 7 serotype specific PS antigens (4, 6B, 9V, 14, 18C, 19F, and 23F) were purchased from the American Type Culture Collection (ATCC, Rockville, MD, USA). Cell wall PS (C-PS) used for the elimination of nonspecific reactivity was purchased from Statens Serum Institute, Copenhagen, Denmark. The PnPS 22F, which was selected for better absorption of the common nonspecific epitopes, was purchased from ATCC. For the test sera, 5 out of 12 pneumococcal ELISA calibration sera (748, 752, 754, 760, and 764, NIBSC, Hertfordshire, UK), which had been provisionally assigned for the detection of IgG concentrations for the 7 serotypes, were used.
The serum reference assay standard, 89-SF, was assigned as 4.1 μg/mL for PnPS 4, 16.9 μg/mL for PnPS 6B, 6.9 μg/mL for PnPS 9V, 27.8 μg/mL for PnPS 14, 4.5 μg/mL for PnPS 18C, 13.0 μg/mL for PnPS 19F, and 8.1 μg/mL for PnPS 23F (7). 89-SF for each of the serotypes was prepared at a 1:1,000 dilution with absorption solutions including only C-PS. The calibration sera 748, 752, 754, 760, and 764 were prepared at 1:250 dilutions with absorption solutions with C-PS and PS type 22F. The diluted sera were used at 2.5-fold serial dilutions up to 7 times with dilution ranges from 1/250 to 1/24,414. Each PnPS was prepared at a concentration of 2 mg/mL and was stored at −20°C. These were used in a concentration of a 5 μg/mL with phosphate-buffered saline buffer (containing both 0.02% sodium azide [NaN3] and 0.05% Tween-20).
ELISA
The standardized ELISA method for quantification of anti-PnPS antibodies, was conducted as previously reported, which can be located at http://www.vaccine.uab (89). Briefly, optimal concentrations of the 7 PnPS (1 μg/mL for 14 and 18C; 2 μg/mL for 4 and 9V; 10 μg/mL for 6B, 19F, and 23F) were coated at 37°C for 5 hours per 100 μL in 96 well medium binding polystyrene microtiter plate (Corning & Costar, Corning, NY, USA). Sera at 1:1,000 dilutions of 89-SF and 1:250 dilutions of calibration sera were pre-absorbed for 30 minutes at room temperature with each prepared solution, and were then diluted by 2.5-fold serial dilution. Coated plates with each PnPS were washed 5-times using a 30 to 60 seconds soak during the first wash with Tris-buffered solution (TBS) including 0.1% Brij™ 35 solution (Thermo Fisher Scientific, Waltham, MA, USA). Fifty microliters of all sera were added to the washed plates and incubated for 2 hours at room temperature. To each microtiter plate well, 100 μL of 1:2,000 diluted goat anti-human IgG alkaline phosphates conjugate (Southern Biotech, Birmingham, AL, USA) were added and incubated for 2 hours at room temperature. Next, 100 μL of a 1 mg/mL concentration of P-nitrophenyl phosphate in diethanolamine-MgCl2 buffer, pH 9.8, was added to all wells for 1 hour. The reaction was stopped by the addition of 50 μL of 3M sodium hydroxide (NaOH) per well. Absorbance readings were obtained with dual wavelength readings at 405 nm (experimental) and 690 nm (reference) on a microtiter plate reader.
ELISA validation test
All the tests for the validation were done in concordance with the bioanalytical method validation of Center for Drug Evaluation and Research (CDER) and the pneumococcal ELISA standardization-calibration sera of the NIBSC, UK written in April 26, 2001 (8). The overall acceptable ranges were defined as laboratory-determined antibody values of ELISA calibration sera with no more than 40% error related to the assigned values.
Specificity
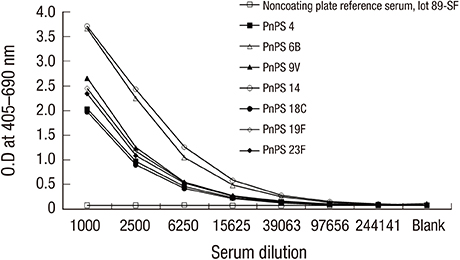
Specificity was defined as the ability to selectively and precisely evaluate the anti-pneumococcal IgG antibodies regardless of the presence of other components in the testing sample. To evaluate specificity, 8 plates were analyzed; 7 plates coated with 1 of 7 PnPS (4, 6B, 9V, 14, 18C, 19F, and 23F) and 1 plate with no coated antigen. The 89-SF and calibration sera were analyzed for the 8 plates and optical density (OD) was analyzed at different sera dilutions; the results were compared between the antigen-coated plates and antigen-free plate for each PnPS.
