

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The usage of antidepressants in children and adolescents has been on the increase over the last few decades, except for the temporary decrease around the time of the warning issued by the Food and Drug Administration (FDA) regarding the risk of suicidal behavior in 2004 (12), becoming almost comparable to its use in adults (3). In 2010, the Center for Disease Control and Prevention and the National Center for Health Statistics (CDC/NCHS) reported that 4.8% of adolescents take antidepressants in the US (4).
Antidepressants are FDA approved for major depressive disorder (MDD), obsessive-compulsive disorder (OCD), generalized anxiety disorder (GAD), or enuresis in children and adolescents. Four selective serotonin reuptake inhibitors (SSRIs) (escitalopram for OCD and adolescent MDD, fluoxetine for OCD and MDD, fluvoxamine and sertraline for OCD), one serotonin and norepinephrine reuptake inhibitor (SNRI) (duloxetine, for GAD), and two tricyclic antidepressants (TCAs) (clomipramine for OCD from age 10 and imipramine for enuresis) have FDA-approved indications in the pediatric population. The Korean Ministry of Food and Drug Safety (MFDS) does not endorse antidepressant prescription for pediatric depressive disorder; OCD (fluvoxamine, sertraline) and enuresis (imipramine, amitriptyline) are the only two disorders for which antidepressant prescription is approved for children and adolescents. However, several other classes of antidepressants, including SNRIs, norepinephrine reuptake inhibitors, norepinephrine dopamine reuptake inhibitors, and tetracyclic antidepressants, are now being used off-label for the treatment of depressive and anxiety disorders in children and adolescents (5), but their effectiveness and tolerability have not been sufficiently studied in this population.
Several studies have examined the prescription rates of antidepressants for children and adolescents and reported a large difference between countries, ranging from 0.11% to 0.54% in West European countries (26) and from 1.54% to 1.80% in the United States (7) and Canada (1). These studies also reported considerable off-label antidepressant usage (26), but there is only limited information on the prevalence, effectiveness, and safety of off-label antidepressant use in youths. Moreover, the prescription pattern and regulation vary among countries. Thus, concerns have been raised about the increasing use of off-label antidepressants without sufficient information (8).
Only a few studies have examined the antidepressant usage in the pediatric population in Asian countries. One study reported that 4.7% of antidepressant prescriptions were for Asian children and adolescents (9), suggesting a lower prescription rate compared to adults. However, although Chee et al.'s study (9) was based on data from multiple countries, subjects were referred from a limited number of hospitals, lowering the representativeness of the sample. Therefore, we sought to investigate the extent and pattern of antidepressant prescription for Korean children and adolescents, using population-based data from the Korean National Health Insurance Service National Sample Cohort of the year 2013.
MATERIALS AND METHODS
Data source and study population
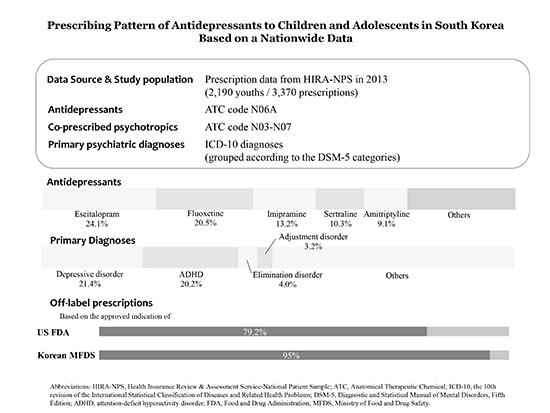
The dataset used in this study is the Health Insurance Review and Assessment Service-National Patient Sample (HIRA-NPS) of the year 2013 (serial number: HIRA-NPS-2013-0066). The HIRA-NPS was a stratified sample according to sex and an age interval of 5 years, comprising approximately 3% based on the National Health Insurance claims data (10) covering approximately 98% of the entire national population (about 50 million persons). The dataset included around 0.2 million children randomly extracted by age-gender stratification among a total of 6.7 million children and adolescents within the age range of 6–18 years. The sample extraction method has been extensively tested for representativeness and externally validated by computing the estimation of the number of patients, the frequency of top 30 diseases as well as health expenditure from it and comparing them with those from the whole insurance-covered population (11). Hence, several population-based studies have been conducted using HIRA-NPS data (1213). Our study population was defined as youths (aged 6–18 years) from the dataset who were prescribed any antidepressant medication defined below, at least once in the year of 2013.
