

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Subclinical thyroid disease is comprised of subclinical hyperthyroidism and subclinical hypothyroidism, which are characterized by abnormal thyroid stimulating hormone (TSH) with normal free thyroxine. Although subclinical thyroid diseases are common in middle-aged and elderly individuals (1), they receive less attention compared with other overt thyroid diseases due to their asymptomatic clinical characteristic. However, several studies have demonstrated that subclinical thyroid diseases are associated with increased risk of cardiovascular disease (CVD) (2). For subclinical hyperthyroidism, several large prospective cohort studies showed an increased risk of coronary heart disease mortality, incident atrial fibrillation, and heart failure in patients with serum TSH levels < 0.1 mIU/L (2). For subclinical hypothyroidism, previous studies demonstrated the association between hypercholesterolemia and atherosclerosis, which can elevate the risk of CVD (3). Moreover, in a recent meta-analysis, subclinical hypothyroidism was shown to actually be correlated with increased risk of CVD and mortality (4). Therefore, concerns about screening and treatment to prevent CVD have also been magnified in patients with subclinical hypothyroidism (5).
The biochemical reference range for defining subclinical thyroid diseases is dependent on the serum TSH levels, which can be affected by multiple factors, such as age, gender, smoking, body mass index (BMI), iodine intake, and thyroid autoantibodies (67). A recent Korean study with subjects between the age 20 and 79 years using institutional routine health check-up data demonstrated that the serum TSH levels in a Korean reference population were higher (0.73–7.06 mIU/L) than those reported in other countries (0.4–4.2 mIU/L) (8). Relevant research using the data of the Korea National Health and Nutrition Examination Survey (KNHANES) VI also showed similar results regarding the serum TSH levels (0.62–6.68 mIU/L) in a Korean reference population who were 10 years or more (9). Therefore, there is a possibility that the relationship between subclinical thyroid diseases and CVD risk may show a different characteristic compared with previous results usually conducted in Western countries.
The Framingham risk score has been renowned as a 10-year CVD risk score model that most reliably predicts CVD events and mortality in the next 10 years with subjects of baseline examinations free of CVD, who were 30 years or more (101112). The predictors used in the risk model are age, gender, total cholesterol, high-density lipoprotein (HDL) cholesterol, systolic blood pressure (SBP), treatment status of hypertension or diabetes, and smoking status (12), which we can easily obtain from large population-based data. Nevertheless, there have been a few studies investigating the relationship between subclinical thyroid diseases and the 10-year CVD risk score to date.
Therefore, the objectives of this study were to verify the association between subclinical thyroid diseases and 10-year CVD risk score in the Korean population who are 30 years or more, and to establish a new TSH reference range extracted from KNHANES VI data.
MATERIALS AND METHODS
Study participants
This study was performed using the data obtained from the KNHANES VI study (2013 to 2015), a cross-sectional and nationally representative survey conducted on non-institutionalized individuals by the Division of Chronic Disease Surveillance, Korea Centers for Disease Control and Prevention. The KNHANES data is obtained from 3,840 individuals, randomly chosen from 192 regions in Korea, on an annual basis, using a stratified, multistage sampling procedure. The survey was comprised of a health interview, a health examination, and a nutrition survey. The data were collected via household interviews and standardized physical examinations were conducted at mobile examination centers. Treatment status was defined as patients currently taking antihypertensive medications. Subjects were classified as having diabetes mellitus if their fasting plasma glucose was ≥ 126 mg/dL or they reported actively using an oral hypoglycemic agent or insulin on the health survey. Patients currently taking oral hypoglycemic agents or insulin were defined as treatment status of diabetes. The KNHANES database is publicly available at the KNHANES website (available at http://knhanes.cdc.go.kr/knhanes/eng). Following the criteria based on the Framingham Heart Study data, subjects without prevalent CVD who were 30 to 74 years of age were included in this study (12). Stroke, myocardial infarction, and angina pectoris were defined as CVD in the KNHANES data. Pregnant women were excluded from the reference population, since it is possible for physiologic changes to affect thyroid function. Finally, we included a reference population of 3,722 subjects (1,922 males and 1,800 females) with no history of thyroid disease, no history of taking medications that could affect thyroid function, no family history of thyroid disease, negative anti-thyroid peroxidase antibody (TPOAb) results (less than 35 IU/mL), and serum-free T4 (fT4) levels in the reference range (0.80 to 1.80 ng/dL).
