

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
More than half of all sexual assault victims report experiencing sexual victimization more than once (1). In a recent Korean national survey, 52.2% of victims of sexual violence reported having been victimized more than once (2). These revictimized women experience more emotional distress and psychopathology, including post-traumatic stress disorder (PTSD) (3) and suicide attempts (4) than sexual assault victims who are singly victimized. Furthermore, revictimized women were at higher risk of engaging in prostitution and were less likely to use condoms consistently than women who had been sexually abused only as a child or an adult (5), resulting in higher social cost. Several studies have focused on the risk factors of revictimization, such as childhood abuse (6), risk recognition (7), and sexual assertiveness (8). PTSD symptoms (9) and depression and anxiety (10) have also been proposed as risk factors for rape and revictimization.
Post-traumatic negative cognition affects post-traumatic stress symptoms and prognosis in traumatized victims (11). Thoughts about one's perceived weaknesses and the dangers of the world play an important role in the development of PTSD (12). Several trauma theorists have proposed that negative thoughts about the world and one's incompetence mediate the development of PTSD after sexual assault (1314). In other studies, avoidance-coping embedded dysfunctional cognitions (e.g., “the world is dangerous,” “the accident was my fault”) are associated with greater levels of post-traumatic stress symptoms (1516). However, how post-traumatic cognition contributes to the link between a history of sexual abuse and post-traumatic stress symptoms in sexual assault victims in Korea remains unclear.
Given that women with a history of sexual abuse show higher post-traumatic symptoms than women without a history of sexual abuse, it is important to determine which factors lead to a poor prognosis to develop intervention strategies that reduce symptoms in sexually revictimized women. Negative post-traumatic cognition is widely recognized as being important in the exploration of the relationship between negative cognition and post-traumatic stress symptoms. The aim of this paper was to determine the role post-traumatic cognition plays in the relationship between a history of sexual abuse and post-traumatic stress symptoms in sexual assault victims in Korea. We hypothesized that revictimized women would show more severe post-traumatic stress symptoms than singly victimized women, and that these symptoms would be mediated by post-traumatic negative cognition. The study was conducted using data from a Sunflower Center, a crisis intervention center for sexual assault victims, in Korea.
MATERIALS AND METHODS
Participants and procedure
Data were obtained from victim records at the Sunflower Center of Southern Gyeonggi for Women and Children Victims of Violence and Ajou University Hospital in Korea. The Sunflower Center is a government-funded, hospital-based, crisis intervention service center that provides counseling, legal and investigative support, and medical and psychological treatment for victims of sexual violence, domestic violence, and sex trafficking in Korea. For this study, we retrospectively evaluated the records of victims who visited the center between December 2014 and June 2016, and excluded victims of domestic violence or sex trafficking, male victims, victims with intellectual disabilities and those without Korean nationality, as well as victims whose crime report was considered unreliable.
Demographic characteristics and the features of the assault were obtained from data recorded at the initial baseline assessment. At this baseline assessment, victims completed self-report questionnaires to evaluate post-traumatic cognition and the severity of post-traumatic stress symptoms, anxiety, and depression. One month after the initial assessment, victims were contacted by telephone and re-completed the self-report questionnaire to evaluate the severity of post-traumatic stress symptoms.
Measures
At the initial assessment, victims completed the Post-traumatic Cognitions Inventory (PTCI) to evaluate negative trauma-related thoughts and beliefs. The PTCI consists of 36 items, which are divided into three subscales: negative cognitions about self (21 items; negative self), negative cognitions about the world (7 items; negative world), and self-blame for trauma (5 items; self-blame). Each item is scored on a seven-point Likert scale. The PTCI subscales have good test-retest reliability (0.75–0.89), good internal consistency (Cronbach's α, 0.86–0.97), and moderate-to-high correlations with post-traumatic stress symptom severity (17). The PTCI items were translated into Korean by the first author, and then reviewed by a fluent bilingual psychiatrist. Cronbach's α in the present study was 0.95.