Antidepressants and concomitant psychiatric medication
We defined antidepressants as agents included in the Anatomical Therapeutic Chemical (ATC) classification code N06A, among all available antidepressants in Korea. The medications prescribed were amitriptyline (Elavil®, Merck Sharp & Dohme, Kenilworth, NJ, USA), bupropion (Wellbutrin®; GlaxoSmithKline, Triangle Park, NC, USA), citalopram (Celexa®; Forest Laboratories LLC, St. Louis, MO, USA), clomipramine (Anafranil®; Mallinckrodt Inc., Hazelwood, MO, USA), duloxetine (Cymbalta®; Eli Lilly and Company, Indianapolis, IN, USA), escitalopram (Lexapro®; Forest Laboratories LLC), fluoxetine (Prozac®; Eli Lilly and Company), fluvoxamine (Luvox®; Jazz Pharmaceuticals, Inc., Palo Alto, CA, USA), imipramine (Tofranil®; Excellium Pharmaceutical, Inc., Fairfield, NJ, USA), milnacipran (Savella®; Forest Laboratories LLC), mirtazapine (Remeron®; Organon USA Inc., Roseland, NJ, USA), nortriptyline (Pamelor®; Mallinckrodt Inc.), paroxetine (Paxil®; GlaxoSmithKline), sertraline (Zoloft®; Pfizer Inc., New York, NY, USA), tianeptine (Stablon®, Servier, Suresnes, France), trazodone (Oleptro™; Angelini Pharma Inc., Gaithersburg, MD, USA), and venlafaxine (Effexor®; Wyeth Pharmaceuticals Inc., Philadelphia, PA, USA). Cases where more than one antidepressant was prescribed were nevertheless counted as duplicate categories, so the sum of case numbers exceeded the total cases where antidepressants were given. We also counted individuals who received more than one kind of combination separately for each combination. Antidepressant combinations and concomitant psychotropic medications were counted if they were prescribed on the same date. The distribution of the maximum number of concomitantly prescribed antidepressants was also examined.
Concomitant psychiatric medication was selected from those listed in the ATC code N03–N07. The authors comprehensively selected agents falling into the following categories: antipsychotics, medications for attention-deficit hyperactivity disorder (ADHD), benzodiazepines, and other sedatives or hypnotics.
Psychiatric diagnoses
For each case in the dataset, the primary diagnoses at the last antidepressant prescription were obtained, with the assumption that the primary diagnoses would contain the most relevant information and the final diagnosis would be relatively the most accurate. As an operational definition, the following the 10th revision of the International Statistical Classification of Diseases (ICD-10) codes were acknowledged as valid psychiatric diagnoses in our study: bipolar disorders (F30–31), depressive disorders (F32–33), cyclothymia (F34.0), dysthymia (F34.1), mood disorder not otherwise specified (NOS) (F34.8–34.9), mood disorder NOS (F38), phobic anxiety disorders (F40), panic disorder (F41.0), GAD (F41.1), mixed anxiety and depressive disorder (F41.2), anxiety disorder NOS (F41.3–F41.9), OCD (F42), acute stress disorder (F43.0), post-traumatic stress disorder (PTSD) (F43.1), adjustment disorder (F43.2), other stress reaction (F43.8–F43.9), dissociative disorders (F44), somatoform disorders (F45), depressive conduct disorder (F92.0), pervasive developmental disorders (F84), elimination disorder (F98.0–F98.1), eating disorders (F98.2, F50), ADHD (F90), organic mood disorder (F00–F09, G00–G99), and mood disorder due to substance (F10–F19). The diagnoses were grouped together such that their corresponding diagnoses in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), would belong to the same category, for an easier comparison of disparities in antidepressant prescription according to diagnoses.