Data extraction
The TSH reference range was defined to be between 2.5th and 97.5th percentile of the reference population. Subclinical thyroid disease groups were categorized into three groups; subclinical hyperthyroidism, euthyroidism that is normal, and subclinical hypothyroidism, by cutoff of TSH. The reference population with a TSH range of below the 2.5th percentile was defined as subclinical hyperthyroidism and those of above the 97.5th percentile as subclinical hypothyroidism.
We used a gender-specific algorithm enabling physicians to identify candidates with high-risk atherosclerotic CVD events using measurements readily available at the clinic or at the office. In accordance with the gender-specific 10-year CVD risk score prediction formula (12), we calculated the risk scores of subjects based on their age, gender, total cholesterol, HDL cholesterol, SBP, treatment status of hypertension, and diabetes, as well as smoking status for males and females, respectively.
Biochemical measurements
Blood samples were collected from the antecubital vein of each participant after overnight fasting to obtain the levels of serum TSH, fT4, TPOAb, total cholesterol, HDL cholesterol, and white blood cell (WBC) counts. After separation of the serum within 30 minutes, the sample was transferred to the testing facility. The samples were processed, transported to the Central Testing Institute located in Seoul, and analyzed within 24 hours. The levels of serum TSH, fT4, and TPOAb were analyzed using an electrochemiluminescence immunoassay within the first 24 hours (Roche Diagnostics, Mannheim, Germany). TSH was measured using an E-TSH kit (Roche Diagnostics), for which the reference range was 0.35 to 5.50 mIU/L. The fT4 was measured using an E-Free T4 kit (Roche Diagnostics). The fT4 reference range was 0.89 to 1.76 ng/mL. TPOAb was measured using an E-Anti-TPO kit (Roche Diagnostics). The normal range for TPOAb in humans is < 34.0 IU/mL. The reported results of TSH, fT4, and TPOAb levels met the specifications regarding accuracy, general chemistry, special immunology, and ligand of the quality control and quality assurance guidelines set forth by the College of American Pathologist. The levels of total and HDL cholesterols were measured using the homogenous enzymatic colorimetric method (Hitachi Automatic Analyzer 7600-210; Hitachi, Tokyo, Japan). WBC counts were collected using a flow cytometry via a semiconductor laser (XE-2100D and XN-9000; Sysmex, Kobe, Japan). Blood pressure was measured three times at 30 second intervals after a minimum of 5 minute of rest in a seated position, and recorded as an average value of the second and third measurements. Hypertension was defined as SBP above 140 mmHg or diastolic blood pressure (DBP) above 90 mmHg. Urine iodine (UIod) concentrations were measured from the random spot urine samples (first morning urine, if possible) of the study populations via an inductively coupled plasma mass spectrometry devise (ICP-MS; Perkin Elmer ICP-MS, Waltham, MA, USA). UIod concentrations were measured using an Iodine standard (Inorganic Venture, Christiansburg, VA, USA).
Statistical analysis
The value of CVD risk score was log-transformed due to non-normality. All statistical analyses were performed after stratification by gender, since the CVD risk score was a gender-specific value. The weighted results were estimated using survey sample weight variables for the associations between health interview and health examination. The association between clinical variables and log 10-year CVD risk score was identified using simple and multiple linear regression analyses for the complex survey. We estimated the least squares means (LS means) of log 10-year CVD risk score for the effect according to the subclinical thyroid disease group compared with the euthyroidism group in the generalized linear model, after adjusting for BMI, WBC, and UIod. The LS means specify the predicted marginal mean over the balanced population. We also tested differences of the LS means of log 10-year CVD risk score using pairwise Wald χ2 test with Bonferroni correction for multiple comparisons. Statistical analyses were performed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA). A P value of less than 0.05 was considered to be statistically significant (two-tailed).
RESULTS
TSH reference range of the study population
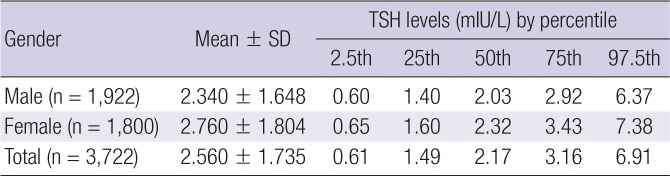
The distribution of TSH level is shown in Table 1. In this study population, the TSH reference range was defined as being between 0.61 (2.5th percentile) to 6.91 mIU/L (97.5th percentile). The TSH reference range in males (0.60–6.37 mIU/L) tended to be lower than that in females (0.65–7.38 mIU/L). A population with less than 0.61 mIU/L of TSH was considered to have subclinical hyperthyroidism, those in between 0.61 to 6.91 mIU/L to have euthyroidism, and those with greater than 6.91 mIU/L to have subclinical hypothyroidism.
