

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Scrotal trauma is an uncommon type of urogenital trauma, and its treatment can reduce possible complications including chronic pain, infertility, hypogonadism, and impaired self-esteem (1). The acutely traumatized scrotum is observed as a painful and markedly swollen scrotum, making clinical examination difficult. Ultrasonography provides a simple and rapidly available method to evaluate the anatomic and physiologic integrity of scrotal contents, and aids in distinguishing among pathologic entities (2). Although recent studies have shown high sensitivity of ultrasonography for the diagnosis of testis rupture, the reliability of ultrasonography remains controversial. For instance, any alteration of the normal testicular echogenicity is a useful diagnostic criterion, but this feature alone cannot guarantee the presence of testicular rupture or indicate the need for exploratory surgery. The use of alteration in testicular echogenicity alone increases the number of false-positive cases, because intratesticular heterogeneous echogenicity is also caused by hemorrhage or infarction (3). In this study, we investigated patients who were treated for scrotal trauma at our institute for the last 3 decades to describe our experience, with an emphasis on etiologies and ultrasonographic findings in these patients.
MATERIALS AND METHODS
Patients who were treated at our institute with scrotal trauma between 1986 and 2015 were included in this study. We evaluated clinical, ultrasonographic, and intraoperative findings for all patients.
The etiologies of blunt testicular injury were classified as follows: assault, fall down, sports, and traffic accident. Testis rupture was defined as laceration of the tunica albuginea or testicular destruction identified during surgical exploration.
Ultrasonography was performed by the radiologist on call. Results were reviewed by a urologist before surgical exploration. The ultrasonographic findings for testis injury were as follows: echo pattern of testicular parenchyma (homogenous vs. heterogeneous), contour definition of testicular parenchyma (intact contour vs. loss of contour), and pattern of hematoma (extra-testicular vs. intra-testicular vs. intra- and extra-testicular). Intra-testicular hematoma was defined as a focal area of altered echogenicity within the testis with no internal flow on color Doppler and preservation of the ovoid shape in multiple planes, while extra-testicular hematoma was defined as extra-testicular collection within the tunica vaginalis with low-level echoes (456).
Surgical exploration was then performed on an emergent basis after analgesia administration and anesthesia preparation. Surgery usually consisted of unilateral transverse scrotal or median longitudinal access, allowing for exploration of the contralateral testis. Salvage management with debridement of necrotic testicular tissue and closure of the tunica albuginea was performed each time. Orchiectomy was performed only in informed patients when salvage therapy was not possible. Depending on the surgical findings, the severity of injury was graded using a scaling system for organ specific injuries (7). According to this scaling system, testicular injury was graded as follows; grade I as contusion or hematoma, grade II as subclinical laceration of tunica albuginea, grade III as laceration of tunica albuginea with < 50% parenchymal loss, grade IV as major laceration of tunica albuginea with ≥ 50% parenchymal loss, and grade V as total testicular destruction or avulsion. All patients were evaluated in the outpatient clinic within one month after surgery. Further follow-up visits depended on the presence of complications.
Spearman correlation coefficient (rho) was calculated for assessing the correlation between ultrasonographic and surgical findings. Correlation of ultrasonographic findings including echo pattern of the testicular parenchyma, contour definition of the testicular parenchyma, and pattern of hematoma with surgical findings including contusion/hematoma, laceration of tunica albuginea, and testicular destruction/avulsion were analyzed. Regarding the strength of correlations, coefficients < 0.3 were considered weak, 0.3–0.5 were moderate, and > 0.5 were strong. All statistical analyses were performed using SPSS software (version 18.0; SPSS Inc., Chicago, IL, USA) with a P value < 0.05 defined as statistically significant.
RESULTS
The median age of the patients was 28.0 years (interquartile range [IQR], 15–37 years). The median time between the urologic consultation and the initial trauma was 2.0 hours (IQR, 0.8–8.0 hours).
