

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Approximately 20% to 30% of patients will present with muscle-invasive bladder cancer (MIBC) at the time of initial diagnosis. Because this is one of the most aggressive epithelial tumors, a significant proportion of patients will experience recurrence, and approximately 50% of cystectomy patients will ultimately die of disease despite therapy (1). Radical cystectomy (RC) with bilateral pelvic lymph node dissection (PLND) is the treatment of choice for clinically localized MIBC and has also been performed for patients with aggressive non-MIBC (NMIBC). Nevertheless, this procedure still has a 50% 2-year risk of distant metastasis and a 60% 5-year risk of death in patients with MIBC (2).
Robot-assisted radical cystectomy (RARC) has been emerging as an equivalent approach to open RC with potentially equivalent oncological outcomes (3). Moreover, it has been suggested that RARC results in improvements in perioperative morbidity and ease of recovery, as well as permitting earlier initiation of adjuvant systemic therapies (45). However, despite these potential perioperative benefits (6), RARC has been criticized for the paucity of reports regarding long-term oncologic outcomes (7). Despite the fact that early oncologic outcomes appear to be favorable, longer-term follow-up studies are still lacking (89).
In this multicenter study, we analyzed intermediate-term oncologic outcomes following RARC with bilateral PLND in 346 patients with bladder cancer (BC). In addition, we analyzed predictive risk factors and patterns of recurrence in comparison to the findings of previous studies.
MATERIALS AND METHODS
After approval was obtained from the Institutional Review Board at each center, we retrospectively reviewed patient databases. We identified 346 patients treated with RARC between 2007 and 2015 at six institutions in Korea.
Study participants included patients with recurrent/multiple or high-grade superficial or MIBC without evidence of metastatic disease on preoperative imaging (10). High-grade superficial BC was defined as pT1G3 tumors, and recurrent BC was defined as pTaG1G2 BC that had recurred despite three or more transurethral resections. The criteria also include bacillus Calmette-Guérin refractory tumors, defined according to the European Association of Urology guidelines (11). Eligible patients were medically cleared for RC with PLND, aged ≥ 18 years, and had clinical stage Ta–T4/N0–N3/M0 BC. Exclusion criteria included clinical stage M1, any contraindication to the Trendelenburg position, or prior “extensive” abdominal surgery.
The surgical technique of RARC with bilateral PNLD and urinary diversion (UD) has been previously described (12). Standard PNLD was most commonly used in patients included in the current study; this technique consists of excising lymphatic tissue from the external iliac artery, external iliac vein, obturator nerve, and hypogastric artery up to the common iliac artery. Extended PLND includes standard PLND in addition to resection of tissue medial to the genitofemoral nerve and along the common iliac artery up to the aortic bifurcation. UD was performed mostly extracorporeally in the current study population, and was performed intracorporeally in 53 (15.3%) subjects.
The endpoint of the present study was the identification of predictive factors for recurrence and recurrence patterns. Logistic regression was performed for analysis of variables to identify predictive factors for recurrence. Potential predictors included diversion technique (ileal conduit vs. orthotopic bladder substitution [OBS]), corporeal type (extracorporeal vs. intracorporeal), mean time to Foley removal, mean hospital stay, surgical margins, type of PLND (extended vs. standard), lymph node (LN) yield, pathologic tumor stage, and nodal stage. Tumor grade and pathologic stage were determined using the 2002 American Joint Committee on Cancer tumor, node, and metastasis (TNM) staging system and the 2004 World Health Organization/International Society of Urologic Pathologists classification of papillary urothelial neoplasms, respectively (13).
Additional endpoints included overall survival (OS), cancer-specific survival (CSS), and recurrence-free survival (RFS). OS was defined as the time from date of cystectomy to death due to any cause. CSS was defined as the time to death due to BC, whereas RFS was defined as the time from date of cystectomy to local or metastatic recurrence, based on histologic or radiologic evidence. The estimated distributions of OS, CSS, and RFS were obtained using Kaplan-Meier analysis. The log-rank test was used to compare the Kaplan-Meier curves among pathologic tumor stage, type of LN dissection, LN density, and margin status. All analyses were performed using SPSS software (version 20.0; SPSS Inc., Chicago, IL, USA). P values < 0.05 were considered statistically significant.