Precision
The precision was defined as the closeness of test results obtained by the values of the same analytes in a short period under the same conditions, evaluated using reproducibility and intermediate precision. For reproducibility, all 5 calibration sera were evaluated in 5 separate assays for all 7 serotypes and the coefficient of variability (CV) was assessed between the 5 assays. For intermediate precision, each serum was analyzed 7 times in a single plate for each serotype and the CV was assessed between the results of the assays.
Accuracy
Accuracy was defined as the degree of agreement of a measured quantity to its actual value. The antibody titers for each serotype were compared with provisional assignments of ELISA calibration sera. Accuracy was evaluated by the results of 24 tests analyses for 7 anti-PnPS.
Spiking recovery test
The spiking recovery test, a method to evaluate the accuracy, was analyzed by adding a known amount of analyte to the reference serum. Recovery was calculated by comparing the observed concentration as determined by ELISA and the expected concentration by summation. Acceptable ranges for recovery were defined as 100% ± 40% between results of multiple analyses at different dilution concentrations.
In this analysis, calibration serum 742 was used. The assigned values of calibration serum 742 were 6.2 μg/mL for PnPS 4, 9.9 μg/mL for PnPS 6B, 2.1 μg/mL for PnPS 9V, 7.4 μg/mL for PnPS 14 and 18C, 11.5 μg/mL for PnPS 19F, and 0.9 μg/mL for PnPS 23F. The calibration sera (serum 742) were diluted with 3 different dilutions of 1/40, 1/80, and 1/160. The diluted sera at each different dilution were mixed with a selected concentration of calibration sera, which was the lowest antibody concentration serum among 5 different calibration sera for each serotype.
Lower limit of quantification (LLOQ)
The LLOQ evaluated the accuracy and precision of the lowest concentration of serum that could be quantified. The quantitation limit for the type specific serotypes was calculated with the detection limit multiplied by 3, which was estimated in every analysis.
Stability
The stability of analytes evaluated the consistency of results in conditions likely to be encountered during sample handling and analysis. For the test, all 5 calibration sera were used.
The freeze-thaw stability of analytes was tested to evaluate the effect of the freeze thaw cycles of the analytes. The 5 calibration sera repeated the freeze thaw cycle from 1 to 4 times where sera were kept at room temperature for 30 minutes after stored in −20°C for more 12 hours.
The short-term temperature stability of analytes was tested to evaluate the effect of the kept time of analytes. The 5 calibration sera were kept at room temperature for 1, 2, and 4 hours.
Statistical analysis
OD was measured using SoftMax Pro 4.8 program of Molecular Devices Corporation (Sunnyvale, CA, USA). The OD was converted to antibody concentrations with a computer program for pneumococcal antibody ELISA that was developed by Mr. Brian Plikaytis at the Center for Disease Control and Prevention (CDC) in Atlanta, Georgia. The CV, standard deviation (SD), and mean OD for the standard of the each plate were calculated using standardized curve-fitting 4 parameter logistic equation (4PL equation). The CV, recovery, and the relativity of antibody concentrations were calculated to evaluate the validity.
The results were considered acceptable if they were within 40% error of the assigned value for the sera. For each of the validation assessments, acceptable ranges for reproducibility and intermediate precision were defined as CV ≤ 15% and CV ≤ 20%, respectively. Spiking recovery tests were analyzed by comparing observed concentrations with expected concentrations; they were deemed acceptable if test results were within 100% ± 40%. Stability (freeze thaw stability and short term temperature stability) was considered acceptable when CV ≤ 20%.
Ethics statement
This was a validation study on an analytical lab test (anti-IgG pneumococcal ELISA), using reference and calibration serum samples which are widely distributed by the FDA and NIBSC, UK. As the objective of this study was to validate results of the assay, and not directly analyze serum samples, this work did not receive an Institutional Review Board approval. Also as the serum samples were not directly obtained from human subjects in our study, there was no need for informed consent.