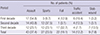
The etiology of blunt testicular injury was assault in 43 (37.4%) patients, sport in 27 (23.5%) patients, fall in 22 (19.1%) patients, and traffic accident in 14 (12.2%) patients. Nine (7.8%) patients were managed for penetrating testicular injury due to stab wound. An assault was the most common etiology of injury during the first decade. However, it decreased gradually from 54.8% during the first decade to 23.1% during the third decade. The proportion of injuries due to sports and fall during the third decade (23.1% and 32.7%, respectively) was higher than that of the first decade (9.7% and 12.9%, respectively) (Table 1). The severity of testicular injury decreased over 30 years (Fig. 1). Over the first and second decades, testicular injuries graded higher than 3 accounted for more than 70% of injuries. However, within the most recent decade, more than 70% patients presented with grade 1 testicular injury.
Table 1
Etiology of testicular injury stratified by decade
![]()

Of the 106 patients with blunt testicular injury, 80 (75.5%) patients underwent ultrasonography. Among these 80 patients, a heterogeneous echo pattern of the testicular parenchyma was observed in 44 (55%) patients. Loss of contour definition of the testicular parenchyma was observed in 41 (51.3%) patients. Regarding the pattern of hematoma, most patients showed intra-testicular hematoma (27 [33.8%]), followed by intra- and extra-testicular hematoma (26 [32.5%]) and extra-testicular hematoma (3 [3.8%]) (Table 2).
Table 2
Ultrasonographic and surgical findings of patients

![]()
Among the 26 patients who did not undergo ultrasonography, 10 patients were treated with conservative management for minimal injury based on clinical examination. The remaining 16 patients were treated with urgent surgical management based on clinical examination including physical examination and computed tomography.
Of the 9 patients with penetrating testicular injury, 3 (33.3%) patients underwent ultrasonography. The remaining 6 patients were treated with urgent surgical management because of an open wound with testicular exposure.
Among the total of 83 patients who underwent ultrasonography, 56 (67.5%) patients were treated with surgical management. Most patients with a heterogeneous echo pattern of the testis (70.5%) and loss of contour definition (81.9%) on preoperative ultrasonography were found to have laceration of the tunica albuginea or testicular destruction during surgery. Approximately, 85% of patients with intra- and extra-testicular hematoma showed laceration of the tunica albuginea or testicular destruction during surgery. The correlation between preoperative ultrasonographic and surgical findings showed a moderate to strong degree of correlation. Contour definition of the testicular parenchyma strongly correlated with surgical findings, demonstrating a Spearman correlation co-efficient of 0.758. Using the findings of heterogeneous testicular parenchyma, loss of contour definition, intra-testicular hematoma, and intra- and extra-testicular hematoma, the ultrasonographic sensitivity and specificity for the diagnosis of testicular rupture were 76.7% and 100%, respectively. For instance, patients with homogenous echo, normal contour definition, and extra-testicular hematoma in pre-operative ultrasonography, testicular rupture was not observed at surgery.
DISCUSSION
The testes are protected by their own mobility and by their anatomical position between the thighs. Further protection is provided by the tunica albuginea and the cremaster reflex (8). Therefore, testicular injuries are not common among injuries of the genitourinary tract (9). According to previous reports, most testicular injuries are caused by blunt trauma (1011). The Societe Internationale d'Urologie (SIU) consensus group on genitourinary trauma stated that most blunt trauma occurs during athletic activity (12). However, a study from Korea in 2008 reported that assault is the most common cause of testicular injury (13). Similar to the previous Korean study, our experience showed that assault was the most common etiology of blunt trauma during the 30-year period evaluated in this study.
Testicular injury usually presents with acute scrotal swelling, pain, and ecchymosis. Skin lacerations or loss can also occur. Due to severe swelling and pain, adequate physical examination might be difficult (12). Indeed, significant testicular injury cannot be excluded by a lack of tenderness (2). Therefore, for precise diagnosis and proper treatment, imaging studies are necessary. The most sensitive and specific imaging modality for diagnosis of testicular injury is scrotal ultrasonography (14151617). The integrity and vascularity of the testis can be evaluated by scrotal ultrasonography, so that rupture of testis can be distinguished from hematocele, hydrocele, testicular torsion, or epididymitis (12). According to our experience, the correlation between preoperative ultrasonographic and surgical findings showed a moderate to strong degree of correlation. Ultrasonographic sensitivity and specificity for the diagnosis of testicular rupture were 76.7% and 100%, respectively.
