

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Autism spectrum disorder (ASD) is a pervasive neurodevelopmental disorder, which is usually diagnosed in early childhood. While the median worldwide prevalence of autism is 0.62% (12), Kim et al. (3) have reported a prevalence as high as 2.64% for children aged 7–12 years. In Taiwan, where the National Health Insurance (NHI) system is available for all nationals, the cumulative prevalence of ASD has increased from 1.79 per 10,000 people in 1996 to 28.72 in 2005 according to a study of a population of 372,642 people (4). Compared to this rapid increase in prevalence, the development of an appropriate treatment method for the impaired communication and social interaction that are the core symptoms of ASD, and which addresses the cause of the disease, is lagging behind. At present, mainly educational and behavioral approaches are used to improve the related behavioral problems and to promote sociability (5).
Additionally, since the mechanism underlying ASD is not yet clear, various drugs are used to improve symptoms. Although the US Food and Drug Administration-approved medications for ASD are risperidone and aripiprazole, for treatment of irritability (67), psychotropic medications are prescribed to about 30%–60% of children with ASD to control aggression, irritability, and other problematic behaviors (89). Compared to the general population, children with ASD use overall nine times more psychotropic drugs, including 22 times more antipsychotics and six times more Attention-Deficit/Hyperactivity Disorder (ADHD) medications (10). In a study of 60,641 children with ASD, based on medical aid claims data, 56% of child patients were reported to have received prescriptions for one or more psychotropic medications (11). Strikingly, there have been more studies related to pharmacotherapy for ASD involving child and adolescent patients than those involving adult patients; these studies also show that the prescribed drug classes differ according to age in child and adolescent patients (12). Although psychotropic medication is often used for ASD patients, it is difficult to generalize and apply the results of previous studies, due to the limited subject groups and regions addressed in these studies.
The Ministry of Health and Welfare in Korea operates a single NHI system under the Health Insurance Law established in 1989 (13). According to the claims data from 2015, approximately 50,490,157 individuals (97.1%) had NHI, while 1,544,267 individuals (2.9%) had medical aid (1415). Claims from medical institutions nationwide are reviewed by the Health Insurance Review and Assessment Service (HIRA), and the reviewed data have been established as a database, termed the National Health Insurance Claims Database (NHICD). NHICD includes patients' diagnosis, treatments, procedures, surgical histories, and prescription drugs (16). In particular, a vast amount of NHICD information has been accumulated, as 99.9% of claims have been made via a computerized network since 2007 (17). Therefore, the NHICD offers highly representative and objective data.
Studies on diagnostic incidence and prescription trends for child and adolescent ASD patients are not only useful for clinicians, but are also fundamental to establishing treatment-related policies for children and adolescents with ASD and their families. To overcome the limitations of subjects and regions in previous studies, we here utilized the Korean NHICD to analyze the diagnostic incidence and prescription trends of autism in Korea.
MATERIALS AND METHODS
Data source and study population
We obtained data from the NHICD from January 1, 2009, to December 31, 2013, with permission for its use from HIRA. The data spanned 5 years, because this is the limit set by the HIRA for use of this data for research purposes. The subjects were those under 19 years of age, because it becomes more challenging to analyze medication use during adulthood due to increasingly more comorbid mental disorders and physical illnesses, in addition to ASD (518). Moreover, ASD-related drug studies are mostly conducted in underage groups (12), and therefore this study also selected subjects under 19 years of age to allow comparison with the results of other studies.
The subjects were those with a first diagnosis of F84, i.e., pervasive developmental disorders (PDDs), in the 10th revision of International Statistical Classification of Diseases and Related Health Problems (ICD-10) (19): F84.0, childhood autism; F84.1, atypical autism; F84.2, Rett's syndrome; F84.3, other childhood disintegrative disorder; F84.4, overactive disorder associated with mental retardation and stereotyped movements; F84.5, Asperger's syndrome; F84.8, other PDDs; and F84.9, PDD, unspecified. Those whose first diagnosis involved other psychiatric diagnoses or physical disorders were excluded. Since the Korean NHICD followed the ICD-10 standard, this standard was applied. To calculate the diagnostic incidence, we selected patients who had at least one medical claim containing F84 and who had not been diagnosed in the previous 360 days. Of the data for 2009–2013, the data for 2013 were excluded because the insurance data had not been completed in the database by early 2014 when this study was begun. Therefore, the final data used for analysis were the NHICD data for the 3 years from January 2010 to December 2012.
