

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Familial Mediterranean fever (FMF) is an autosomal recessive autoinflammatory disease characterized by frequent attacks and chronic inflammation (1). Whereas FMF is widely found among Mediterranean and Middle Eastern populations, sporadic cases have been reported in the Far East (2). Although it usually starts during childhood and progresses with attacks, the disease may be diagnosed late. Therefore, there is a long time between the onset of symptoms and the time patients are diagnosed and their treatment initiated.
During attack periods, proinflammatory cytokines primarily interleukin (IL)-1β are released, and serum levels of acute phase reactants including C-reactive protein (CRP), serum amyloid A, fibrinogen, and erythrocyte sedimentation rates (ESRs) significantly increase (345). Due to the persistent inflammation that occurs in FMF patients (6), they experience severe inflammation during both chronic and acute periods. Oxidative stress (OS) and oxidant/antioxidant imbalance have been demonstrated in FMF patients previously (7). Increased OS may play a role in the persistent subclinical inflammation in FMF. Increased OS is caused by the imbalance between the production and removal of reactive oxygen species which in turn causes an increase in oxidative damage. Oxidant damage has harmful effects on both cellular molecules and cellular/extracellular structures. Dynamic thiol disulphide homeostasis status has critical roles in antioxidant protection. OS is reported to be involved in the prognosis of various diseases and syndromes including cardiovascular disorders, cancer, allergy, some neurological disorders, diabetes, and diabetic retinopathy (8910). Colchicine, the gold standard treatment for FMF blocks the release of cytokines and microtubule depolymerization. Treatment with colchicine suppresses inflammation and the development of amyloidosis (11). However, around 30%–40% of all FMF cases partially respond to colchicine treatment and 5% of them are accepted as colchicine resistant (121314). No exact definition of colchicine resistance is found in the literature (15). But the most commonly accepted “colchicine resistant” definition is a patient having > 6 attacks/year or > 4 attacks in the last 6 months (16).
Thiol-disulfide balance has recently been a frequent topic of discussion. Erel and Neselioglu (17) have recently developed a new, simple and cost-efficient spectrophotometric method for measurement of thiol-disulfide. Thiols are functional groups present in the structure of main proteins. Thiols react with reactive oxygen radicals and become oxidized, and remove these radicals to prevent tissue damage. Reactive oxygen radicals are formed because of increased OS in the environment. Disulfide (DS) bonds form following this oxidation. DS bonds can be reduced back to thiol groups. Measurement of thiol-disulfide levels indirectly shows OS levels. In a study of FMF patients in the attack-free period, thiol levels were found to be lower than healthy controls (18). This result is not surprising because FMF patients suffer from OS. Most probably, to protect the organism, thiol groups in FMF patients may have been bound to reactive oxygen radicals and become oxidized and decreased.
The aim of the present study was to assess whether thiol/disulfide imbalance is related to attack and colchicine resistance in FMF patients.
MATERIALS AND METHODS
Study population
The present study is a cross-sectional study of 118 FMF patients (60 male, 58 female) and 60 healthy individuals (29 male, 31 female) of suitable age and gender. The study included adult FMF patients who had been admitted to our hospital rheumatology clinic and diagnosed with FMF according to Tel-Hashomer criteria (19). The control group consisted of healthy individuals who had been admitted to our hospital's internal medicine and rheumatology clinics and had no diseases detected after physical examination and analyses. People with tobacco and alcohol consumption, chronic medication use (FMF patients using the medication other than colchicine) were excluded from the study. The results of Mediterranean fever (MEFV) gene mutations were saved from hospital records.
Definition of attacks and colchicine resistance in FMF patients
Briefly, the criteria defining FMF attack included all the following: fever (≥ 38°C) lasting from 6 to 72 hours accompanied by painful clinical findings of serositis/arthritis, skin rash and elevated CRP (> 5 mg/L) levels, and/or ESRs (> 20 mm/h). Clinically, colchicine resistance was defined as more than three typical FMF attacks within the last six months despite treatment with with 2 mg of colchicine or more (16).