RESULTS
Specificity
The specificity of the pneumococcal ELISA was evaluated for 7 serotypes to PnPS antigens with optimal coating concentrations and with a blank plate with no antigen coating. The 89-SF and 5 calibration sera showed that the OD decreased with dilution. The value of the 5 calibration sera corresponded to each provisional IgG value. The non-coating wells were estimated with a similar level of blank wells regardless of the dilution fold and PnPS antigen serotype (Fig. 1).

Precision
The reproducibility measures were generally within the acceptable range with the exception of the calibration serum 764 for PnPS 9V (Table 1).
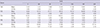
Table 1
Reproducibility precision results of 5 calibration sera for 7 anti-PnPS (acceptable range: CV ≤ 15%)
![]()
The intermediate precision measures were within the acceptable range when compared with the provisional assigned values. When comparing CV, the measures were within the acceptable range with the exceptions of calibration serum 752 for PnPS 14, calibration serum 760 for PnPS 9V, and calibration serum 764 for PnPS 4 and PnPS 6B (Table 2).
Table 2
Intermediate precision results of 5 calibration sera for 7 anti-PnPS (acceptable range: CV ≤ 20%)

![]()
Accuracy
Accuracy was evaluated by measuring the correlation between the provisional assigned values and the obtained results from 24 runs for 7 serotypes. There were good correlations for all serotypes including PnPS 4, 14, 18C, 19F (r = 0.99), PnPS 6B (r = 0.97), PnPS 9V (r = 0.96), and PnPS 23F (r = 0.94).
Spiking recovery test
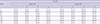
The calibration serum 742 was used to test for 7 serotypes. The results were within the acceptable range for 5 serotypes, with the exception of PnPS 6B and 19F (Table 3).
Table 3
Spiking recovery* test of calibration serum 742 with 1/250 dilution and with the lowest antibody concentration serum in the middle of 5 sera tested in this assay for each anti-PnPS (acceptable range: 100% ± 40%)

PnPS = pneumococcal polysaccharide.
*Recovery (%) = (observed concentration/expected concentration) × 100.
![]()
LLOQ
The LLOQ was calculated by multiplying the detection limit, measured by the ELISA, by 3. The results were 0.05 μg/mL for PnPS 4, 0.086 μg/mL for PnPS 6B, 0.085 μg/mL for PnPS 9V, 0.073 μg/mL for PnPS 14, 0.058 μg/mL for PnPS 18C, 093 μg/mL for PnPS 19F, and 0.051 μg/mL for PnPS 23F.
Stability
Freeze-thaw stability
The 5 reference sera were subjected to 4 freeze-thaw cycles for 7 serotypes. The results ranged from 86.61% to 115.59%, within the acceptable range when compared to result from the first cycle (Table 4).
Table 4
FT stability of 5 calibration sera for 7 anti-PnPS (acceptable range: within ± 20%)
FT = freeze thaw, PnPS = pneumococcal polysaccharide.
*Freeze thaw cycle: sera were subjected to 4 freeze thaw cycles. †Relative to FT 1 (%) = (based upon mean value) FT 2/FT 1 × 100.
![]()
Short-term temperature stability
The 5 sera were placed at room temperature for 1, 2, and 4 hours and were then assessed using ELISA. The results ranged from 81.3% to 120.0%, within the acceptable range when compared to result of the 5 sera placed at room temperature for 1 hour (Fig. 2).

Percent error relative to the assigned values
When analyzing all the results from each of the validation analyses, the results were within 40% error for the majority of the antigens, with the exception of PnPS 6B and 23F for 2 and 1 calibration sera, respectively (Table 5).
