

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recently, various types of rehabilitation robots and virtual reality tools have been introduced in the rehabilitation field, to enhance recovery of the hemiplegic arm (12345). Repetitive training with simple passive range of motion (ROM) exercises have shown little effect on functional recovery; therefore, something more than just passive repetition is required and task-oriented therapies such as activities of daily living training are being emphasized. Recently, rehabilitation robots are being developed to provide integrated treatment methods and induce high motivation (6) as well as intensive treatment dose (7).
Mirror therapy has been conventionally used in rehabilitation, especially for hemineglect symptoms. The effectiveness of mirror therapy in neurorehabilitation was demonstrated in several studies, along with action observation and motor imagery (891011). Mirror therapy is known to activate the sensorimotor cortex and facilitate the brain neuroplasticity; by providing an illusion using a mirror, it makes the subject think as if the paralyzed arm is really moving while the intact arm is moving at the other side of the mirror (9). However, the mirror therapy is not performed widely in the clinical field because the paralyzed arm actually remains unmoving during the treatment period. If the hemiplegic arm also moves in real-time, it would facilitate proprioception that refers to joint position sense or kinesthetic sense. Proprioception is provided in skeletal muscle spindles, Golgi tendon organs, and the fibrous capsules in joints. It is then conveyed to the peripheral nerves, dorsal column-medial lemniscus pathway of the spinal cord, and finally to the sensory cortex of the brain (12). However, to our knowledge, the effect of mirror therapy on proprioception has not been established yet.
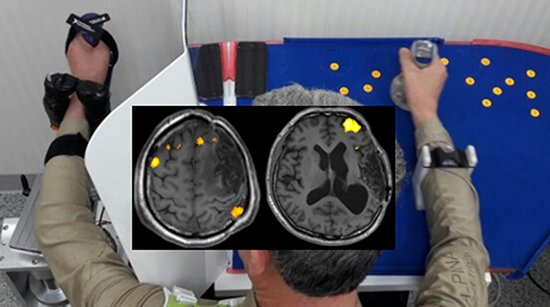
We previously developed a real-time robotic mirror therapy system by adding a 2-axis exoskeleton robot to the hemiplegic side arm (Fig. 1). The purpose of the robotic mirror therapy was to provide proprioceptive stimulus to the sensory cortex, and thus facilitate neuroplasticity and functional recovery of the hemiplegic arm (131415). In this study, we present clinical findings from a clinical case using the robotic mirror therapy system.

MATERIALS AND METHODS
Robotic mirror therapy system
A real-time 2-axis robotic mirror therapy system (Seoul National University Hospital, Seoul, Korea) was used, which was previously developed (16). It is a planar 2-axis upper limb exoskeleton robot consisting of elbow and wrist joints and 3 Attitude and Heading Reference System sensors to measure the movement of the intact limb and actuate the exoskeleton on the paretic arm performing the reflected movements (Fig. 1). This system provides proprioceptive input to the sensory cortex during the mirror therapy using the robot, which conventional mirror therapy does not provide. The robotic mirror therapy consists of 4 tasks, each performed for 5 minutes: ball in holes, soccer game, dot tracing, and moving a cup. The setup and adjustment time of the robotic mirror therapy system is approximately 3 minutes for a normal subject and 4 minutes for a stroke patient. Including the warm-up period, the total treatment time for 1 session is approximately 30 minutes (16).
Validation of the robotic mirror therapy system synchronicity
To validate both synchronicity and the response time simultaneously, an optical motion tracker system (PST Base; PS-Tech, Amsterdam, The Netherlands) was used for capturing the motion of the robot. Optical passive markers with distinctive patterns were devised and trained via motion tracking software in order to differentiate objects recognized by the motion tracker. These markers were attached on the end-effector, wrist joint, wrist restrictor, and elbow joint of the robot system, and corresponding positions on the intact arm side. The optical motion capture system was held directly on top of the robot system for accurate trajectory analysis. Position as well as orientation information of the arm and robot was simultaneously collected via motion capturing software. Random movement was performed and captured for 5 times, at approximately 3 minutes for each movement. The mean angle error regarding both synchronicity and time response simultaneously ranged from 1.97 to 4.59 degrees (Fig. 2).