Blood sampling
For FMF during an attack-free period (FMF-AFP) and healthy controls, peripheral blood samples were obtained after 12 hours fasting. A similar protocol was employed, within the first 24 hours of FMF attack for FMF during an attack period (FMF-AP). Ten mL plain tubes and 2-mL vacuum tubes containing ethylenediaminetetraacetic acid (EDTA) were used. Blood samples were centrifuged at 1,500 g for 10 minutes. ESRs and CRP levels were measured within 3 hours of obtaining samples. Serum samples, which were obtained for thiol and DS studies were immediately frozen at −80°C until analysis. Native thiol (NT), total thiol (TT) and disulphide amounts of the FMF and healthy controls were examined in the same session with the same serum samples.
Biochemical analysis
For CRP, the immunoturbidimetric method with the Beckman Coulter AU5800 clinical chemistry system (normal value: < 5 mg/L; Beckman Coulter, Inc., Brea, CA, USA) was used. The Alifax ESR analyser system modified western blot green method (standard value: < 20 mm/h; Alifax, Polverara, Italy) was used to analyze samples for ESR measurements. Serum NT, TT, and DS levels (µmol/L) were measured using the new, cost-effective spectrophotometric method described previously by Erel and Neselioglu (17). Briefly, reducible DS bonds were first reduced to form free functional thiol groups. Formaldehyde was used to remove unused and consumed sodium borohydride, and after the reaction with 5,5′-dithiobis-(2-nitrobenzoic acid) (DTNB), all thiol groups including both reduced and native groups were determined. The amount of active DS was determined by taking half of the difference between serum TT and NT groups. After the calculation of native and total thiols (-SH), DS amounts (−S-S), the percentage of disulfide/total thiol (DTT)ratios, the proportion of native thiol/total thiol (NTT) ratios and the percentage of disulfide/native thiol (DNT) ratios were calculated (%).
Statistical analysis
All statistical analyses were conducted using SPSS software (version 18; IBM Corp., Armonk, NY,USA). Kolmogorov-Smirnov test was used to detect whether the distribution of groups was homogeneous. Continuous variables with normal distribution were presented as mean ± standard deviation (SD), while continuous variables without normal distribution were presented as median (interquartile range [IQR]). Categorical variables have been shown as percentages or numbers. The groups were compared by using the student's t-test for continuous variables with normal distribution and Mann-Whitney U test for continuous variables with non-normal distribution. Categorical variables were analyzed by using χ2 tests. Correlation analysis among numeric parameters were determined by using the Pearson's and Spearman's correlation test. A P value lower than 0.05 was considered significant.
RESULTS
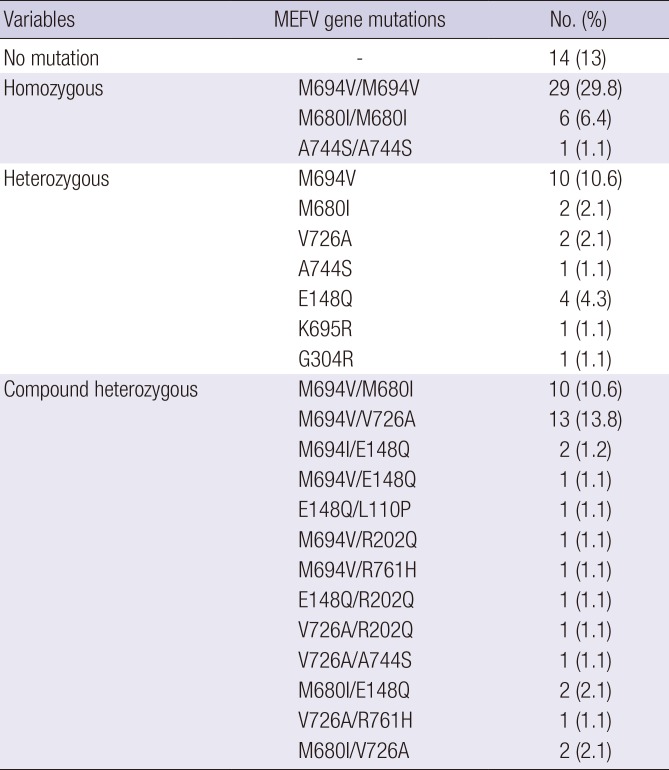
FMF patients and control group were similar in terms of age (35.6 ± 10.1 vs. 36.8 ± 11.6, P > 0.050) and gender distribution (M/F, 60/58 vs. 29/31, P > 0.050). The clinical and demographic characteristics of all FMF patients are presented in Table 1. Seventy-four (60.2%) patients had positive family history and the most common symptom was fever (91.1%). Twenty-four patients (19.5%) were colchicine resistant. Forty-two (34.1%) patients had typical FMF attacks. Table 2 shows the distribution of gene mutations among FMF patients.