Table 1
Distribution of TSH in the study population
Baseline characteristics of the study population
The clinical characteristics of 1,922 males and 1,800 females are shown in Table 2. There were 90 subjects (50 males and 40 females) considered to have subclinical hyperthyroidism, 3,540 subjects (1,840 males and 1,700 females) to have euthyroidism, and 92 subjects (32 males and 60 females) to have subclinical hypothyroidism. The mean age (± standard deviation) for males (49.32 ± 11.70 years) was similar to that for females (49.11 ± 11.62 years). HDL cholesterol level seemed high in females (53.55 ± 11.65) compared with males (47.42 ± 11.21), which was also the case for each subgroup of study population (i.e., subclinical hyperthyroidism, euthyroidism, and subclinical hypothyroidism). The cigarette smoking rate was much higher in males (42.8%) than in females (5.8%). There was a difference in the 10-year CVD risk score between the two genders. The 10-year CVD risk score in males seemed higher (12.75 ± 11.75) than that in females (5.14 ± 5.99), which was also found in each subgroup of subclinical hyperthyroidism, euthyroidism, and subclinical hypothyroidism. The distributions of the other factors were similar between males and females.
Table 2
Baseline characteristics of study population
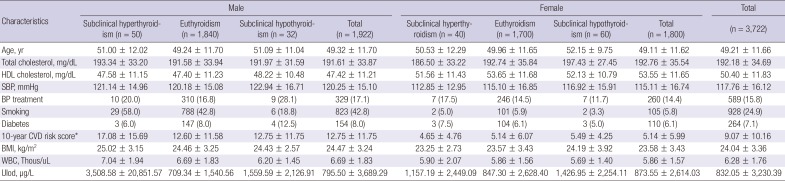
Data are shown as mean ± standard deviation or number (%).
HDL = high-density lipoprotein, SBP = systolic blood pressure, BP = blood pressure, CVD = cardiovascular disease, BMI = body mass index, WBC = white blood cell, UIod = urine iodine.
*The 10-year CVD risk score was calculated based on each subject's age, gender, total cholesterol, HDL cholesterol, SBP, treatment status of hypertension or diabetes, and smoking status according to the gender-specific CVD risk prediction formula (12).
Association between TSH and 10-year CVD risk score by gender
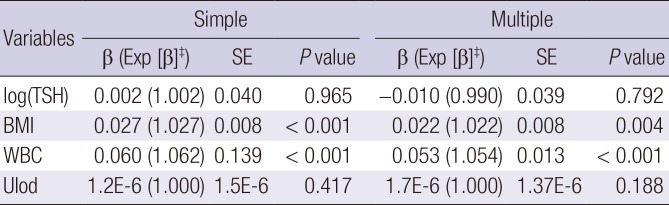
Since the 10-year CVD risk score was different based on gender, we examined the association between TSH (log-transformed) and 10-year CVD risk score separately for each gender (Tables 3 and 4). TSH showed a significantly positive association with 10-year CVD risk score, after adjusting for confounding factors (such as BMI, WBC, and Ulod) in females (P = 0.008), but not in males (P = 0.792). BMI was statistically significant in each gender. WBC was significantly associated with the 10-year CVD risk score, after adjusting for confounding factors, in males only (P < 0.001). UIod showed no significance in both genders.
Table 3
Association* between TSH and 10-year CVD risk score† (male population)
TSH = thyroid stimulating hormone, CVD = cardiovascular diseases, SE = standard error, BMI = body mass index, WBC = white blood cell, UIod = urine iodine.
*Simple and multiple linear regression model were executed for the complex survey in males. †Log-transformed 10-year CVD risk score was regressed due to non-normality on residuals. ‡Exponentially transformed β coefficient in the fitted model.
Table 4
Association* between TSH and 10-year CVD risk score† (female population)

TSH = thyroid stimulating hormone, CVD = cardiovascular diseases, SE = standard error, BMI = body mass index, WBC = white blood cell, UIod = urine iodine.