Table 5
Performance of Ewha Center for Vaccine Evaluation and Study for the analysis of 5 calibration sera-shown is the number of sera whose assayed value has a percent error ≤ 40%

| Value | PnPS | |||||||
|---|---|---|---|---|---|---|---|---|
| 4 | 6B | 9V | 14 | 18C | 19F | 23F | All types | |
| No. of serum samples (%) | 5/5 (100) | 3/5 (60) | 5/5 (100) | 5/5 (100) | 5/5 (100) | 5/5 (100) | 4/5 (80) | 32/35 (91) |
![]()
DISCUSSION
In this study, we evaluated the validity of ELISA for quantitation of serotype specific anti-pneumococcal IgG antibodies at the Ewha Center for Vaccine Evaluation and Study. The specificity, precision, accuracy, spiking recovery test, LLOQ, and stability were analyzed for 7 serotypes (4, 6B, 9V, 14, 18C, 19F, 23F) included in the PCV7. The serum standard, 89-SF, and 5 calibration sera showed specificity in the detection of the IgG for the 7 PnPS antigens. The specificity is an important measure reflecting the ability to inhibit non-specific reactions and allowing for the analysis of the presence of precise anti-pneumococcal antibodies in a patient's serum (8910).
The reproducibility and intermediate precision analyses were generally within acceptable ranges (reproducibility, CV ≤ 15%; intermediate precision, CV ≤ 20%) for all 7 serotypes. The accuracy was proven by showing a high correlation when compared with the provisional antibody values of the calibration sera. The results of the spiking recovery test were also acceptable with the exception of PnPS 6B and 19F. However, previous studies have shown that there is variation within antibody values for the serotypes PnPS 6B, 9V, 19F, and 23F (11). According to the reference report of the pneumococcal ELISA standardization-calibration sera, 5 laboratories showed different results for each serotype and serum; disparity in PnPS 6B values between laboratories were speculated in that study (11). Our findings were consistent with results in the previous study. The LLOQ ranged from 0.05 to 0.093 μg/mL for the specific PS antigens, which are much lower than the surrogate for protection against pneumococcal diseases (0.2–0.35 μg/mL). The stability results were within the acceptable ranges, proving that measures were very stable during serum handling and storage, the freeze and thaw cycles, and the analytical process. Consequently, the validity for the evaluation of 7 pneumococcal specific anti-PnPS IgG using ELISA, conducted at the Ewha Center for Vaccine Evaluation and Study, was confirmed.
The ELISA is a sensitive and the plausible method in the biological field. Although the WHO ELISA protocol for anti-pneumococcal IgG antibody analysis is well described, each lab that performs the assay should be well validated. As a result, 12 research centers have suggested the need for guidelines detailing analysis methods for the antibody concentration and pneumococcal ELISA study using quality control sera (12). Provisional assignments of 12 calibration sera were established for each specific PnPS antigen. The Center for Biologics Evaluation and Research and CDC initially suggested that at least 85% of values for each serotype should have no greater than 40% error relative to the provisional assigned value (13). However, it was later agreed that when evaluating anti-pneumococcal IgG antibodies using ELISA, it is acceptable if 9 of the 12 sera are no greater than the 40% error criteria. In this study, although we used only 5 calibration sera, the results were within the acceptable criteria for most antigens with the exception of PnPS 6B and 23F. PnPS 6B relatively differs from other serotypes and the results in this study showed correspondence to results ascertained from other laboratories (111213).
After the validation assay was established at the Ewha Center for Vaccine Evaluation and Study, the IgG serotype-specific anti-pneumococcal antibody ELISA has been widely applied on various studies including infants (14) and also elderly subjects (15). This utility of ELISA for the quantitation of IgG serotype-specific anti-pneumococcal antibodies in human serum is not only limited to evaluating immunogenicity to vaccines, but also has been used to evaluate patients suspected with immune abnormalities (1617). Recently, it was used in the diagnosis of CD21 deficiency, which is a type of primary immunodeficiency; it showed impaired antibody responses to polysaccharides but intact antibody responses to protein antigens (18). Thus, there is a need for the anti-IgG pneumococcal ELISA in various settings, all of which need accurate, reproducible, and well-validated analysis methods.
This study was conducted for 7 pneumococcal capsular serotypes. Further studies are needed for more serotypes using the new reference standard serum, 007sp, which has replaced 89-SF (1920).
In conclusion, the Ewha Center for Vaccine Evaluation and Study shows good performance in the use of the standardized WHO ELISA for serotype specific anti-pneumococcal IgG antibodies. The ELISA was effective in evaluating the immune response against pneumococcal vaccines with great consistency and accuracy.
 XML Download
XML Download