Clinical treatment settings
Treatment with the planar 2-dimensional robotic mirror therapy system was initiated under a clinical trial on stroke patients (ClinicalTrials.gov Identifier: NCT02878746). Patients were recruited under following criteria: 1) over 18 years old; 2) supratentorial stroke diagnosed between 4 months and 6 years ago; and 3) upper-limb hemiplegia with a score on the Medical Research Council (MRC) scale of grade 2 or less. The main exclusion criteria were as follows: 1) severe spasticity with a score on the modified Ashworth scale (MAS) of grade 3 or more; 2) Mini-Mental State Examination (MMSE) score less than 12; and 3) global or sensory aphasia. The treatment session was provided for 30 minutes per day for 2 weeks.
Clinical evaluation
Clinical functional evaluations were performed before and after 10 sessions of the therapy and at a 2-month follow-up evaluation. The Fugl-Meyer Assessment scale of the upper extremity (FMA-UE) (17), MAS (18), modified Barthel index of the upper extremity (MBI-UE) (1920), Jebsen hand function test (JHFT), hand power measurement, and hemineglect tests (line bisection test and Albert's test) were performed by the same occupational therapist.
To assess proprioception, the thumb finding test (TFT) was performed because of its wide use and reliability (2122). It may be assessed after confirming normal proprioception in the unaffected arm. TFT is performed by the patient touching his or her nose with eyes closed, and the examiner lifts the affected arm to eye level. The patient is then asked to grasp the thumb of the affected hand with the unaffected hand, and this is repeated. The examiner then places a hand over the patient's eyes and raises the patient's affected hand well above the patient's head. The patient is then asked to grasp the thumb as before (22). The TFT score was rated from 0 to 3 points; 0 (no difficulty), able to locate the affected thumb accurately; 1 (slight difficulty), aims in right general direction but missing the affected thumb by less than 3 inches, then able to locate it within 5 seconds; 2 (moderate difficulty), finds the affected arm and climb up the limb to the affected thumb; 3 (severe difficulty), unable to find the thumb and does not climb up to the affected thumb (22).
A functional magnetic resonance imaging (fMRI) study was performed before and after 10 sessions of the robotic therapy according to the protocol in the following section. For comparison, we obtained fMRI data from a normal subject while performing the same tasks as the participant.
Setup for fMRI tasks
The functional imaging consisted of 2 tasks: first, to execute the repetitive passive ROM exercise for dorsiflexion and volar flexion of the hemiplegic wrist joint, and second, to perform active ROM exercise for the same movement and joint. Passive ROM was performed from end to end of possible ROM, and the subject was instructed to perform the movement as best as they can for the active ROM task, since they could not fully perform the designated movement. An fMRI block design was used in both tasks, where 2 rest blocks (each 20 seconds) were interleaved with 1 active block (each 20 seconds). In both tasks, a pair consisting of 1 rest block and 1 active block was repeated 8 times.
For the active wrist of ROM exercise, the participant was thoroughly instructed before entering the scanner. The “start” and “stop” signs were given by the examiner in the scanning room, and compliance with the instructions was ensured by visual inspection throughout the exam. For the passive wrist of ROM exercises, the hemiplegic wrist was manually moved by the examiner's hand during the fMRI acquisition.