At the initial assessment and 1 month later, victims completed the PTSD Symptoms Scale: Self-Report Version (PSS-SR) to evaluate the severity of post-traumatic stress symptoms. The PSS-SR consists of 17 items that correspond to the PTSD symptoms listed in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV). The PSS-SR has an acceptable-to-good reliability and validity, and provides a measure of symptom severity (18). The PSS-SR used in this study was composed of items derived from the PTSD diagnostic criteria in the Korean version of the Structured Clinical Interview for the DSM-IV (19).
At the initial assessment, victims completed the Korean version of the Beck Depression Inventory (BDI) (20) and Beck Anxiety Inventory (BAI) (21) to evaluate depression and anxiety, respectively. The BDI is a 21-item self-report scale that evaluates the severity of depressive symptoms. The Korean version of the BDI has good psychometric properties, with internal consistency of 0.92 (22). The BAI is a 21-item self-report questionnaire designed to evaluate the frequency of anxiety symptoms over a 1-week period. We administered a Korean version of the BAI that demonstrates good psychometric properties. The internal consistency coefficient of the BAI is 0.93, and test-retest reliability is 0.84 (23).
Data analysis
All statistical analyses were conducted using SAS, version 9.4 (SAS Institute Inc., Cary, NC, USA). Women who reported having experienced prior sexual abuse were classified as sexually revictimized. Women who reported no prior sexual abuse were classified as singly victimized. Chi-square and Fisher's exact tests were used to compare the distribution of categorical variables between groups. Independent samples t-test was used to compare PSS-SR scores, PTCI scores, BDI score, and BAI score between revictimized and singly victimized women. The paired t-test was performed to compare the PSS-SR score at initial assessment and at 1 month follow-up.
To test whether post-traumatic negative cognition mediated the relation between a history of sexual abuse and severity of post-traumatic stress symptoms, we first tested the bivariate correlation between a history of sexual abuse (coded as 0 for no, 1 for yes) and PTCI scores (total score, negative self-subscale score, negative world subscale score, and self-blame subscale score) at initial assessment and PSS-SR scores (total score, re-experiencing subscale score, avoidance subscale score, and hyperarousal subscale score) at 1 month follow-up. We conducted regression analysis with and without adjusting for PTCI scores to test the direct and indirect pathways connecting a history of sexual abuse with the severity of post-traumatic stress symptoms. All regression analyses were adjusted for age, marital status, and type of violence.
RESULTS
A total of 646 people reporting sexual victimization visited the Center between December 2014 and December 2015. One hundred and forty-six of these were excluded (8 men and 82 women with intellectual disabilities, 9 women with foreign nationalities, and 13 women with unreliable crime reports). The remaining 157 (31.4%) of the 500 women had completed the psychological measures (PTCI, PSS-SR, BDI, and BAI) at the initial assessment. Those who did not complete the questionnaires were either victims too agitated or too drunk to fill in the questionnaires, victims with limited ability to understand the Korean language, and those who refused to answer the questionnaires. Fifty-two of these women were lost to follow-up, and 105 (66.9%) participated in a telephone survey at 1 month after the initial assessment. These 80 women were included in the analysis. Victims who did not complete the baseline psychological assessment (n = 239) were more likely to be aged over 30 years, assaulted rather than raped, and not drunk at the time of the crime than victims who did complete the baseline psychological assessment (n = 121; data not shown, available on request). The type of perpetuator differed between victims who were lost to follow-up (n = 41) and victims who were not lost to follow-up (n = 80; data not shown, available on request). However, victims included in and excluded from the analysis did not differ in the main exposure variable, whether or not they reported being exposed to prior sexual abuse.
Among the 105 female victims included in the analysis, 83 (79.1%) reported having been raped, and 63 (60.0%) visited the center within 24 hours of the crime. 10 (9.5%) reported that they had been sexually victimized before, and were classified as revictimized. The remaining 95 women were classified as singly victimized. Revictimized women showed a trend of being more likely to have had a photograph taken during the assault (Table 1).