RESULTS
Baseline data
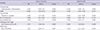
Basic characteristics of patients and perioperative outcomes are shown in Table 1. The mean age of patients was 65.7 ± 10.6 years (interquartile range [IQR], 60.0–73.0). Among the patients, 296 (85.5%) were men, and 36 (10.4%) received neoadjuvant chemotherapy. The types of UD included ileal conduit (38.4%), OBS (57.2%), and continent cutaneous urinary diversion (CCUD; 4.3%). Diversion types included extracorporeal (80.3%), intracorporeal (15.3%), and CCUD (4.4%). The numbers of patients who underwent standard PLND and extended PLND were 179 (51.7%) and 167 (48.3%), respectively.
Table 1
Baseline characteristics of patients and perioperative parameters

Values are presented as number (%) or mean ± SD.
IQR = interquartile range, BMI = body mass index, ASA = American Society of Anesthesiologists, UD = urinary diversion, OBS = orthotopic bladder substitution, CCUD = continent cutaneous urinary diversion, PLND = pelvic lymph node dissection, EBL = estimated blood loss, SD = standard deviation.
Oncologic outcomes
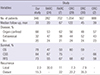
The number of patients with high tumor grade was 269 (77.7%), and 237 (68.4%) patients had organ-confined disease. Rates of LN density (1–20 vs. > 20) were 13.6% and 6.1%, respectively, while 278 patients (80.3%) had node-negative disease. LN yield was 17.1 ± 12.0 (IQR, 9–23), which included yields of 10.7 ± 12.0 and 24.0 ± 11.9 in standard and extended PLND, respectively. Nine patients (2.6%) had positive surgical margins (PSMs) (T1/T2: 1.2%; T3/T4: 1.4%) (Table 2).
Table 2
Pathologic outcomes

Predictive factors and patterns of recurrence
In logistic regression analysis, the type of LN dissection was a significant predictor of recurrence and death from cancer (odds ratio [OR], 2.816; 95% confidence interval [CI], 1.27–6.20; P < 0.001 and OR, 5.953; 95% CI, 2.25–15.65; P = 0.001, respectively), as was pathologic tumor stage (OR, 2.417; 95% CI, 1.36–4.30; P = 0.003 and OR, 3.804; 95% CI, 1.80–8.05; P < 0.001, respectively). PSM (OR, 10.916; 95% CI, 1.90–62.57; P = 0.007), LN yield (OR, 0.946; 95% CI, 0.91–0.99; P = 0.010), and positive LN (OR, 1.087; 95% CI, 1.01–1.17; P = 0.026) showed statistical significance for cancer recurrence, while corporeal type did not show significance (P = 0.056) (Table 3).
Table 3
Logistic regression analysis of variables associated with recurrence and death from BC after treatment with RARC
Local and distant recurrence occurred in 7 (2.0%) and 53 (15.3%) patients, respectively. Regarding local recurrence, 6 patients experienced recurrence on the cystectomy bed, while only 1 patient experienced recurrence on the PLND template. In terms of distant recurrence, the lung (15/53) was the single most common site, followed by extrapelvic LN (13/53), bone (7/53), and the liver (4/53). Nine patients had multiple recurrence sites (9/53). Another 4 patients experienced recurrence of secondary urothelial carcinoma (UC) in the upper urinary tract (2 patients) and urethra (2 patients). The distribution of recurrence locations is shown in Fig. 1.