Table 1
The demographic and clinical characteristics of FMF patients
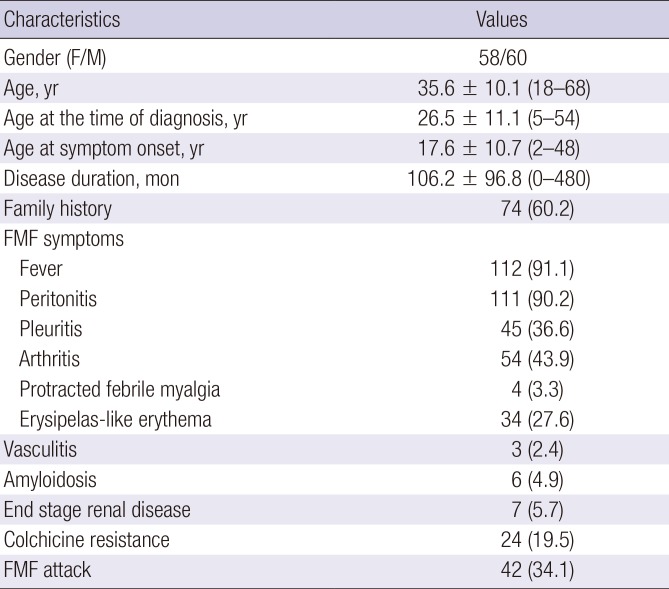
Table 2
MEFV gene mutations in FMF patients
NT (349.9 ± 51.7 vs. 442.2 ± 58.4 µmol/L, P < 0.001), TT (388.1 ± 56.0 vs. 482.1 ± 57.3 µmol/L, P < 0.001), NT/TT (P < 0.001) values of FMF patients were significantly lower compared to the control group. DNT (P < 0.001), DTT (P < 0.001), CRP (P < 0.001), and ESR (P = 0.021) values of FMF patients were remarkably higher compared to the control group. DS value of the FMF group was slightly higher compared to the control group. Thiol and DS values of FMF and the control group are given in Table 3.
Table 3
Laboratory results of the FMF and the control group
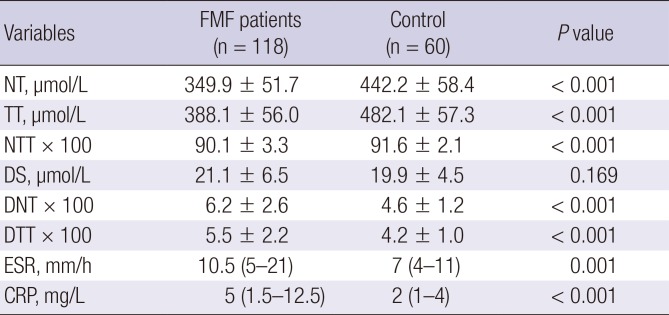
ESR and CRP were given as median (IQR). The others were expressed as mean ± SD. Calculated using Student's t-test for normal distribution or Mann-Whitney U test for non-normal distribution.