Statistical analysis
The data were processed using SAS 9.3 (SAS Institute Inc., Cary, NC, USA). For the comparison between age groups, we performed chi-square test. Fisher's exact test was performed for comparison with an insufficient number of samples for χ2 test. Statistical significance was set at P < 0.05 after Bonferroni correction. Descriptive statistical analysis was performed for rest of the data.
RESULTS
A total of 2,190 youths from the HIRA-NPS-2013 sample were prescribed antidepressants at least once during the study period, bringing the annual antidepressant prescription to approximately 1.1% of the whole pediatric population. Their age and gender distribution and primary psychiatric diagnosis are described in Table 1. The most frequent diagnosis was depressive disorder (n = 469, 21.4%), followed by ADHD (n = 442, 20.2%).
Table 1
Profiles of subjects treated with antidepressants (n = 2,190)

ICD-10 = the 10th revision of the International Statistical Classification of Diseases, ADHD = attention-deficit hyperactivity disorder, NOS = not otherwise specified, PDD = pervasive developmental disorder, OCD = obsessive-compulsive disorder, PTSD = post-traumatic stress disorder, GAD = generalized anxiety disorder, SD = standard deviation.
*Values are presented as mean (SD).
![]()
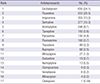
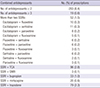
The share of each antidepressant in the total prescriptions is outlined in Table 2. Escitalopram (n = 650, 24.1%) and fluoxetine (n = 553, 20.5%), the two antidepressants approved for the treatment of depressed youths by the FDA, were ranked as the two most frequently prescribed agents, comprising roughly half of the total prescriptions. They were followed by imipramine (n = 355, 13.2%), sertraline (n = 277, 10.3%), amitriptyline (n = 246, 9.1%), and tianeptine (n = 150, 5.6%).
Table 2
Ranking of antidepressants prescribed (n = 2,697)
![]()
Table 3 provides the distribution of psychiatric diagnoses which necessitated antidepressant pharmacotherapy, according to the age group. For children aged 6–12 years, not depressive disorder but ADHD was the most prevalent diagnosis in antidepressant prescription. Depressive disorder was more prevalent in the adolescent age group (age 13–18), while elimination disorder, ADHD and tic disorders were more frequent in children (age 6–12) who were prescribed antidepressants.
Table 3
Prescription pattern for antidepressants prescribed according to age groups (n = 2,190)
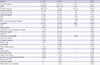
Values are presented as number (%).
ADHD = attention-deficit hyperactivity disorder, NOS = not otherwise specified, PDD = pervasive developmental disorder, OCD = obsessive-compulsive disorder, PTSD = post-traumatic stress disorder, GAD = generalized anxiety disorder.
*P < 0.05/29 (Bonferroni correction). †Fisher's exact test.
![]()
The antidepressant prescription pattern according to diagnostic groups is provided in Table 4. For youths with depressive disorders, anxiety disorders, stress and trauma-related disorders and OCD, the most prescribed antidepressant was escitalopram, while those with ADHD, intellectual disability and developmental disorders were more likely to receive fluoxetine than escitalopram. For elimination disorder, imipramine, probably due to its approved indication, was by far the most prescribed (85.6%). Compared to other antidepressants, paroxetine and trazodone were slightly more likely to be prescribed to those with stress and trauma-related disorders. According to the Korean MFDS standards, 95% of the prescriptions in our sample were off-label; applying the US FDA standards, the off-label rate remained high at 79.2%. By the Korean MFDS standards, off-label prescriptions comprised 72.3% of OCD treatment and 14.4% of enuresis treatment. For all the other diagnoses including depressive disorder, all prescriptions were off-label. By the US FDA standards, the off-label prescription rate remained 44.0% for depressive disorder and 48.7% for OCD.
Table 4
Prescription pattern for antidepressants prescribed according to diagnosis (n = 2,272)
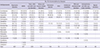
Only the ten most frequent diagnostic groups are shown.