Kaplan-Meier curves for OS, CSS, and RFS
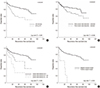
The Kaplan-Meier curves show the OS, CSS, and RFS. The 5-year OS, CSS, and RFS rates were 78%, 84%, and 73%, respectively (Fig. 2). We analyzed RFS at the last follow-up according to several factors to determine their effect on recurrence. In the present study, the presence of non-organ confined disease (> pT2) was a significant predictor of RFS (organ-confined vs. non-organ-confined: 68% and 51%; log-rank test: P < 0.001; Fig. 3A). At the last follow-up, RFS for extended PLND vs. standard PLND was 70% and 47%, respectively (P = 0.038; Fig. 3B). At the time of last follow-up, LN density (0 vs. 1–20 vs. over 20) was 67%, 41%, and 29%, respectively (P < 0.001; Fig. 3C). Furthermore, a PSM was associated with a significantly increased risk of disease recurrence compared to a negative surgical margin (64% and not calculable, respectively; P < 0.001; Fig. 3D).
Fig. 2
Kaplan-Meier curves for: OS of 93%, 84%, and 78% for 1-, 3-, and 5-year, respectively; CSS of 94%, 87%, and 84% for 1-, 3-, and 5-years, respectively; RFS of 88%, 78%, and 73% for 1-, 3-, and 5-years, respectively.
OS = overall survival, CSS = cancer-specific survival, RFS = recurrence-free survival.
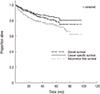
Fig. 3
Kaplan-Meier curves for oncologic outcome. (A) RFS at last follow-up for organ-confined vs. non-organ-confined disease was 68% vs. 51%, respectively (P < 0.001); (B) RFS at last follow-up for extended and standard PLND was 70% vs. 47%, respectively (P = 0.038); (C) RFS at last follow-up between LN density was 67%, 41%, and 29%, respectively (P < 0.001); and (D) RFS at last follow-up for negative vs. positive soft tissue margin status was 64% vs. not calculable, respectively (P < 0.001).
RFS = recurrence-free survival, PLND = pelvic lymph node dissection, LN = lymph node.
DISCUSSION
In our study, analysis of oncologic outcomes in intermediate term follow-up was the primary endpoint. The results of our multicenter trial demonstrated similar oncologic results and predictive factors for recurrence compared with other studies. The 3- and 5-year OS, CSS, and RFS were slightly higher than those found in contemporary RARC series. Pathologic tumor stage, extent of PLND, LN density, and PSM were significant prognostic factors with regard to RFS.
We analyzed predictive risk factors for recurrence in comparison to previous studies. It is known that LN status is the most powerful surrogate prognostic marker for long-term RFS and OS following RC (14). In the present study, a median of 17 LNs were removed (IQR, 9–23). There is no general consensus in the literature regarding the exact threshold of nodes at which a survival benefit can be predicted, with most studies reporting numbers in the range of 9 to 16 (14).
In terms of PLND extent, the current study did not reveal unusual results compared to those of previous studies. One criticism of RARC is that the extended PLND cannot be as complete as that in open RC due to limitations in accessing the nodes at the aortic bifurcation. However, recent RARC series reveal LN yields comparable to those observed in open RC series (1516). In the current study, compared with standard PLND, extended PLND resulted in significantly reduced risk of recurrence and death from BC (P = 0.001 and P < 0.001, respectively). In addition, at the last follow-up, there was a significant difference in RFS for extended PLND vs. standard PLND (P = 0.038). PLND is considered an integral part of RC and there are some evidences that the greater number of nodes removed during RC, the better the chance of long-term survival (17). A few studies have argued that this finding is the result of a Will Rogers phenomenon, an apparent paradox obtained from moving cases from the pN0 to the pN+ group, which might account for the better results observed with extended PLND. However, one important reason for performing extended PLND is that, although “skip” metastasis appears to be a relatively rare event in BC, cases have been reported in the literature (18). This means that the obturator fossa is not necessarily the first site of BC metastasis. In addition, several previous studies have reported a survival benefit with extended PLND or in accordance with increasing numbers of removed LNs (1920).
