

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Middle East respiratory syndrome (MERS) is a lethal respiratory disease caused by MERS-coronavirus (MERS-CoV) and occurs mostly in the Middle East, initially by camel-to-human transmission, and then by human-to-human transmission. However, the disease was spread to other continents, probably by an index case, with subsequent pandemic outbreaks through human-to-human transmission through droplets and contact. During these respiratory viral outbreaks, pregnant women can be expected as highly vulnerable candidates for infection (1).
A MERS outbreak occurred in Korea in 2015 with 186 infections, including 38 deaths (23). We experienced a case of a Korean pregnant woman who was confirmed for a MERS-CoV infection via a polymerase chain reaction (PCR) test. This is the first case of a MERS-positive pregnancy reported outside the Middle East and is also the first case of having been exposed and confirmed on 3rd trimester of pregnancy with full-recovery and successful full-term delivery.
CASE DESCRIPTION
On May 27, 2015, the patient's mother was exposed to the 14th MERS patient, had a fever starting from June 3 and was diagnosed with MERS on June 7. While febrile, she had been in close contact with her daughter, a 39-year-old pregnant woman (gravida 2 para 1). On June 8 (35 weeks and 4 days of gestational age [GA]), this pregnant woman visited the emergency room complaining of mild myalgia. Based on this contact history with a MERS patient and her symptoms, a MERS-CoV PCR test was performed and the result was found to be positive on June 9. Starting from June 9, the patient developed dyspnea and sputum production. Although chest auscultation was normal, the oxygen saturation (SpO2) was 95% in room air and chest radiography showed diffuse opacity in the left lower lung area compared to a previously obtained radiographic image. The laboratory findings included a leukocyte count of 5,570/mm3 (normal range 4,000–10,000/mm3), with a differential of 71.4% segmented neutrophils, 20.5% lymphocytes, and 7.9% monocytes; and C-reactive protein level of 1.95 mg/dL (normal range 0–0.3 mg/dL). She was given supplemental oxygen for hypoxia and conservative treatment, with hydration and pain control. The antiviral agents used in other severe MERS-CoV patients were not used in this patient, because her symptoms and laboratory findings were not severe. Also, there was no evidence of any potential harm to the fetus and pregnant woman related to those drugs.
After several days, her dyspnea and myalgia improved. The SpO2 was 98% in room air and chest radiography showed interval improvement. On June 19 and 21, MERS-CoV PCR was performed and the results were negative. She had no symptoms related to MERS.
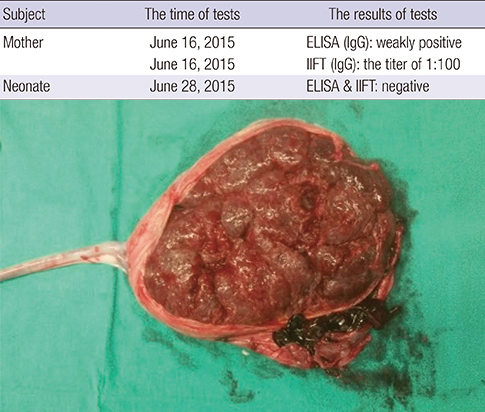
On June 23, the patient manifested abrupt vaginal bleeding with rupture of membranes. A fist-sized blood clot was found through speculum examination and she had abdominal pain. Fetal cardiotocography showed no deceleration, but a variability of fetal heart rate changed from moderate to minimal. With an impression of placental abruption, her obstetrical team decided on emergent cesarean delivery. A 3,140 g male newborn was delivered at 37 weeks and 5 days of gestation. Apgar scores at 1 and 5 minutes were 9 and 9, respectively. As expected, about 10% placental abruption was found (Fig. 1). After delivery, the baby was immediately moved to the airborne infection isolation room (AIIR) and received an initial care with all health care personnel (HCP) completely protected according to the Centers for Disease Control and Prevention (CDC) guidelines (4). MERS-CoV PCR tests and antibody tests were performed with umbilical cord blood and placenta, and all results were negative.
Fig. 1
A gross finding of placenta. Placenta abruption was observed as dark blood clot on the maternal side of placenta.