fMRI acquisition
The fMRI scans were conducted with a Siemens MAGNETOM Trio, A Tim Syngo scanner (Siemens Healthcare GmbH, Erlangen, Germany) using echo planar imaging (EPI; time of echo [TE] = 30 ms, time of repetition [TR] = 3,000 ms; 9 slices of 3.5 mm thickness, voxel size 1.9 × 1.9 × 3.5 mm3), angulated in parallel to the anterior and posterior commissure line. Whole-brain scans including 8 blocks of executed movements, consisting of 8 EPI alternating with 7 blocks of rest, were recorded per condition. For anatomical reference, an anatomical data set using a T1-weighted magnetization prepared rapid gradient-echo (MP-RAGE) (slice thickness 1 mm, TR = 1,670 ms, TE = 1.89 ms, flip angle = 9°) was obtained in the same session.
fMRI data analysis
The fMRI data were preprocessed using Statistical Parametric Mapping 12 (SPM12; Wellcome Trust Centre for Neuroimaging, London, UK; www.fil.ion.ucl.ac.uk/spm/) implemented in MATLAB 2014b (Mathworks Inc., Natick, MA, USA). This included slice timing, realign, co-register and spatial smoothing (Gaussian kernel of full-width-half-maximum 6 mm). The participant's own magnetic resonance imaging (MRI) scan was used to determine the region of interest (ROI) without normalization to the Montreal Neurological Institute (MNI) template, because the brain contour was impossible to normalize due to partial brain atrophy and ventriculomegaly.
RESULTS
Participant description
A 56-year-old male with underlying hypertension was admitted to a tertiary hospital due to subarachnoid hemorrhage caused by anterior communicating artery aneurysmal rupture. Coil embolization was performed on the same day with initiation of dual antiplatelet therapy. On the next day, vasospasm and infarction with hemorrhage occurred. Brain MRI findings suggested acute right middle cerebral artery infarction. Decompressive craniectomy was performed on the next day, followed by a month of intensive care unit care. After being transferred to general ward, rehabilitation therapy was initiated. He had received continuous and intensive rehabilitation therapy, including physical and occupational therapy for 5 days a week, however, severe left hemiplegia persisted.
At 11 months after stroke onset, he was mentally alert and was able to perform independent single cane gait slowly with ankle-foot-orthosis. The MMSE score was 27 points with slight attention deficit (−3 points). Manual muscle testing (MMT) showed grade 1 for shoulder flexor, grade 2 for elbow flexor, and grade 1 for wrist extensor and finger flexors. Muscle powers in the lower extremities showed grade 3 for hip flexor, grade 2 for knee extensor, and grade 1 for ankle dorsiflexor. Spasticity was minimally present in elbow flexor and wrist flexor, measured as grade 1 on the MAS. Deep tendon reflex was increased for the biceps jerk. Sensory function of left upper extremity was impaired for pain, temperature, and touch, showing 70% compared to the intact side. Proprioception was also moderately impaired, with TFT scored 2 for the eye level and 3 for the overhead level. Albert's test score showed 6/12 on the left side, suggesting presence of left hemispatial neglect. At the time, the patient was enrolled in this study and received the 2-dimensional robotic mirror therapy for 30 minutes per day for 2 weeks (10 sessions). During the 2-week period, he continued on receiving conventional physical and occupational therapy in hospitals 5 days per week on an outpatient basis, which the patient has been receiving for several months. Occupational therapy consisted of passive ROM exercise and functional electrical stimulation.
Clinical evaluation
The results of evaluations performed in the initial period, immediate follow-up after 10 sessions, and 2-months post-treatment follow-up period are shown in Table 1.
Table 1
Functional evaluation before and after the robotic mirror therapy (56-year-old male patient with chronic right middle cerebral artery territory infarction)
At the follow-up functional evaluations after the 10th session, the TFT score of the hemiplegic arm considerably improved. The TFT score at the eye level was improved from 2 to 1, and the TFT score measured at the overhead level from 3 to 1. The Albert's test score on the left side improved from 6 to 11 out of 12. Other parameters revealed no difference before and after robotic mirror therapy. At the 2-month post-therapy follow-up, TFT scores were 1 for both the eye level and overhead level, and the Albert's test score on the left side was 11 out of 12.