The populations younger than 19 years of age amounted to 10,882,052 people in 2010, 10,631,826 in 2011, and 10,405,854 in 2012, as of December in each year (20). Even though the subjects of this study were patients with PDD, which is different from ASD in the Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5) (21), we have described them as patients with ASD for convenience.
Methods
The annual incidence of ASD from 2010 to 2012 was calculated by dividing the number of newly diagnosed cases of ASD during the 3-year period by the number of general population for the same period. We analyzed the data of patients with ASD depending on sex, age, type of medical insurance (NHI or medical aid), and type of medical institution visited (general hospital, mental hospital, private clinic, and others). For comparison by age group, the population of 0–18 years old was subdivided into 3-year age groups following the HIRA sample data analysis reported by Hwangbo et al. (22). The prevalence of pharmacotherapy use was calculated using the same method as diagnostic incidence. We counted patients who had received at least one prescription of psychotropics, but had not taken any psychotropics in the previous 360 days. Medications were classified into seven categories: antipsychotics (typical and atypical); ADHD drugs (stimulants and non-stimulants); antidepressants (selective serotonin reuptake inhibitors [SSRIs] and tricyclic antidepressants [TCA]); anxiolytics (benzodiazepines); mood stabilizers; opioid antagonists (naltrexone only); and miscellaneous.
RESULTS
During 2010–2012, the annual number of newly ASD-diagnosed patients aged 0–18 years were 5,596, 6,163, and 5,847, for the three consecutive years. The mean annual diagnostic incidence in this age group during 2010−2012 was 5.52 per 10,000 population. Males accounted for 77.0% (Table 1). The highest number of patients diagnosed with ASD fell in the 0–3 and 4–6 years age groups. When compared by insurance type, the NHI group accounted for 93.8%. For diagnosis by medical institution, the highest proportion was diagnosed in private clinics, followed by general hospitals, mental hospitals, and others, in order.
Table 1
Cumulative incidence of ASD diagnosis and characteristics of patients with ASD for the period 2010–2012
Values are presented as number (%).
ASD = autism spectrum disorder, NHI = National Health Insurance, Medicaid = medical aid.
![]()
The mean prescription prevalence for the 3 years was 30.4% (Table 2). When compared by sex, males showed a higher prescription rate than females (χ2 = 110.86; P < 0.001). The prescription rate increased with the patients' age (χ2 = 3,551.68; P < 0.001). In analysis by insurance type, patients with medical aid had a higher prescription rate than those with NHI (χ2 = 129.77; P < 0.001). When compared by type of institution, the prescription rate was higher in private clinics than in general hospitals or mental hospitals (χ2 = 181.15; P < 0.001).
Table 2
Comparison of cumulative medication rates (%) among different population groups for the period 2010–2012
Med = patients prescribed with one or more psychotropics, Non-med = drug naïve cases, NHI = National Health Insurance, Medicaid = medical aid.
*P < 0.001.
![]()
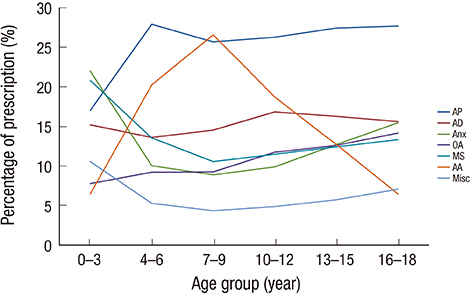
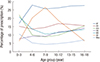
An analysis of the pattern of prescriptions revealed no differences across the 3 years (χ2 = 21.92; P = 0.08). Atypical antipsychotics were used most frequently, followed by antidepressants, ADHD drugs, mood stabilizers, anxiolytics, and opioid antagonists, in order (Table 3). The mean numbers of drugs prescribed per person were 2.54. When analyzed using sex as a variable, there was a significant difference in terms of drug types (χ2 = 97.92; P < 0.001; Table 4). Males had a higher prescription rate of antipsychotics and ADHD drugs than females. In females, antidepressants, anxiolytics, and mood stabilizers were more often prescribed than in males. When analyzed by age, there was also a significantly different pattern of drug prescriptions (χ2 = 818.12; P < 0.001) (Fig. 1). Patients aged 0–3 years old had a higher prescription rate of anxiolytics, whereas the prescription rate of ADHD drugs tended to increase from 4 years of age, reaching a peak at 7–9 years of age. The prescription rate of antipsychotics increased from 4 years of age and was highest after the age of 10 years.