Table 1
Characteristics of the participants

![]()
The PSS-SR score at initial assessment did not differ between revictimized and singly victimized women. The PTCI and BDI scores at initial assessment and PSS-SR score at 1 month follow-up were significantly higher for revictimized women than for singly victimized women. There was a statistically significant difference (mean [standard deviation], 4.0 [8.69] vs. −3.3 [9.22]; P value = 0.020) (Table 2) in the differences in PSS-SR scores at 1 month follow-up and at initial assessment between victims with and without a history of sexual abuse. PSS-SR scores were significantly decreased for singly victimized women (P value = 0.001), whereas they were increased for revictimized women (P value = 0.180) (Fig. 1).
Table 2
Severity of PTSD symptoms and post-traumatic negative cognition at initial assessment and 1 month follow-up in sexually assaulted women with and without a history of sexual abuse

Data are presented as mean (standard deviation).
PTSD = post-traumatic stress disorder, PSS-SR = Post-traumatic Stress Disorder Symptoms Scale: Self-Report Version, PTCI = Post-traumatic Cognitions Inventory, BDI = Beck Depression Inventory, BAI = Beck Anxiety Inventory.
![]()
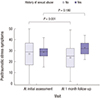 | Fig. 1Boxplot of PSS-SR scores of victims with and without a history of sexual abuse at initial assessment and at 1 month follow-up.
PSS-SR = Post-traumatic Stress Disorder Symptoms Scale: Self-Report Version.
|
The association between a history of sexual abuse and PSS-SR score was attenuated after adjusting for PTCI score (Fig. 2).
 | Fig. 2Direct and indirect pathways connecting a history of sexual abuse with the severity of post-traumatic stress symptoms. Data on history of sexual abuse was coded as 1: yes, 0: no. The severity of post-traumatic stress symptoms was evaluated at 1 month follow-up using the PSS-SR. Post-traumatic negative cognition was evaluated at initial assessment using the PTCI.
PSS-SR = Post-traumatic Stress Disorder Symptoms Scale: Self-Report Version, PTCI = Post-traumatic Cognitions Inventory.
|
DISCUSSION
Only 9.5% of the victims were classified as sexually revictimized. At initial assessment, revictimized women had a higher PTCI total score than singly victimized women, indicating greater post-traumatic negative cognition. The change in symptom severity during the first month after the visit was significantly different between revictimized and singly victimized women. Although not statistically significant, probably because of the small sample size (10), the PSS-SR score of revictimized women at 1 month follow-up had increased, indicating an increase in the severity of post-traumatic stress symptoms, whereas that of singly victimized women had decreased. Post-traumatic negative cognition fully mediated the association between a history of sexual abuse and the severity of post-traumatic stress symptoms.
Several limitations should be taken into account when interpreting these results. First, only one-third of the women who were eligible to be included in the analysis had completed the psychological questionnaires at the initial assessment. However, those included in and excluded from the analysis did not differ in the main exposure variable, i.e., whether or not they had been exposed to prior sexual abuse, and we believe that the low inclusion rate would not have had a major impact on the results. Also, while a larger sample size would have been more ideal, current analysis nonetheless yielded statistical significance. Second, only about 9% of the women included in the study reported prior sexual abuse. This is a much smaller proportion than in extant studies (23). This difference may be due to a number of factors. The Sunflower Center is an emergency support center, and acute victims may be more likely to seek such support than chronically victimized women who have experienced multiple attacks. It is also possible that some women did not report their abuse history, possibly due to shame or fear of being blamed, or to avoid being disadvantaged in the investigative or legal process. However, this potential misclassification bias towards the null and reduces the power of the study, making our results more conservative. Third, although a thorough evaluation of past life events and trauma history, including childhood abuse and physical victimization, would have yielded a more fruitful analysis and allowed us to compare the effect of sexual violence on post-traumatic stress symptoms with that of other types of traumas, this was beyond the scope of the current study. In addition, a structured interview would have provided more objective information on the psychiatric status and psychological functioning of the victims than the self-report questionnaires used. However, the data collected reflect an acute stage of trauma.