fMRI analysis
For the passive ROM task, there were no significant activation areas before the treatment sessions (Fig. 3A). However, after 10 sessions, the lower part of the superior parietal lobule (Brodmann area [BA] 7) and premotor cortex (PMC; biological motion [BM] 6) were significantly co-activated during the passive ROM exercise (P < 0.001, Fig. 3B). Percent signal change of the lower part of superior parietal lobule was 0.10% before robotic mirror therapy, and 0.38% after 10 sessions of therapy. For the active ROM task, the contralateral PMC was mainly activated during the active ROM exercise in the post-treatment fMRI scan (P < 0.001, Fig. 3C and D). Additionally, the left cerebellum was also significantly activated at post-treatment evaluation during both active and passive tasks (P < 0.005, Fig. 3B and D). During the active ROM in the normal subject, the task was performed with his left arm and the right PMC and prefrontal cortex showed significant activation (P < 0.050, Fig. 3E).
Fig. 3
The fMRI study of the patient. The BOLD signal increased in the lower part of the right superior parietal lobule, left PMC, and left cerebellum during the passive left wrist ROM exercise after 10 sessions of robotic mirror therapy (P < 0.005, A: before, B: after). The signal increased mainly in the right prefrontal cortex and left cerebellum during the active ROM exercise after 10 sessions of robotic mirror therapy (P < 0.005, C: before, D: after). The activation pattern during active left wrist ROM in a normal subject is shown (P < 0.050, E). Minimum cluster size for all activations shown is 32 voxels.
fMRI = functional magnetic resonance imaging, BOLD = blood oxygen-level dependent, PMC = premotor cortex, ROM = range of motion.

DISCUSSION
The main concept of the robotic mirror therapy system was to provide proprioceptive input in addition to the conventional mirror therapy by moving the hemiplegic arm with an exoskeleton. Although the evaluation and treatment were done for only one clinical case, the clinical and radiological evaluation results suggested possibilities of enhancing proprioceptive function by using the robotic mirror therapy system. The robotic mirror therapy system used in this study is different from the previous studies of upper extremity robots performing bilateral arm movement with exoskeletons, in that previous robots are not actually using a mirror and cannot induce the illusion, which is a critical component of mirror therapy (2324).
The patient in this study showed improvements in proprioception (measured by TFT) and hemispatial neglect after robotic mirror therapy. Conventional mirror therapy is also known to be effective for hemispatial neglect (825262728), and recently upper limb rehabilitation robot was shown to have beneficial effects on hemispatial neglect (2930). In the fMRI analysis after all treatment sessions, the lower part of the superior parietal lobule and PMC were co-activated during the passive ROM exercise. Because the patient conducted specific tasks with the robotic mirror system for 2 weeks, and fMRI tasks were just simple ROM exercises, we assumed that training effects on the study results could be excluded. The lower part of the superior parietal lobule is known to receive inputs from the somatosensory cortex (12). Receipt of tactile and proprioceptive information from muscles and joints causes the superior parietal lobule to tap into its own memory stores.
On the other hand, the PMC was mainly activated during active ROM exercise at post-treatment, which was probably due to the absence of somatosensory input. Because the patient could not move the hemiplegic wrist on his own due to severe weakness, the active ROM task was actually motor imagery. Previous studies showed the PMC can be activated by motor imagery (2531). The PMC receives rich sensory inputs from the superior parietal lobule, incorporating tactile and visuospatial signals. The PMC is usually active bilaterally, if at all. The patient in our study also showed bilateral activation of PMC; however, it was more dominant on the contralateral side, which is assumed to be because the brain lesion involved part of the PMC on the ipsilateral side.
