

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Ischemic heart failure (HF) after myocardial infarction (MI) is the most common cause of HF and its incidence is 52% in Korea (1). Although infarct size is the main determinant of long-term mortality in patients with MI and reducing infarct size is essential for suppressing chronic ischemic HF (2), the effects of many pharmacological or non-pharmacological interventions with percutaneous coronary intervention were modest and the impact on clinical outcomes have not been well-studied (3). Stem cell therapy has emerged as a complement to these aforementioned modalities for reducing ischemic HF in patients with MI (4), and various routes can be used to deliver stem cells. Among these, percutaneous intramyocardial delivery is theoretically more effective than the intracoronary or surgical intramyocardial route for targeting the injection site, because it can use myocardial mapping system for the injection (5). Cell type may also be an issue. Mesenchymal stem cells (MSCs) are emerging as an extremely promising therapeutic agent for tissue regeneration (6). Despite the myocardial protective role of MSCs, the therapeutic capacity is limited after intravenous or intracoronary delivery (7). Therefore, this study investigated the effect of delivering MSCs by the percutaneous intramyocardial route, using a novel myocardial mapping system, on left ventricular (LV) systolic function recovery in a porcine MI model.
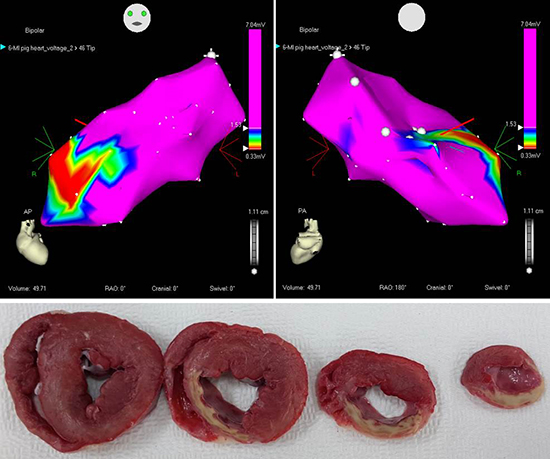
This study included 18 pigs (MI was induced by occluding the left anterior descending [LAD] coronary artery: 8 pigs received MSC treatment and 10 did not) from the animal catheterization laboratory of Chonnam National University Hospital. Yorkshire × Landrace F1 crossbred castrated male pigs (25 kg) were observed from the Laboratory Animal Center of Chonnam National University Medical Institute 7 days before the experiment. On the day of the procedure, the pigs were anesthetized and the left carotid artery was surgically exposed, and MI was induced with occlusion of LAD using a polyethylene terephthalate (PET) occlude. Porcine adipose tissue-derived mesenchymal stem cells (ATSCs) were isolated from abdominal subcutaneous white adipose tissue. To verify stemness of the porcine MSCs, adipogenic, chondrogenic, and osteogenic differentiation was induced using Stem Cell Differentiation Kits (Invitrogen Life Technologies, Carlsbad, CA, USA). These cells were used in the experiment at passages 3–4 and 1 × 107 cells were injected into each animal. After 1 week of MI, a total of 8 acute myocardial infarction (AMI) pigs received ATSC injections via intramyocardial route after LV mapping. The transthoracic echocardiography (TTE) was performed before injecting the ATSCs, and again after 4 weeks, in 8 MI pigs to examine the LV ejection fraction (EF) which represents LV systolic function. TTE was also done at the same time in 10 control MI pigs. Images were taken using a conventional cardiac ultrasound system (Vivid S3; GE Healthcare, Schenectady, NY, USA) under general anesthesia while the pigs were in the supine position. LV end-systolic volume (LVESV) and end-diastolic dimensions (LV end-diastolic volume [LVEDV]) were determined from two-dimensional imaging, and LVEF was calculated using the modified biplane method (8). After anesthesia, the right carotid artery was surgically exposed and an 8F introducer sheath with a side port was placed in the right carotid artery. Then, a LV mapping catheter (NOGASTAR®; Biosense Webster, Irwindale, CA, USA) was inserted into the left ventricle and connected to a mapping system (NOGA® XP; Biosense Webster). The mapping catheter was manipulated in every part of the left ventricle, and the catheter recognized the voltage in the myocardium and sent a signal to the mapping system. The mapping system showed an image of the mapping results which were defined by the boundary of different colors (red: infarcted myocardium, purple: healthy myocardium, and green: borderline infarcted myocardium). An intramyocardial injection catheter with a protruding needle (MyoStar®; Biosense Webster) was used for the ATSC injections. The borderline infarction zone was the site for the ATSCs injections which is represented as a green color in the mapping system. The length of the needle was adjusted to no more than 50% of the target tissue depth (5–10 mm) and the rate of injection for each 0.1 mL was 30 seconds, followed by a 5 seconds hold at the same pressure at the injection site before removing the needle (9). A total of 2 mL of ATSCs were injected, and the injection points were spaced at least 10 mm apart according to the manufacturer's guidelines.