Despite these limitations, our analyses exhibit several strengths that warrant attention. First, psychological status was assessed at the acute stage after the sexual assault. The majority of the women included in the analysis underwent the initial evaluation within 3 months of experiencing the sexual assault, and about two-thirds underwent the evaluation within 24 hours. Second, although the follow-up was short in duration, longitudinal data were acquired through the 1 month telephone follow-up survey, and allowed us to understand the short-term trajectory of post-traumatic stress symptoms in sexual assault victims.
Acute post-traumatic stress symptoms gradually improve with time (24); however, revictimized women had a higher PSS-SR score, indicating more severe symptoms, at 1 month follow-up than at the initial assessment. There may be several explanations for this. First, revictimized victims may have experienced additional traumatic events in the 1 month-interval between initial assessment and follow-up. Revictimized victims may exhibit a number of risk factors, including maladaptive coping strategies or risk recognition ability, that make them prone to additional traumatic events, such as post crime victimization, i.e., victim blaming or inappropriate post-assault behavior by medical or investigative personnel. Maladaptive coping strategy is one of the risk factors for sexual revictimization (25). Individuals who reported both childhood and adulthood sexual assault had more post-traumatic stress symptoms and were more likely to use drugs or alcohol to cope, act out sexually, withdraw from people, and seek therapy services than individuals who reported only adulthood sexual assault without childhood sexual assault (25). Risk recognition ability has also been associated with interpersonal revictimization (726). Second, dissociation in the acute stages after the assault may have been more prevalent in revictimized women than in singly victimized women, and post-traumatic stress symptoms may have therefore worsened in these women as dissociation dissipated with time (7).
Previous researches have shown that maladaptive beliefs related to the trauma play an important role in the development and maintenance of PSTD symptoms and are predictive of higher PTSD symptom severity (111617). In our study, revictimized women similarly had more maladaptive cognitions regarding their trauma than singly victimized women. Especially, revictimized women showed higher scores in the Self (negative cognitions about the self) and Blame (self-blame for trauma) subscales of the PTCI than singly victimized women. Previous studies indicated that Asian cultures endorse more rapist-supportive attitudes such as women are responsible for preventing rape and victims cause rape (2728). A recent study also suggested that Asian American college women showed more maladaptive beliefs about the sexual assault than White American college women (29). Our results suggest that revictimized women showed more negative cognitions about the self than singly victimized women, which in turn was associated with higher PTSD symptom severity. Compared with previous study which emphasized the role of cognitive appraisals concerning the dangerousness of the world in maintaining the PTSD symptoms in Korean victims of sexual trauma (16), revictimized women are endorsing negative attitudes about themselves as a result of the repeated trauma.
These findings suggest that revictimized women are a distinct group, with different psychological profiles and 1 month symptom trajectories to those of singly victimized women. As Cloitre (30) argued, the response to a victim of sexual assault should be based on that victim's characteristics. We believe that evidence-based protocols are required to enable revictimized women to be identified and enable tailored support and services to be provided to these women. Personnel working with this population should be aware of the characteristics and respond accordingly.
When providing services for victims of sexual violence, treatment of post-traumatic symptoms may not be enough. Revictimized women may benefit from interventions focused on post-traumatic negative cognition, such as trauma focused cognitive behavioral therapy (3132). Interventions targeted at preventing revictimization should also be included, because revictimized women report more severe symptoms. Social learning or feminist intervention and risk detection or executive function interventions significantly reduced the risk of sexual revictimization, and should be considered as part of the service provided for victims of sexual violence (33). A mindfulness-based program aimed at reducing sexual revictimization also had a large effect; women with a history of child sexual abuse who participated in such a program were less likely to be sexually assaulted and raped at 2-month follow-up (34). In addition, problematic alcohol drinking has been proposed as a predictor of sexual revictimization (3536). In a sexual assault risk reduction intervention study, a program that targeted both sexual assault and alcohol use was the most effective way of reducing the risk of sexual assault (37).
Early detection of sexually revictimized women and tailored service and treatment intervention is needed to serve better this group of victims. Interventions targeted at preventing revictimization or post crime victimization may also help victims recover from the trauma and prevent future abuse.
 XML Download
XML Download