Another prognostic factor for RFS observed in our study was LN density (P < 0.001). LN density refers to the number of LNs containing metastatic deposits divided by the total number of nodes removed. Several studies have suggested that LN density could have prognostic value, and some studies have suggested that LN density is superior to the TNM classification system, as well as to the absolute number of positive LNs, in predicting OS and CSS (21). In addition, a recent meta-analysis showed that LN density could be an independent predictor of clinical outcomes in LN-positive patients (22).
Margin status is also an important prognostic factor for RFS following RC (23). A PSM was associated with a significantly increased risk of disease recurrence. In the present study, 9 patients (2.6%) had PSMs, similar to the findings of a previous study (24). Furthermore, a PSM was associated with a significantly increased risk of disease recurrence compared to a negative surgical margin (P = 0.007).
Meanwhile, with emerging surgical techniques, continued assessments are necessary to ensure optimization of outcomes. Some authors have reported that there could be a distinct pattern of recurrence following RARC. Nguyen et al. (25) reported that extrapelvic LN locations and peritoneal carcinomatosis were more frequent following RARC than open RC in patients with distant recurrence. This is a matter for consideration, since recurrence patterns of cancer could have a great effect on patient survival. Therefore, another aim of this study was to determine whether or not recurrence patterns were unusual in patients undergoing RARC with PLND.
Regarding distant recurrence in solid organs, the lung, bone, and liver remained the most frequent sites, a finding consistent with previous studies (26). The recurrence of extrapelvic LN metastasis (3.8%) was similar to that observed in previous open RC series (325). However, in the present study, some cases of extrapelvic LN recurrence were concentrated in the initial period following the performance of RARC, which could be a reason for the relatively higher rates of distant recurrence. Another concern regarding RARC was the higher rate of peritoneal carcinomatosis, which implies cancer cell dispersal by pneumoperitoneum. In the current study, no recurrence of peritoneal carcinomatosis was observed. We investigated the recurrence of secondary UC separately. This is important because the follow-up strategy should reflect the risk or extravesical recurrence (in particular, the prostatic urethra in men, as well as the upper urinary tract) (27). This result did not show a significant difference compared with the findings of previous studies (25).
In the present study, 5-year OS, CSS, and RFS were 78%, 84%, and 73%. In a small set of patients who received more than 5 years of follow-up, patients undergoing RARC experienced an OS of 64%, CSS of 75%, and RFS of 50% (8). A series of 121 patients who underwent RARC provides additional longer follow-up data, with a median follow-up of 5.5 years. In this study, the OS, CSS, and RFS were 48%, 71%, and 65% at 5 years, and 35%, 63%, and 54% at 10 years (28). The survival results obtained in the current study suggest that the enrolled patients had more favorable oncologic outcomes compared with previously reported RARC series. In fact, the rate of organ-confined disease according to pathologic results was relatively higher in comparison to other studies from high-volume centers. We adduced oncologic comparative data in Table 4.
Table 4
Percentage of patients according to disease characteristics (organ-confined or extravesical or node positive) and survival analysis in a large series of RC for UC of the bladder (our study/RARC/ORC)
There are several limitations to our study, foremost the limitations inherent to retrospective analyses. Therefore, our study is limited by biases such as lack of random assignment, patient selection, and incomplete data acquisition. It should also be noted that the present findings apply to patients treated by an experienced surgeon, at a high-volume tertiary care center. This may limit the generalizability of these findings to low-volume community-based practices. In addition, the patients in this study underwent RC performed by multiple surgeons and had specimens evaluated by multiple pathologists. However, all surgeons operated at selected centers with significant experience in BC management, which might increase the external validity of the data compared to the single center, single surgeon setting.
In conclusion, we found that oncologic outcomes and predictive factors for recurrence were not unusual in intermediate-term follow-up among patients who underwent RARC. In addition, there were no significant differences in recurrence patterns compared with open RC. Further validation would be warranted to better understand the oncologic outcomes of RARC for UC.
 XML Download
XML Download