FMF = Familial Mediterranean fever, NT = native thiol, TT = total thiol, NTT = native thiol/total thiol, DS = disulfide,DNT = disulfide/native thiol, DTT = disulfide/total thiol,ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, IQR = interquartile range, SD = standard deviation.
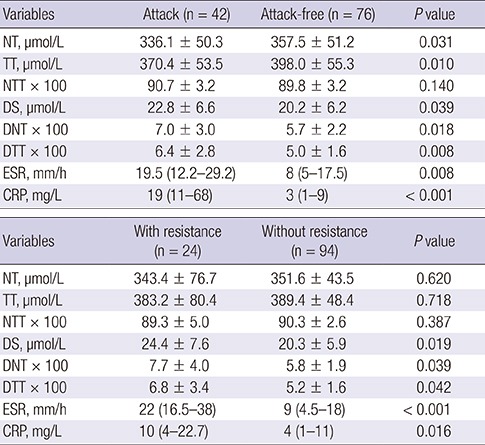
Comparison to FMF-AP, FMF-AFP had lower NT and TT values NT values (336.1 ± 50.3 vs. 357.5 ± 51.2 µmol/L, P = 0.031). Similarly, TT (370.4 ± 53.5 vs. 398.0 ± 55.3 µmol/L, P = 0.010) in FMF-AP were much lower compared to FMF-AFP. DS (22.8 ± 6.6 vs. 20.2 ± 6.2 µmol/L, P = 0.039) DNT (P = 0.018), DTT (P = 0.018), CRP (P < 0.001), and ESR (P < 0.001) values in FMF-AP were significantly higher compared to FMF-AFP (Table 4).
Table 4
Laboratory results of FMF patients in attack period and attack-free period
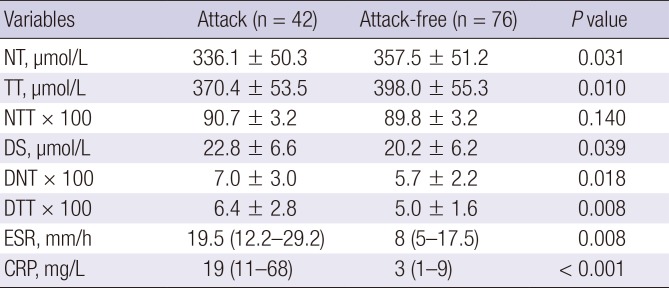
ESR and CRP were given as median (IQR). The others were expressed as mean ± SD. Calculated using Student's t-test for normal distribution or Mann-Whitney U test for non-normal distribution.
FMF = Familial Mediterranean fever, NT = native thiol, TT = total thiol, NTT = native thiol/total thiol, DS = disulfide, DNT = disulfide/native thiol, DTT = disulfide/total thiol,ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, IQR = interquartile range, SD = standard deviation.
Given in Table 5 is a comparison of TT, NT, CRP, ESR, and DS levels in FMF patients according to colchicine resistance. DS (24.4 ± 7.6 vs. 20.3 ± 5.9 µmol/L, P = 0.019), DNT, DTT, CRP, and ESR levels in the colchicine resistance group were found to be significantly higher than in patients without colchicine resistance.
Table 5
Laboratory results of FMF patients with and without colchicine resistance
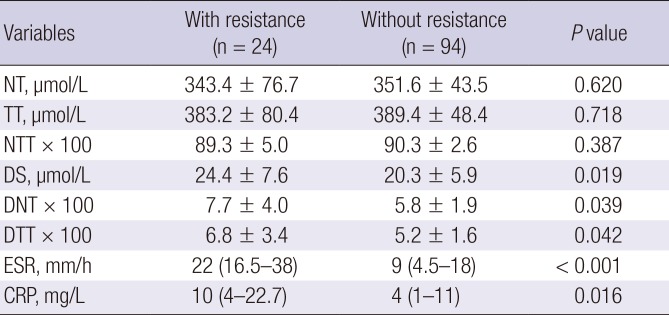
ESR and CRP were given as median (IQR). The others were expressed as mean±SD. Calculated using Student's t-test for normal distribution or Mann-Whitney U test for non-normal distribution.