A systematic testing procedure for coronavirus infection, including chest radiograph and serial reverse transcription (RT)-PCR assays with peripheral blood and nasopharyngeal swab, did not demonstrate the presence of MERS-CoV in the newborn. MERS-CoV antibody tests were performed with mother and newborn sera on June 16 and June 28, respectively (5). In the mother's serum, immunoglobulin G (IgG) was detected, albeit weakly, (0.302) via enzyme-linked immunosorbent assay (ELISA; Euroimmun AG, Luebeck, Germany), and via indirect immunofluorescence test (IIFT; Euroimmun AG) with a titer of 1:100. IgM and IgA were not detected through ELISA and the plaque reduction neutralization test (PRNT) result was below the cutoff value. However, MERS antibodies for IgG, IgM, and IgA were not detected in the newborn's blood samples. (Table 1)
Table 1
Maternal and neonatal antibody tests for MERS
| Subject | The time of tests | The results of tests |
|---|---|---|
| Mother | 16-Jun-15 | ELISA (IgG): weakly positive |
| 16-Jun-15 | IIFT (IgG): the titer of 1:100 | |
| Neonate | 28-Jun-15 | ELISA & IIFT: negative |
The patient and her newborn baby were discharged in stable condition on June 30 with no clinical abnormalities on follow-up at the outpatient clinic.
DISCUSSION
MERS-CoV was first isolated from a patient who died from a severe respiratory illness in Jeddah, Saudi Arabia in June 2012 (6). Since then, more than 1,698 confirmed cases were reported to the World Health Organization (WHO). Clinical features of MERS are variable, and infected patients can be asymptomatic or have an acute febrile illness, upper respiratory tract disease, or even multiple organ failure resulting in death (7891011). However, there are limited data about the clinical features of MERS-CoV infection during pregnancy and the perinatal outcome of patients diagnosed with MERS-CoV infection. To our best knowledge, there have been 9 reported cases in which pregnant patients had positive laboratory results for MERS-CoV including this case (12131415) (Table 2). Unlike other cases, this case is not only the first MERS-CoV infection during pregnancy occurred outside of the Middle East, but also the first case of MERS confirmed on 3rd trimester of pregnancy showing good outcome of both mother and baby.
Table 2
Characteristics and outcomes of MERS-CoV infection during pregnancy
Currently, an exposure time to this virus during pregnancy and a severity of maternal disease could be expected to affect the perinatal outcome. However, there is limited knowledge about the clinical implications of MERS-CoV infection on the maternal, fetal, and placental aspects of pregnancy. From the maternal aspect, there is no epidemiologic data regarding whether pregnant women are more susceptible to MERS. Also, it is unknown whether MERS-CoV infected pregnant women have a more severe disease course compared with the non-pregnant population. In our case, she showed a mild disease course. She had low level of IgG antibody by ELISA and IIFT but not detectable neutralization activity by PRNT. It has been suggested that neutralizing antibodies are produced at low levels and are potentially short-lived after mild or asymptomatic MERS-CoV infection (1617). From the fetal aspect, it is unclear whether MERS was a causative factor in the stillbirth or preterm birth. Fetal specimen and/or placenta were not available for evaluation in the previous cases. As pregnancy alters maternal pulmonary function and consumes more oxygen, severe respiratory illness during pregnancy results in maternal hypoxemia. Maternal hypoxemia can be associated with poor fetal oxygenation, which eventually could lead to preterm birth or stillbirth. Also, altered immune responses during pregnancy could affect the fetal outcome (13). From the placental aspect, there have been no reports of MERS causing pathology of the placenta including infarction, insufficiency, or villus placentitis. Our case showed placenta abruption clinically, which can be caused by maternal infection. There is no evidence of a relationship between MERS-CoV and placenta disorder. However, the possibility that this virus may be a cause of placenta abruption should be of concern.
Lastly, the remaining question was whether the virus could cross the placenta causing significant infection in the fetus, and whether MERS could cause vertical transmission. Camel-to-human transmission, and human-to-human transmission via contact, droplet, and possibly airborne routes are the known modes of transmission (1819). However, there are no data about perinatal transmission of MERS-CoV. Moreover, if the mother mounts an appropriate immune response to produce enough neutralizing antibodies without serious conditions, passive antibodies transferred from mother to fetus may have a protective effect on the fetus. There is only one case reporting the mother's serologic data previously (15), in which stillbirth occurred at approximately 5 months of gestation, although the mother had MERS-CoV antibody by ELISA (titer 1:1,600), immunofluorescent antibody (IFA), and microneutralization titer assay (titer 1:80). In our case, although the mother had IgG antibody (titer 1:100 by IIFT), antibody was not detected in neonatal serum. This finding may provoke different interpretations in regard to the role of maternal antibodies in the fetus or to transmission of maternal antibodies, necessitating more data in the future. To know whether prenatal transmission of MERS-CoV can occur, collection of samples including amniotic fluid, placenta, and umbilical cord is needed from an infected pregnant patient.
Further studies with a larger sample size will help in understanding of the pathophysiology and perinatal outcome of MERS during pregnancy and the optimal mode of delivery.
 XML Download
XML Download