A missed testicular rupture results in not only testicular atrophy, secondary infection, chronic pain, and infertility but also psychological problem such as altered self-image (2). Therefore, when rupture of the testis is suspected, immediate surgical exploration is recommended. Many studies suggested that early exploration reduces morbidity and the length of hospital stay (8111819). Ninety percent of injured testis can be salvaged if treated properly within 72 hours of injury (420212223). However, this decreases to 30% when the patient receives treatment more than 72 hours after injury (212425). During surgery, the injured testis should be irrigated and necrotic tissues must be debrided. Watertight closure with absorbable suture material should be applied to the lacerated tunica albuginea. Seven-day administration of broad-spectrum antibiotics is needed after surgery (12). On the other hands, conservative management with rest and scrotal elevation might be adequate for stable scrotal hematomas.
Over the past 30 years, 115 patients with testicular injury presented to our medical center. Similar to previous reports (1011), most injuries (92.7%) were caused by blunt trauma and only 9 patients were treated for penetrating testicular injury. However, the etiology of blunt trauma from our experience was different from that of western studies. The most common etiology of blunt trauma was an assault, which was the second most common cause in the western studies. However, the trends of etiology are changing. In the first decade, the proportion of cases due to assault was 54.8%, decreasing to 23.1% during the third decade. In contrast, the proportion of injuries due to athletic activity and falls increased from 9.7% and 12.9% to 23.1% and 32.7%, respectively. In addition, the severity of testicular injury during the third decade was milder than that of the first or second decade. Intentional assault can lead to severe testicular injury. In recent years, the severity of testis trauma has declined as the rate of testis injury from assault has decreased. All included patients underwent consultation with a urologist within 72 hours from the initial trauma, so that most injured testes could be salvaged unless the injuries were severe. This early consultation could be due to the Korean Healthcare system, which makes it easy to for patients to see doctors. Nevertheless, 11 patients underwent removal of the injured testis, not due to delayed treatment but due to the severity of injury. Among patients who underwent surgical treatment and testis salvage, only two patients had testicular atrophy. Both patients had abnormal findings on scrotal ultrasound, such as heterogeneous echo pattern of injured testis and intra- and extra-testicular hematoma. During the surgery, a severely lacerated tunica albuginea and intra- or extra-testicular hematoma were detected. According to these findings, we could verify that ultrasonographic findings before treatment are important. This is in concordance with previous reports (14151617). Compared with ultrasonographic and surgical findings, both sensitivity and specificity of scrotal ultrasound for the diagnosis of testicular rupture were high. The most important findings on scrotal ultrasound were a heterogeneous echo pattern of the testis and loss of contour definition, which correlated with laceration of the tunica albuginea or testicular destruction. Furthermore, intra- and extra-testicular hematoma was another important finding for the diagnosis of lacerated tunica albuginea or destructed testis. Therefore, if patients with scrotal injury show these findings on scrotal ultrasound, early exploration of the scrotum is mandatory.
The present study was retrospective in design, and thus has some limitations. First, because it was a single center study, the number of included patients is relatively small and there may be a selection bias. Therefore, our experience cannot be generalized to all patients with testicular injury in Korea. However, considering that the incidence of scrotal injury is low compared to that of other injuries, our experience seems to reflect the patterns and trends of testicular injury in Korea. In addition, there has been no study with data from a single center covering a 30-year period. Another considerable limitation is that ultrasonography is a subjective modality. Therefore, ultrasonographic findings performed by different observers may be inconsistent. To overcome this limitation, in our medical center, scrotal ultrasound was usually performed and evaluated by both a urologist and radiologist. Moreover, ultrasonographic findings, such as contour or echo pattern of testis and hematoma pattern, were well described so that we could perform the present study.
In conclusion, the trend of testicular injuries has changed over 30 years. Although the etiology and severity of injury have changed, scrotal ultrasound for determining an appropriate management strategy in scrotal trauma is important. According to our experience, we conclude that if abnormal findings are detected on scrotal ultrasound, surgical exploration is mandatory.
 XML Download
XML Download