FMF = Familial Mediterranean fever, NT = native thiol, TT = total thiol, NTT = native thiol/total thiol, DS = disulfide, DNT = disulfide/native thiol, DTT = disulfide/total thiol,ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, IQR = interquartile range, SD = standard deviation.
On correlation analysis, a negative correlation between NT levels and demographic and clinical parameters such as age (r = −0.228, P = 0.002), first symptom age (r = −0.204, P = 0.027), FMF diagnosis age (r = −0.303, P = 0.001), CRP (r = −0.153, P = 0.044), and ESR (r = −0.218, P = 0.004), while a positive correlation between colchicine dose and NT levels (r = 0.232, P = 0.014) were detected. There was a negative correlation between TT and age (r = −0.232, P = 0.002), first symptom age (r = −0.187, P = 0.043), FMF diagnosis age (r = −0.276, P = 0.003), CRP (r = −0.178, P = 0.019), and ESR (r = −0.246, P = 0.001), while there was a positive correlation between TT and colchicine dose (r = 0.205, P = 0.030). There was a positive correlation between DS and CRP (r = 0.153, P = 0.044) and ESR (r = 0.186, P = 0.014).
DISCUSSION
FMF is a chronic autoinflammatory disease with recurrent serositis or arthritis attacks. Colchicine treatment is the standard therapy for avoiding attacks and amyloid deposition in FMF patients. However, a group of patients do not respond well to colchicine therapy (121314). A high level of inflammation is seen during the attack periods of FMF and in some patients there is a persistent chronic subclinical inflammation between attack periods. This persistent chronic inflammation leads to OS and oxidative tissue damage (7). Thiol/disulfide homeostasis has an important role in prevention of oxidative tissue damage. Findings from the present study show that, FMF patients have significantly lower levels of NT and TT than a group of healthy controls. During attack periods, NT and TT levels fall in contrast to rising levels of DS. The DS DNT, and DTT ratios were significantly higher among FMF patients with colchicine resistance than those without resistance. Dosages of colchicine were significantly associated with NT and TT levels.
Thiol groups are sulphur-containing protein compounds with antioxidant properties. They exist in plasma most prominently as bound to albumin and amino acids. A small portion of thiols in plasma contain cysteine, cysteinyl-glycine, glutathione, and methionine. Reactive oxygen radicals formed during OS react with thiols and become oxidized to form DS bonds. The DS bonds formed are reversible, and they can be reduced to thiol groups again. Maintaining the thiol-disulfide balance is essential for antioxidant defense and apoptosis. A thiol-disulfide imbalance can result in the formation of reactive oxygen radicals leading to endothelial dysfunction and apoptosis (2021). The thiol-disulfide balance is found to be altered in chronic conditions such as hypertension, diabetes mellitus, stroke, and hypothyroidism (22232425).
Until recently, the thiol-disulfide balance was measured manually by using the methods described by Erel and Neselioglu (17). This simple and cost efficient method uses a fully automatic method to measure thiol-disulfide balance. Using this new method, Yucel et al. (26) found in their study of pregnant FMF patients that the thiol-disulfide balance is altered in FMF patients compared to healthy controls. Sahin et al. (18) investigated total oxidant capacity and TT level in FMF patients. In this study, TT levels were found to be higher in FMF patients compared to the control group. The authors investigated TT levels only but did not explain the association between these high levels and defensive or compensative mechanisms.
