

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
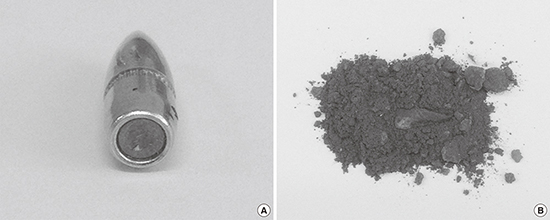
Awareness about lead poisoning in Korea has increased (1). Since 1972, all workers with lead exposure are placed under medical surveillance according to the Korean Industrial Safety and Health Act, which requires the blood lead concentration of these workers to be measured at least once every year. The blood lead levels (BLL) in Korea lead workers decreased every year and occupational lead poisoning has recently become rare (23). But, the military regularly consumes large quantities of ammunitions that contain lead. Recently, the Korea military outdoor firing ranges are being converted into indoor firing ranges. Indoor firing ranges with poor ventilation systems increase the risk of exposure to shooting by-products (e.g., heavy metals), compared to outdoor firing ranges (Fig. 1) (45). Thus far, in Korea, no special health management was undertaken for indoor firing range workers since they were not recognized as heavy metal exposure workers. Herein, we present a case of lead poisoning in a soldier who managed an indoor firing range, and who was treated at our hospital. Institutional improvements were implemented based on the findings of this case. In Korea, this is the first report of lead poisoning through this route. Through this case report, the risk of heavy metal poisoning in indoor firing ranges was confirmed, and institutional improvements in the work environment and health management of workers were implemented.

CASE DESCRIPTION
In March 2014, a 39-year-old Korean professional male soldier presented with a 6-month history of various nonspecific symptoms. He received hospital treatment and underwent several health examinations; however, no specific findings were observed. The symptoms were dizziness, fatigue, asthenia, irritability, elevated blood pressure (above systolic 160 mmHg), palpitation, eyestrain, and tinnitus, which aggravated with time.
The patient had an unremarkable medical history and was a current smoker (0.7 pack/day for 15 years). He consumed 700 mL of beer once a week. The patient had worked for 13 months in a newly constructed indoor firing range. He performed general management of the indoor firing range. His work included setting the firing range (preparing the bullets and targets) before the firing exercises, and cleaning and handling the disposed warheads after the firing exercises. There was much gray-black dust during the cleaning process; however, he did not wear any special protective equipment.
His BLL was measured owing to suspicion of heavy metal poisoning; 0.1 mL of whole blood was diluted with 0.8 mL 1%Triton™ X-100 (Sigma-Aldrich, St. Louis, MO, USA) and analyzed for BLL using graphite furnace atomic absorption spectrometry (novAA 400p;Analytik Jena AG, Jena, Germany). The BLL was estimated at 64 µg/dL; therefore, the patient was diagnosed with lead poisoning and immediately withdrawn from his work to avoid further lead exposure. The standard for elevated BLL among adults is 10 µg/dL, as determined by the Adult Blood Lead Epidemiology & Surveillance from the National Institute for Occupational Safety and Health (NIOSH) (5). The Occupational Safety and Health Administration (OSHA)'s occupational exposure limit for BLL is 40 µg/dL (6). Korean blood-lead criteria for the diagnosis of lead poisoning in workers is 40 μg/dL (7). The patient was immediately admitted to the military hospital and investigated thoroughly. His examination revealed elevated blood pressure (150/110 mmHg), and the peripheral blood smear showed poikilocytosis. The liver function test, renal function test, complete blood count, and differential count were within normal ranges. His urine tested negative for microproteinuria. According to the examination by the neurologist, there were no significant findings in the electromyography, nerve conduction velocity, brain magnetic resonance imaging, and neurologic tests. The hearing test indicated mild hearing loss (hearing threshold: right/left = 35/35 dB) at 4 kHz, and he was diagnosed with dry eye by the ophthalmologist; he received treatments from the respective departments.
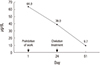
The treatment for lead poisoning included avoidance of the harmful factor (prohibition of work) for 3 weeks following which he underwent BLL measurement. The BLL was 39 µg/dL and the blood zinc protoporphyrin (ZPP) level was 45.1 µg/dL (reference range: 10–38 µg/dL). He showed no improvement of symptoms; hence, for an intensive BLL decrease chelation treatment was administered. For the chelation treatment, 1 gram of calcium-disodium ethylenediaminetetraacetic acid (CaNa2 EDTA) was mixed with 250 mL of 5% dextrose (JW Life Science Corp, Seoul, Korea) in water and was administered intravenously over 6 hours. The chelation treatment was given for 5 days, and the renal functions and liver functions were assessed daily. He completed 5 days of chelation treatment with no adverse effects. He was discharged after his blood pressure normalized (130/85 mmHg) and the subjective symptoms improved. Three weeks after the discharge (7 weeks after lead exposure avoidance), the BLL was 9.7 µg/dL (Fig. 2).
Fig. 2
Changes in the BLL of the patient with lead poisoning who worked at indoor firing ranges.
BLL = blood lead level.
As evident from the workplace environmental monitoring (April 2 to April 15, 2014), the exposure in the air was an 8hours, time-weighted average of 0.015–0.387 mg/m3, which exceeded the acceptable standards (0.05 mg/m3) (Table 1) (6). From the field investigations, it was confirmed that a swirl formed in the indoor firing range from inappropriate filter use (using a charcoal filter instead of a dust filter) and poor design of the ventilation system. The dust accumulated as it was not discharged outside the indoor firing range, and entered the body through the respiratory tract and oral intake before and after the firing and during cleaning and disposal of the warheads.
Table 1
Workplace environmental monitoring results of lead from indoor firing range