Table 3
Patterns of psychotropic medications for the period 2010–2012
AP = antipsychotics, AD = antidepressants, AA = anti-Attention-Deficit/Hyperactivity Disorder (ADHD) drugs, MS = mood stabilizers, Anx = anxiolytics, OA = opioid antagonists, Misc = miscellaneous.
![]()
Table 4
Comparison of prescription patterns by sex for the period 2010–2012

AP = antipsychotics, AD = antidepressants, AA = anti-Attention-Deficit/Hyperactivity Disorder (ADHD) drugs, MS = mood stabilizers, Anx = anxiolytics, OA = opioid antagonists, Misc = miscellaneous.
*P < 0.001.
![]()
DISCUSSION
The mean annual incidence of ASD diagnosis in this study was 5.52 per 10,000 people, which was higher than that of Taiwan (4.41 people) (4). In Taiwan, which has a similar NHI system to that of Korea, the incidence tended to increase from 0.91/10,000 in 1997 to 4.41/10,000 in 2005 (4). Since no comparative data were available for Korea, and as the present study period (3 years) was short, it would be necessary to compare at least 10 years of data to comprehend the trend of the annual incidence, as has been done in Taiwan (4). The reason for the increase in ASD diagnosis is likely that ASD has broader diagnostic criteria than previously used for the diagnosis of traditional infantile autism, that experts and parents have become more aware of the disease, and that many child specialist services have developed over the past number of years (4).
The diagnostic incidence was the highest in the age range from 0 to 3 years. Preceding studies have shown similar results. In an analysis of the Autism and Developmental Disabilities Monitoring (ADDM) Network data, 43% of children with ASD received comprehensive evaluation before the age of 3 years (23). In a Taiwanese study of subjects younger than 18 years of age, the group aged 0–5 years showed the highest incidence (4). In the report by Williams et al. (24) of a study of children aged 14 years or younger, the diagnosis rate was higher in those before school age (3–4 years of age), and the incidence of new diagnoses tended to decrease with age. It was therefore speculated that, while the absolute number was the highest in the group aged 0–6 years, the incidence in the older age group increased as the cumulative incidence increased annually. Interestingly, the incidence rate was higher in general hospitals and private clinics, whereas the drug prescription rate was highest in private clinics. It seems that general hospitals were preferred for diagnosis, due to the Korean healthcare system, whereas private clinics were favored for prescription, because drugs were not used temporarily (25).
Patients who used psychotropics for the first time accounted for 30.4% of the diagnosed group on average, which was lower than that of the overall drug administration rate, 63.6%, reported by Spencer et al. (26) for subjects with ASD who were 20 years or younger. In studies that analyzed medical aid claims data (2728), the drug prescription rate was 60% or higher. The prescription rate of psychotropic medications may have been higher in the population covered by medical aid than in the general populations, as medical aid had neither formulary restrictions nor copayment policies, as compared to private insurance (29). On the other hand, Rosenberg et al. (9) reported a drug use rate for children with autism as low as 35%, which was speculated to be due to a low participation rate (20%) in the medical aid group. Considering that drug prescription rates differ according to insurance type, and since this study analyzed the total population, regardless of insurance type, it suggests that the results of this study should be representative of prescription trends of psychotropics for ASD overall.
The drug type most frequently prescribed was antipsychotics, followed by antidepressants and stimulants, in order. Although pimozide is the only drug approved for ASD in Japan, atypical antipsychotics, including risperidone, were used most frequently, followed by other antipsychotics, stimulants, all other central nervous system drugs, anticonvulsants, and nonbarbiturates, in that order (30). These findings were similar to the results of previous studies conducted based on medical aid claims data (1128). In previous studies, antidepressants were prescribed more often than antipsychotic agents, depending on the study (831). Antidepressant prescriptions are used not only for treatment of depressive symptoms, but also for reduction of perseverative, stereotypic, and aggressive behaviors. In some studies, stimulants were used more often than antipsychotic agents (932).
Sex is an important factor determining the drug administration rate and drug types used for patients (11). The present study found that males were significantly more often diagnosed and were more often prescribed drugs than were females. Although some studies reported no relationship between sex and the prevalence of psychotropic use (333435), it has been reported that the ASD diagnostic rate (5) and the frequency of psychotropic medication (36) are both higher in males than in females. The type of drug used also differed depending on sex. In this study, males had higher prescription rates of antipsychotics and ADHD drugs than females, and antidepressants, anxiolytics and mood stabilizers were more often prescribed in females than in males. Similarly, previous studies also showed a higher rate of prescriptions of antipsychotics and ADHD drugs for males and antidepressants and anxiolytics for females (1231). It has been speculated that these characteristics may be related to the age-related increase in the externalizing disorders in males and its internalizing disorders in females, as reported by Hwangbo et al. (22), based on analysis of the Korean NHICD data.