*Simple and multiple linear regression model were executed for the complex survey in females. †Log-transformed 10-year CVD risk score was regressed due to non-normality on residuals. ‡Exponentially transformed β coefficient in the fitted model.
Association between subclinical thyroid diseases and 10-year CVD risk by gender
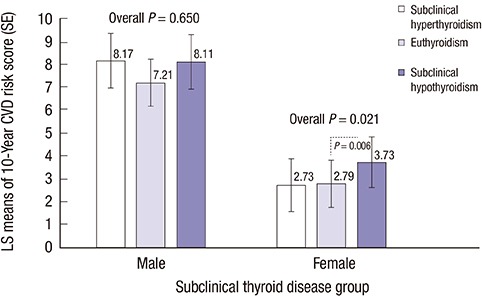
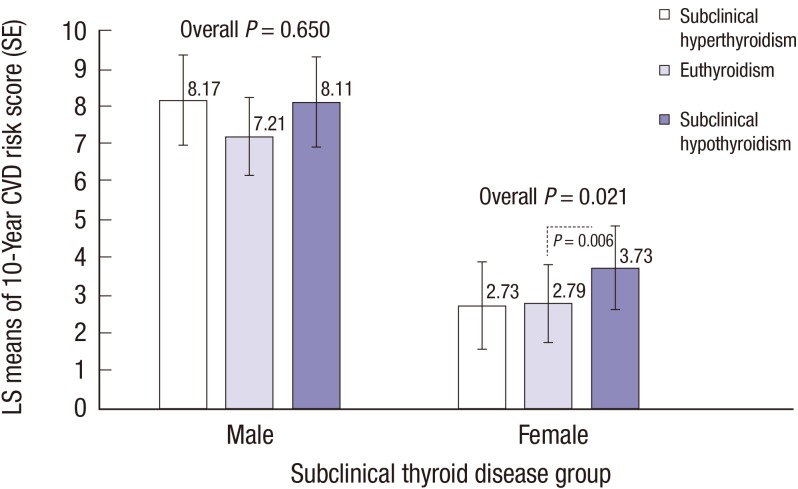
Following the results of Tables 3 and 4, we explored which group of subclinical thyroid diseases significantly conferred a risk of increased 10-year CVD risk score after stratification by gender (Fig. 1). Adjusted means of log 10-year CVD risk score by group of subclinical thyroid diseases tended to be higher in males than those in females. Significant differences were identified between groups in females (overall P = 0.021), but not in males (overall P = 0.650). In particular, there was a significant difference in the LS means of 10-year CVD risk score by the effect of subclinical hypothyroidism group compared with euthyroidism (normal group) in females, after adjusting for BMI, WBC, and UIod (P = 0.006 and Bonferroni corrected P = 0.012). However, there was no significance between subclinical hyperthyroidism and euthyroidism group in females (P = 0.877).
Association between TSH and components of 10-year CVD risk score
To explain the reason of a positive association between TSH and 10-year CVD risk, we performed correlation analyses between TSH (log-transformed) and the components of 10-year CVD risk score in the Framingham formula for males and females, respectively. Among the components of age, gender, total cholesterol, HDL cholesterol, SBP, treatment status of hypertension or diabetes, and smoking status, smoking was correlated with increased log (TSH) both in males (correlation coefficient ρ = 0.183; standard error [SE] = 0.032; P < 0.001) and in females (ρ = 0.204; SE = 0.072; P = 0.005). In females, age (ρ = 0.003; SE = 0.001), total cholesterol and SBP (ρ = 0.002; SE = 0.001) were also positively correlated with log (TSH) (P < 0.05).
DISCUSSION
In this study, the TSH reference range was defined to be 0.61–6.91 mIU/L based on the TSH distribution data of 3,722 subjects included in KNHANES VI. The association between subclinical thyroid disease and CVD risk has not been established and remained controversial. Several studies indicated increased CVD risk for those with subclinical thyroid disease. From prospective cohort studies, subclinical hypothyroidism was associated with increased risk of CVD events and CVD mortality (13). Subclinical hyperthyroidism was also relevant with increased risks of total CVD mortality and incidences of atrial fibrillation (1415). Whereas, another study including a total of 344 subclinical hypothyroidism and 2,624 euthyroid participants aged over 40 years showed that additional assessments of serum TSH levels provided little incremental benefits for the prediction of CVD risk (16). However, these studies usually applied a common TSH reference range without considering the factors that may affect serum TSH levels, such as age and race. In this context, our study firstly showed the association of TSH and 10-year CVD risk score with the applicability of a new TSH reference range that is appropriate for representing the Korean population who are 30 years or more.