There have been several studies regarding cerebral activation evoked by the mirror illusion (3233343536). In right-handed healthy volunteers, the primary motor and somatosensory cortex (BA 2, 3b, and 3a), premotor and parietal areas, and V5 area of visual cortex were activated (34). The mirror illusion may be considered not to elicit immediate changes in motor areas, whereas there is a direct effect on somatosensory areas, especially for left-hand movements. In stroke patients, the fMRI results showed significant activation of the ipsilateral sensorimotor cortex, the anterior prefrontal gyrus, and the occipital gyrus due to the mirror visual illusion of ankle movements (35). The ipsilateral prefrontal cortex was also activated during the active ROM task at post-treatment evaluation in our patient. In chronic stroke patients who received mirror therapy for 8 weeks, there was an increase in the laterality index of ipsilesional BA 4 and BA 6 (32). This is somewhat different from our study in that the activation of motor cortex was also increased, and it seems to be due to the difference in residual function of the paretic arm. In their study, the mean Fugl-Meyer Assessment (FMA) score of the upper extremity was initially 18.9 and 35.6 at 6-month follow-up, whereas the patient in our case could not actually move the wrist at all. The improvement in upper extremity function would have led to increase of blood oxygen-level dependent (BOLD) signal in BA 4. There was also significant activation of the left cerebellum during the active and passive tasks in our case. The role of the cerebellum during the stroke rehabilitation is still unclear; however, it is suggested that the activation of the ipsilateral or contralateral cerebellum may be related to motor learning or cerebello-cortical network (32). In comparison with the normal subject, the pattern of increased signal in the PMC and prefrontal cortex was similar during the active ROM task, whereas there was no significant activation at the cerebellum.
In our study, the proprioception was improved, particularly when compared to other sensory modalities. This may be related to the robotic therapy setting. When the patient put on the exoskeleton, the forearm and hand were fixed with the strap throughout the treatment. Therefore, the tactile sensory input would have been nearly constant without significant variation. However, the most noticeable sensory change during the robotic mirror therapy was the movement of the elbow and wrist joint, which is a proprioceptive stimulation. Before the analysis, we expected to find increased activity in both the somatosensory cortex and the superior parietal lobule, but the dominant change was only seen in the superior parietal lobule. The reason for this result may have been clearer if we had performed the somatosensory evoked potential (SEP) examination. We need to further differentiate the contribution of the robotic mirror therapy to sensorimotor processing from that of tactile stimulation or simple passive ROM exercise.
The mirror effect may degrade proprioceptive information rather than integrate visual and proprioceptive information concerning hand position (37). The magnitude of this effect is linearly related to the size of the visual-proprioceptive conflict (3738). In this aspect, robotic mirror therapy in our study can contribute to visual-proprioceptive integration. Therefore, it is expected to trigger a synergistic effect in terms of proprioception, compared to simple passive ROM exercise alone without mirror therapy.
There are several limitations in this study. First, we performed the robotic mirror therapy with fMRI evaluation for only one case, so it is difficult to generalize the results. Due to our clinical environment and patient population in our hospital, it was difficult to find suitable candidates for this clinical study. There were not enough patients with severe motor impairment and relatively mild cognitive impairments during the study period. However, this study showed that the robotic mirror therapy system could be an option for recovery of proprioception in stroke patients in the future. Further investigation should be performed on a sufficient number of patients. Second, the patient was in the chronic stage and the residual motor function of the hemiplegic arm was too small (MRC grade 1). Therefore, the capacity for recovery of motor power may have been too small. Application of the robotic mirror therapy should be considered for subacute patient to maximize the recovery of motor function as well as proprioception. Third, proprioception was only assessed by TFT. Objective assessment using quantitative sensory test device may have better evaluated the proprioceptive function. Further clinical study should include such quantitative tests.
This study integrating mirror therapy and robotic rehabilitation demonstrated acceptable validity and improvements in evaluations regarding proprioception and hemineglect. Thus, the robotic mirror therapy system may serve as a useful treatment method for supratentorial stroke patients to facilitate recovery of proprioceptive deficit and hemineglect symptoms.
 XML Download
XML Download