FMF is a chronic inflammatory condition characterized by proinflammatory cytokines including tumor necrosis factor (TNF)-α, IL-1β, and IL-6. These cytokines are intensely released during acute attack periods but persists at a certain level in the absence of attacks as well (2728). An inflammatory status is therefore present in FMF patients during both attack and attack-free periods. Persistent levels of cytokines eventually stimulate apoptosis thus leading to an increase in reactive oxygen radicals. OS is known to occur in FMF patients (2930). Reduced activity of the antioxidant enzyme paraoxonase/arylesterase 1 (PON-1) in FMF patients has been associated with the increased OS (31). Also, increased levels of the macrophage migration inhibitory factor (MIF) in FMF patients is reported to cause increased inflammation and OS (32). Our study found lower levels of NT and TT in FMF patients compared to healthy controls. DS levels of FMF patients were also slightly higher than healthy controls. There was a negative correlation between ESR and CRP and NT and TT. Also, we found that thiol groups decrease as the age of FMF diagnosis increases. Because of reduced thiol levels due to binding of IL-1β thiol to DS bridges, plasma free IL-1β levels may increase and result in increased inflammation (33). According to the results of our study, thiol groups are severely diminished in FMF patients compared to healthy controls. Therefore, FMF patients may experience severe OS damage.
Ediz et al. (34) also reported that OS in FMF patients in attack period is higher compared to patients in the attack-free period. Guzel et al. (35) suggested that thiol groups increase in attack periods. They suggested that thiol groups increase to reduce/prevent oxidative damage. However, their study had only eight patients in acute attack period. On the other hand, the study by Yucel et al. (26) only investigated attack-free pregnant women FMF patients.
On the contrary to previous studies, the current study examines FMF patients in both attack and attack-free periods and also the patients with colchicine resistance are compared to cases without colchicine resistance in detail. In this study, twenty-four of the patients (19.5%) are colchicine resistant and forty-two (34.1%) patients have typical FMF attacks. NT and TT levels decrease while DS levels increase during an acute attack. Again, NT and TT levels were slightly lower in colchicine resistant cases when compared to those without colchicine resistance. DS levels were significantly higher in cases with colchicine resistance. The thiol groups may demonstrate a protective effect against the OS that occurs during an attack. The decrease in TT levels can be explained by the reaction with reactive radicals. As far as we know, there are no studies in the literature that evaluates the relationship between thiol-disulfide balance and colchicine resistance in FMF patients during an attack or attack free period extensively.
Colchicine is a conventional medicine used by FMF patients, and its principal effect is microtubule depolymerization. Colchicine prevents inflammation by blocking migration of neutrophils to the endothelium thus preventing IL-1β release (36). Colchicine has also been proposed as a cardioprotective agent due to its anti-inflammatory effects (37).
Colchicine is known to have an antioxidant effect and to strengthen the antioxidant system. It is reported to interact with thiol groups (38). Colchicine decreases superoxide levels by interfering with the intracellular transport and thereby preventing the assembly of the nicotinamide adenine dinucleotide phosphate (NADPH) oxidase complex responsible for superoxide production (39).
In our study, NT and TT levels were slightly lower in cases with colchicine resistance compared to those without colchicine resistance. DS levels were significantly higher in cases with colchicine resistance. Also, dosages of colchicine were significantly associated with NT and TT levels. Therefore, a fully compliant patient should be given the maximum dose of colchicine that could be achieved with tolerable doses (2 mg of colchicine or more).
Thiol groups may be expended to explain increased inflammation and reactive oxygen radicals in cases with colchicine resistance, and thereby thiol-disulfide balance may be broken for the DS. Solomon et al. (40) suggested that undergoing oxidation and forming DS bonds of thiol groups does not diminish the effect of colchicine. Higher DS levels in cases with colchicine resistance compared to cases without colchicine resistance in our study suggest that, the breaking of thiol-disulfide balance may cause colchicine resistance.
In conclusion, the present study shows that FMF patients experience severe OS, especially in the attack period. Thiol-disulfide homeostasis may have an effect on colchicine resistance.
 XML Download
XML Download