Since thyroid hormone, such as triiodothyronine, controls the inotropic and lusitropic properties of myocardium, cardiac growth, and myocardial contractility, hypothyroidism causes a low cardiac output with decreased heart rate and stroke volume (1718). Vascular function is also deteriorated even in mild thyroid hormone deficiency (19). Moreover, hypothyroidism is accompanied by the hypercoagulable state, increased blood viscosity, and high plasma concentration of total homocysteine. Since these cardiovascular deteriorations may also be relevant with subclinical hypothyroidism (202122), a careful prediction of CVD risk or CVD events, in addition to creating an appropriate indication for treatment in these patients, is important. Moreover, the increased risk of coronary heart disease and mortality was even reported in young patients affected by subclinical hypothyroidism with serum TSH levels > 10 mIU/L (1323). In the same context, the 2013 European Thyroid Association (ETA) guideline recommended a levothyroxine replacement therapy for patients aged less than 65–70 years with serum TSH > 10 mIU/L (242526), despite being asymptomatic. Moreover, in these patients, treatment should also be considered when the serum TSH levels are below 10 mIU/L, if these patients have any evidence of heart disease.
We demonstrated that there was a positive, significant association between TSH and 10-year CVD risk score in Korean females, but not in Korean males. Moreover, the 10-year CVD risk score was also significantly higher in females of the subclinical hypothyroidism group than in euthyroid females. Our additional correlation analyses between TSH and the components of 10-year CVD risk score in the Framingham formula showed that age, total cholesterol and SBP may affect increased TSH among the components of 10-year CVD risk score in females. In agreement with our findings, higher cholesterol level has been reported to be associated with higher TSH levels in females (27). Anagnostis et al. (27) demonstrated that atherogenic lipid profiles (high low-density lipoprotein [LDL] and low HDL) were associated with a risk of high TSH in females, even though a more atherogenic lipid profile was generally shown in males than females. The study of Meng et al. (28) verified that males who suffered from hyperlipidemia showed a protective effect of low TSH, while females in hyperlipidemia showed a risk of high TSH. In the 11-year follow-up of the Nord-Trøndelag health study (HUNT) (29), higher SBP and DBP were associated with higher TSH in females, which was consistent with our findings of this study. Furthermore, biochemical abnormalities and physiological changes may explain the increased risk of CVD in females with subclinical hypothyroidism.
This study has several strengths. First, it is the first nationwide epidemiological study investigating the association between subclinical thyroid disease and Framingham risk score in Koreans. We used a new TSH reference range that is appropriate for representing the Korean population who are 30 years or more. Second, this research can suggest a treatment like levothyroxine for females with subclinical hypothyroidism. In Korea, the study of subclinical thyroid disease has a tendency of little interest because it shows rare symptoms, and the recent recommendations regarding this disease have not been widely adopted. Although more clinical trials regarding this issue should be performed in the future studies, this study can be a milestone for subclinical thyroid disease.
However, there are also some limitations to consider. First, we were unable to confirm a causal relationship between TSH and 10-year CVD risk score due to the cross-sectional nature of the study. Second, we could not consider other factors that may have affected the TSH levels, such as high-sensitivity C-reactive protein (hs-CRP), other autoimmune antibodies, pregnancy or 24-hour iodine intake amount (30313233343536). In particular, there are several results regarding the correlation between hs-CRP concentration and subclinical hypothyroidism. Hs-CRP can be regarded as a contributing factor. We suggest future studies regarding the subclinical thyroid disease and hs-CRP. Lastly, spot UIod concentration data might have some possible observation bias due to a daily variability in iodine intake. A 24-hour urine sample data or UIod to creatinine ratio in random single voided urine can be more reliable. We were unable to use urine creatinine due to the high missing rate of our data.
To summarize, TSH showed a statistical significance with the 10-year CVD risk in Korean females. Moreover, subclinical hypothyroidism was associated with increased 10-year CVD risk in comparison with euthyroidism in Korean female population aged more than 30 years. Therefore, we recommend to clinically checkup major CVD risk factors in female patients aged more than 30 years with subclinical hypothyroidism.
 XML Download
XML Download