The drug prescription rate tended to increase with age in this study as well as in several previous studies with large samples of ASD-affected individuals (928). In the comparison of ASD groups aged 8 and 15 years, the 15-year-old group had higher prescription rates of antipsychotics, antidepressants, mood stabilizers, and anxiolytics than did the 8-year-old group (32). In terms of the overall increase in drug prescription with age, a preceding study had claimed that it was either because healthcare providers hesitated to prescribe psychotropic medication to younger children, or because behavioral problems requiring drug prescription appeared later on in life (3137). This was compatible with the report by Mire et al. (38), which stated that the increased use of ADHD drugs and antipsychotics in individuals with ASD aged 7–9 years is probably due to these individuals being of school-going age. Moreover, the present study found differences in the prescribed drug types depending on age. While the group aged 3 years or younger was prescribed more anxiolytics, the groups aged 4–6 and 7–9 years were prescribed more ADHD drugs and antipsychotics prescriptions of antipsychotics and antidepressants were much higher in the older age group. Drug prescriptions in children are also affected by age-related changes in the presenting symptoms; for instance, hyperactivity and irritability are known to decrease, while comorbid mood and anxiety problems increase, as children with ASD get older (38). In a study of child and adolescent patients younger than 21 years, the most frequently prescribed drugs were sedatives for the group aged 0–2 years, neuroleptic drugs and stimulants for the group aged 3–11 years, and neuroleptic drugs for the remaining age group (11). In another study, involving patients younger than 21 years of age, the use of antidepressants, antipsychotics, and anticonvulsants tended to increase with age, whereas prescription of stimulant medication increased with age in the younger population, but decreased for those aged 14 years and older (8).
Interestingly, naltrexone, an opioid antagonist, was used markedly often in this study. Since one randomized control trial on naltrexone reported a trend for improvement of self-injurious behavior (39), the results have not been replicated by an independent research group to date (40). In general, the frequency of medication with naltrexone was very low and was not included as a distinct category (9). Thus, this needs to be revisited in a future NHICD analysis.
The average number of medications per person was 2.54. It has been reported that comorbid psychiatric disorders in ASD reach up to 70%, and that comorbid disease caused a high drug prescription rate in children with ASD (511). In a study of 60,641 Medicaid-enrolled children (11), 56% of cases had a prescription of at least one psychotropic medication. Jobski et al. (12) analyzed data from studies on the use of psychotropic drugs in patients with ASD, in which 24 out of 47 studies used two or more drugs concomitantly. In a future study, comorbid disease data should be analyzed along with the cause for polypharmacy.
The limitations of this study are as follows. First, it is difficult to confirm the age at the first diagnosis of ASD, because the Korean HIRA permits only analysis of 5-year data sets, for administrative reasons. Second, also due to administrative reasons related to the NHICD, we did not have clinical information on symptom severity, or sociodemographic information, such as parental income and educational level. Third, even though various therapeutic interventions can be used to treat and educate patients with ASD, the HIRA does not cover the majority of non-pharmacological methods, such as play therapy, applied behavior analysis, music therapy, language therapy, etc. Therefore, the analysis in this study was unavoidably limited to drug treatment. In addition, advanced medicines, such as oxytocin or memantine, were not officially registered in the HIRA and it was not possible to calculate the prescription for them.
This study has the following strengths. While most preceding studies used parent-reported medication data or a medical aid claims database, this study was conducted on the total population under 19 years of age, so that the results are representative and generalizable.
In conclusion, based on the analysis of the diagnostic incidence and drug treatment prevalence in the total population under 19 years of age, approximately 30% of patients diagnosed with ASD were using psychotropic agents. Although antipsychotic drugs and antidepressants were used most frequently, the type of drugs prescribed differed depending on sex, suggesting that behavioral issues also differ with sex. Medications increased with age, particularly from school age. The medical aid group had a significantly higher medication use frequency than the NHI group. As demonstrated by these results, drug types or medication patterns differed depending on sex, age, health insurance type, and medical institution type. Since the mechanism underlying ASD is not yet elucidated, cause-related drug treatments are not yet available; instead, only symptomatic drug treatment is currently available. Thus, risk-benefit profiles should urgently be established, considering the uncertain benefits of current medications.
 XML Download
XML Download