DISCUSSION
Because lead is very harmful to the body, having a lower BLL is preferable. Whole BLL is the most common and useful laboratory test to confirm lead exposure. Lead in blood is a reasonable reflection of the lead content of most soft tissues. BLLs above 5 µg/dL cause adverse health effects in adults. Hypertension, kidney dysfunction, and spontaneous abortions are known to occur if the BLL exceeds 5 µg/dL. Subclinical neurocognitive deficits and postnatal developmental delay in pregnant women can occur if the BLL is above 10 µg/dL. Reduced birth weight and postnatal developmental delay is possible in pregnant women with a BLL above 20 µg/dL; clinical neurocognitive deficits, above 30 µg/dL; subclinical peripheral neuropathy, anemia (heme synthesis disorder), colic, gout, and sperm abnormalities, above 40 µg/dL; and nephropathy, clinical peripheral neuropathy, and encephalopathy, above 80 µg/dL (8910).
Inhalation and ingestion are the primary routes of lead absorption. Airborne particle size influences overall transfer of inhaled lead to the blood, because as particles become larger they have a tendency to deposit in the upper airway and be translocated to the gut, rather than to deposit in the lower airway and undergo direct respiratory absorption. Approximately 35%–40% of inhaled lead is ultimately absorbed into the bloodstream. The extent to which ingested lead is absorbed into the blood is influenced in part by particle solubility (soluble particles undergo greater absorption), the mass of lead ingested, and the extent of coingestion with liquids or solid food (food in the gut decrease absorption). An estimated 15% of ingested soluble lead is absorbed in adults, compared to approximately 40%–50% in young children. Iron-deficiency and low calcium diets may increase gastrointestinal absorption (1112).
The essential first step in the management of lead intoxication is identification and elimination of the sources of overexposure. Chelating agents, such as parenteral CaNa2 EDTA (calcium disodium versenate) or oral dimercaptosuccinic acid (DMSA, succimer), decrease lead concentration in the blood and certain tissue. In general, chelation in adults should be reserved for those with markedly elevated BLL (e.g., > 80 µg/dL) or possibly symptomatic individuals with BLL > 50 µg/dL (10). CaNa2 EDTA that forms a metal chelate excretable by the kidneys is administered in either acute symptomatic lead poisoning or, during the course of chronic lead poisoning. Therapeutic daily doses up to 50 mg per kg, maximum rate of administration of 20 mg per minute, and total course of therapy restricted to 5 days in a typical treatment protocol. The medication is given intravenously in a dose of 1 to 1.5 grams in 250 mL 5% dextrose in water as a slow infusion over 1 hour, two times a day for 5 days (1314).
In this case, the patient's BLL was as high as 64 µg/dL; however, no disorders were confirmed in the target organs of lead poisoning, such as the kidneys, nervous system, and red blood cells (e.g., anemia). The blood ZPP level measured 24 days after harmful factor avoidance was 45.1 µg/dL, showing mild elevation. An elevation in ZPP reflects lead-induced inhibition of heme synthesis. Because there is a time lag associated with lead induced elevation in ZPP, the finding of elevated BLL with no concurrent increase in ZPP suggests that the lead exposure was of recent onset (1115). This was because the patient had worked for 13 months in the indoor firing range and the exposure was controlled before chronic damage progressed. Because of the findings from this case, all the workers of the indoor firing range within the military underwent complete investigation. Investigation of 120 workers revealed that the mean BLL was 11.3 ± 8.7 µg/dL (range: 2.0–64.0µg/dL), showing a high risk of lead exposure. All the indoor firing ranges within the military were temporarily shut down, and were scheduled to reopen after implementing regulations and supplementing ventilation facilities.
In many countries with developed firing culture, the risk of lead poisoning in indoor firing ranges has been recognized and managed (16171819). However, Korea prohibits guns. The firing culture is not prevalent other than in the military, and firing is partially approved for hunters and in private firing ranges for leisure. Therefore, there is extremely limited experience to indoor firing range construction. Ventilation system design and evaluation by a specialist is essential in constructing an indoor firing range, and safety guidelines for the disposal of warheads should be mandatory. This case represents the first report of occupational lead poisoning in a firing range in Korea. Institutional management is necessary to prevent more cases of poisoning through this route. After this case, periodical workplace environmental monitoring and special health examination of the workers according to the Korean Industrial Safety and Health Act became mandatory for indoor firing ranges within the military. There is no category defined for heavy metal exposure standards in the regulations of private firing range establishments in Korea; therefore, future consideration would be necessary in this aspect (20).
 XML Download
XML Download