ADHD = attention-deficit hyperactivity disorder, GAD = generalized anxiety disorder, OCD = obsessive-compulsive disorder, PDD = pervasive developmental disorder.
![]()
The frequency of antidepressant combinations is provided in Table 5. Although most youths (91.6%) were prescribed a single antidepressant, two or more antidepressants were combined in the remaining 8.4% of cases. The two most common combinations were TCA or trazodone in addition to SSRIs. The next most frequent were the combinations of two SSRIs, SSRI + bupropion, and SSRI + mirtazapine.
Table 5
Combined antidepressant treatments (n = 3,370)
SSRI = selective serotonin reuptake inhibitor, TCA = tricyclic antidepressant, SNRI = selective serotonin and norepinephrine reuptake inhibitor.
![]()
The frequency of psychopharmacological augmentation for antidepressant prescriptions is summarized in Table 6. At least one concomitant psychotropic medication was contained in 60.5% of the antidepressant prescriptions. Antipsychotics, medication for ADHD, and benzodiazepines/zolpidem were combined with 26.7%, 24.4%, and 26.3% of the antidepressant prescriptions, respectively. For the majority of youths with bipolar disorder who received antidepressants in our data (87.5%), medication with mood-stabilizing property such as lithium, valproate, lamotrigine, or antipsychotics were co-prescribed.
Table 6
Concomitant medications (n = 3,370)

![]()
DISCUSSION
Our results give a highly representative overview of the antidepressant utilization among Korean youths. The total prescription prevalence of 1.1% is much higher than that in Western European countries (0.11%–0.54%), although the rate falls slightly short of that in the US or Canada (1.54%–1.8%). The antidepressant prescription prevalence among Korean youths in our study appears rather high, in spite of the relatively low mental health literacy and general mental health care utilization in Korea (14) and the narrow indication for pediatric antidepressant prescription. This could be partly explained by a high prevalence of depressive disorder in Korean youths, compared with the international estimation of depressive disorder prevalence (15); one epidemiologic study reported a 7.4% prevalence of depressive disorder in youths (16), and 25.5% of Korean adolescents report experiencing sadness or hopelessness severe enough to impair functioning for at least two weeks during the past year, on a nationwide web-based survey (17). In addition to factors such as family conflict and low self-esteem (18), Korean youths' depression was associated with low academic achievement, higher socioeconomic status and being in the 12th grade, suggesting the role of academic pressure under a culture-specific competitive environment (19). The high prevalence of depression and the associated suicidal risk (20), combined with a lower availability of psychosocial services and community mental health care (21), could have led to the frequent prescription of antidepressants.
In the majority of cases, antidepressants were prescribed outside the currently indicated range, exceeding most rates of off-label usage of previous studies in other systems (34.4%–58.3%) (26). This could be partly explained by our use of principal diagnosis in the data, where co-morbid disorders could have been under-represented, and by the relatively stricter regulation standards of the Korean MFDS. Nevertheless, even among subjects with depressive disorders, the approved usage comprised only 56.0% by the FDA standards, and the remaining 44.0% were prescribed outside the approval range, representing a high prevalence of off-label antidepressant use. Considering the widespread off-label pediatric antidepressant usage, the impact of this practice has yet to be adequately studied. The unapproved usage might reflect the relative paucity of available therapeutic options in pediatric psychiatry, especially when the few approved medications fail (8), and in the absence of relevant data on the pediatric population, physicians treating them are likely to resort to the extrapolation of adult data (22). However, off-label prescription carries an increased risk of potential adverse effects (23). More clinical trials on children and adolescents are required, as well as regulatory measures to monitor the pharmacotherapy in pediatric psychiatry.