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) for Windows, version 21.0 (IBM, Armonk, NY, USA). The data are presented as means ± standard deviation. The Mann-Whitney test was used to compare the echocardiographic data between the ATSC injection and control groups. The baseline and 4-week follow-up echocardiographic data were compared using the Wilcoxon signed-rank test. A P value < 0.05 was considered significant.
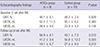
Table 1 showed a comparison of the echocardiographic data at baseline and 4 weeks after MI between the ATSCs and control groups. LVEF (46.1% ± 6.1% vs. 48.2% ± 2.4%, P = 0.829), LVEDV (52.0% ± 11.5% vs. 45.1% ± 6.2%, P = 0.360), and LVESV (28.8 ± 8.0 vs. 23.9 ± 4.2 mL, P = 0.146) were comparable between the two groups at baseline. However, LVEF was higher in the MSC group than in the control group (56.9% ± 8.1% vs. 45.1% ± 7.3%, P = 0.012) 4 weeks post-MI. There was a tendency toward a smaller LVEDV (41.2 ± 9.4 vs. 50.8 ± 12.2 mL, P = 0.055) in the ATSCs group, and LVESV was also smaller (18.1 ± 6.7 vs. 27.5 ± 8.5 mL, P = 0.012) in the ATSCs group at follow-up compared with that in the control group. On comparisons of echocardiography data between baseline and 4 weeks after MI, LVEF increased significantly (P = 0.039) in the ATSCs group, and the LVEDV (P = 0.013) and LVESV (P = 0.001) values decreased significantly from baseline to follow-up. No differences in LVEF (P = 0.228), LVEDV (P = 0.153), and LVESV (P = 0.225) were observed in the two groups. Follow-up LV mapping was performed to compare the infarct sizes between 1 and 4 weeks after MI. Visual estimation showed that infarct size decreased in cell-injected pigs (Fig. 1) on the bipolar voltage map at 4 weeks after MI: anteroposterior (1 week and 4 weeks; Fig. 1A and 1B) and right anterior oblique (1 week and 4 weeks; Fig. 1C and 1D) projections. On the other hand, infarct size was extended in the control pig on the same projections (Fig. 2).
Intramyocardial injection of ATSCs into the accurate sites followed by LV mapping improved LV systolic function, and decreased infarct size on follow-up mapping. This is the first preclinical study in Korea to investigate the efficacy of intramyocardial injection of MSCs using a novel LV mapping system (NOGA® XP) and catheter (NOGASTAR®) in an MI model. Although many preclinical and clinical studies have evaluated the efficacy of stem cell therapy in cases of MI and ischemic HF, the impact of cell therapy remained questionable and they reported only modest success with a mean increase of 2%–8% in LVEF by intracoronary route (9). The percutaneous intramyocardial route is more easily accessible and results in a better engraftment of injected cells compared to the direct injection method. However, special equipment and a catheter system are required for mapping the left ventricle prior to and during cell injections (10).
Other preclinical studies showed the efficacy of percutaneous intramyocardial injections of stem cells in terms of reduced infarct size and improved LV systolic function (111213141516). Although the present study did not evaluate clinical outcomes, LV remodeling represented as LVEDV improved and LV remodeling is the main component of ischemic HF. Therefore, its clinical usefulness is encouraging in patients with MI, although a further large-scaled clinical study is needed. To date, no previous trial to our knowledge has applied stem cell injection via intramyocardial route in Korea.
The limitations of this study include the lack of a sham group, the small sample size, and the loss of histological analyses. Further studies should be performed to investigate the action mechanisms of ATSCs.
In conclusion, we successfully established the intramyocardial injection system and stably delivered stem cells into porcine infarcted myocardium. This is the first pre-clinical trial in Korea, and ATSCs injections using LV mapping system can be useful to recover LV systolic function and to reduce LV remodeling in porcine MI.
Ethics statement
The animal experiment for this study was approved by the Institutional Animal Care and Use Committee of Chonnam National University Medical School and Chonnam National University Hospital (CNU IACUC-H-2015-38), and conformed to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85-23, revised 1996).


 XML Download
XML Download