In our study, 1.5% of the subjects were prescribed antidepressants for bipolar disorder. The antidepressants prescription in the pediatric population could trigger antidepressant-emergent mood switch, the risk of which is increased in bipolar disorder (24). In the potential risk of antidepressant-emergent mood switch, antidepressants do not appear to carry equal risk; desipramine has been reported to carry a higher risk of mood change compared to bupropion (25) and venlafaxine has been associated with more risk than bupropion, paroxetine, or sertraline regarding mood change (2627), although no subjects in our study received venlafaxine for bipolar disorder. Although antidepressants in our data were mostly co-prescribed with mood stabilizer or antipsychotics, antidepressant therapy without mood stabilizer is more likely to induce mood switch (28). Therefore, clinicians prescribing antidepressants in pediatric bipolar disorder should cautiously monitor for mood switch, while weighing risks and benefits of using antidepressants. Further studies are needed regarding the antidepressant use in the youths with bipolar disorder.
Anxiety disorders, as well as OCD and PTSD, are not uncommon in children and adolescents (29), and they are often co-morbid with depressive disorders. While several trials support the use of SSRI's or clomipramine in pediatric OCD (30) or SSRI's and SNRI's in GAD (31), the evidence supporting antidepressant pharmacotherapy in PTSD is relatively limited (32). About a quarter of subjects in our data were prescribed antidepressants for these disorders, escitalopram being the most frequently prescribed medication, followed by other SSRIs. The widespread off-label usage of antidepressants in these conditions may indicate that currently approved diagnoses for antidepressant prescription might not adequately cover this clinical population; therefore, further studies are warranted regarding the role of antidepressant pharmacotherapy for youths with these disorders, which could provide evidence for whether to extend the range of regulatory approval.
A high proportion of our subjects who were prescribed antidepressants were diagnosed with ADHD. Studies suggest that some antidepressants, especially bupropion (33) and some tricyclics (34) could potentially ameliorate the core attention deficit and hyperactivity symptoms. Our result may have been affected by usage for this purpose. Additionally, youths with ADHD show a high co-morbidity with depressive and anxiety symptoms both above and below the threshold for diagnosing depressive or anxiety disorders (35), and antidepressants could also have been prescribed for treating these co-morbid symptoms, with the attendant risk of antidepressant-emergent mood switch (2428).
The combination of antidepressants was relatively uncommon in this study. TCA and trazodone were the most frequently combined agents, which could have been prescribed to benefit from their augmentative sedative property rather than as another antidepressant (36). The combination of two SSRIs was relatively unusual, possibly for fear of increased risk of adverse effects (37) although not much data on the safety of pediatric antidepressant combination therapy exists. More than half of children and adolescents who were prescribed received concomitant psychiatric medications other than antidepressants. While the paucity of effectiveness and safety data from adequate clinical trials regarding multiclass polypharmacy raises concerns (38), the prevalent augmentative usage with other psychotropics could also reflect the extent of the clinical burden in pediatric antidepressant pharmacotherapy.
Our study was limited in several aspects. First, our dataset was based on reimbursement data and thus not immune from issues such as up-coding (39). Therefore, precaution is needed in the appraisal of the diagnostic data. Second, the study design did not account for the variable duration of pharmacotherapy, which might be associated with the duration and possibly severity of the conditions. Third, the data used were cross-sectional only, and thus did not provide direct insight into the changing trends of prescribing antidepressants over time. Fourth, psychosocial treatments, another therapeutic mainstay in pediatric psychiatry (40), were not included in the current study, since a large proportion of those therapies are currently not covered by the national insurance and therefore not adequately represented by the current dataset. Our analysis was limited to pharmacological therapy only and did not provide an overview of pediatric psychiatric treatment in general. Fifth, our sample consisted of youths from one country. Our results need careful interpretation, considering the effect of variable regulation status as well as health care environment on the antidepressant prescription and off-label usage.
Despite of these caveats, our study has following strengths: 1) we conducted our study with population-based data with the highest representativeness; 2) we have comprehensively addressed the usage of antidepressants regarding not only diagnostic indications and off-label usage but also their combination and concomitant medication; and 3) ours is the first study to examine pediatric antidepressant usage in Korea and one of the few studies to reveal a distinctive pattern of pediatric antidepressant usage according to its cultural and administrative context.
Our study shows the prescription pattern of antidepressants for children and adolescents in Korea, of which a large proportion is off-label. The results call for caution and close monitoring by clinicians treating this population.
 XML Download
XML Download