

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ionizing radiation is an effective treatment modality for medulloblastoma, the most common malignant brain tumor in children. Medulloblastoma is sensitive to ionizing radiation; therefore, radiotherapy with chemotherapy following surgical removal of the tumor has been established as the standard treatment. However, it is well known that cranial radiation causes various late complications, including endocrine abnormalities (1), and even rare but life-threatening diseases, such as secondary tumors (2) and vasculopathy (3).
Several types of radiation-induced tumors have been reported in pediatric patients. Meningioma, the second most common radiation-induced tumor in children (2), can develop even after low dose radiation and have distinct characteristics from those of primary meningioma (4). Radiation-induced vasculopathy can appear as moyamoya syndrome characterized by bilateral stenosis of distal parts of internal carotid arteries and formation of abnormal collateral vessels. Moyamoya syndrome is the risk factor for ischemic stroke in children, which can cause prolonged sequelae.
Here, we describe the first case of radiation-induced tumor and radiation-induced moyamoya syndrome that developed in one patient after radiotherapy for medulloblastoma. We emphasize the importance of surveillance of late complications of radiotherapy, especially in pediatric patients.
CASE DESCRIPTION
Initial presentation, operation, and adjuvant therapy
The 3-year-old boy was referred to our hospital in June 2004. He presented with headaches and vomiting for 2 weeks and generalized tonic clonic seizure shortly prior to admission. Magnetic resonance imaging (MRI) showed a contrast-enhancing lesion in the posterior fossa causing hydrocephalus (Fig. 1A) and leptomeningeal enhancement around the spinal cord (Fig. 1B). There was no evidence of cerebral vasculopathy at that time. A midline sub-occipital craniotomy and gross total resection of the main mass was performed in June 2004. The tumor was diagnosed as a medulloblastoma by pathologic examination. Three weeks after surgery, a ventriculoperitoneal shunt was installed in the right lateral ventricle to manage the hydrocephalus.
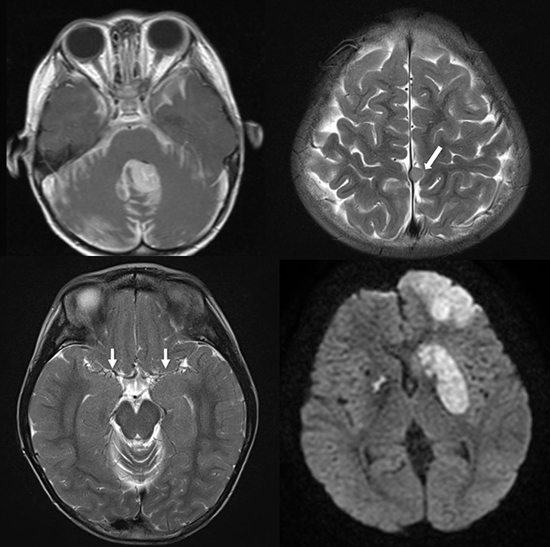
 | Fig. 1Initial presentation: medulloblastoma. Axial (A) and sagittal (B) contrast-enhanced MRI show a strongly enhancing lesion in the cerebellum with surrounding leptomeningeal enhancement, suggesting leptomeningeal seeding. Second presentation: meningioma. A 9 × 7 mm round shape mass (arrow) based on the falx cerebri at the high vertex with peripheral enhancement is shown in axial T2 weighted (C), contrast-enhanced sagittal (D).
MRI = magnetic resonance imaging.
|
One month after the tumor resection, he underwent craniospinal irradiation with a dose of 30.6 Gy followed by a focal boost to the posterior fossa of 19.8 Gy. One month later, he received eight-in-one chemotherapy, including methylprednisolone, vincristine, lomustine, cisplatin, hydroxyruea, procarbazine, cyclophosphamide, and cytosine arabinoside. Due to aggravation of spinal seeding after two courses of the regimen, the chemo-regimen was changed to a composition of carboplatin, cyclophosphamide, vincristine, and etoposide for 9 courses. This was followed by 16 courses of carboplatin, cyclophosphamide, and etoposide and 22 courses of irinotecan, cisplatin and etoposide. Since the chemotherapy was completed in April 2008, he had been routinely followed-up with MRI of the brain and spine without evidence of recurrence until February 2014.
Second presentation, operation, and adjuvant therapy
In February 2014, at 13 years of age, follow-up MRI revealed a new well-enhancing 9 × 7 mm round mass based on the falx cerebri at the high vertex (Fig. 1C and 1D). To rule out tumor seeding of medulloblastoma, a craniotomy and tumor removal was performed in March 2014. During the surgery, the arterial partial pressure of carbon dioxide ranged from 31 to 34 mmHg on arterial blood gas analysis and end-tidal carbon dioxide monitoring. Histopathological examination of the lesion confirmed a diagnosis of meningioma, and it was considered to be a secondary tumor caused by radiation therapy 10 years previously.
On postoperative day 5, the patient complained of right-sided motor weakness, motor dysphasia, dysarthria, and dysphagia. Diffusion MRI demonstrated acute infarction in the left frontal lobe and both basal ganglia (Fig. 2A). Retrospective review of MRI revealed bilateral steno-occlusion of the bifurcation of internal carotid arteries since July 2011 (Fig. 2B). Without any clinical suspicion for cerebral ischemia, the vasculopathies were overlooked at the time of imaging. Magnetic resonance angiography (MRA) showed marked narrowing of the main trunk of both middle cerebral arteries with preserved portions of the branches (Fig. 2C). Perfusion MRI showed delayed time to peak in the both middle cerebral artery and anterior cerebral artery territories. Conventional cerebral angiography confirmed occlusion at the terminal portion of both internal carotid arteries (Fig. 2D). In addition, focal transdural collaterals from the right external carotid artery to the right frontal lobe via the right middle meningeal artery and diffuse leptomeningeal collaterals from vertebral arteries were detected. These radiologic findings were consistent with moyamoya syndrome.
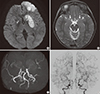 | Fig. 2Acute brain infarction after removal of the radiation-induced tumor. Axial diffusion weighted images (A) show diffusion restriction at the left frontal lobe and both basal ganglia, which indicates acute infarction. Retrospective review of MRI shows bilateral steno-occlusion of the internal carotid artery bifurcation and its branches (arrows) on T2-weighted axial image (B). MRA reveals marked narrowing of the main trunk of both middle cerebral arteries with rather preserved portions of their distal branches (C). Conventional cerebral angiography (D) shows steno-occlusion at the terminal portion of the right internal carotid artery and left internal carotid artery confirming moyamoya syndrome.
MRI = magnetic resonance imaging, MRA = magnetic resonance angiography.
|
After medical treatment and rehabilitation, he showed improvement of motor power and gradually regained control of speech and swallowing. Although perfusion status of left cerebral territory was poor, we decided to delay the surgical intervention for moyamoya syndrome until recurrent ischemic symptoms are present.
Third presentation, operation, and adjuvant therapy
Four months after the second surgery, the patient suffered from analgesics-unresponsive severe headaches associated with dysarthria and dizziness. The frequency of the headaches over the two months increased to 3 to 4 days per week. MRI showed progressed chronic change of previously noted infarction at left frontal lobe and bilateral basal ganglia (Fig. 3A). Perfusion MRI demonstrated decreased perfusion in the middle cerebral artery territories bilaterally and aggravated perfusion in the left anterior cerebral artery territory (Fig. 3B). To resolve the ischemic symptoms, left superficial temporal artery endocephlo-duro-arterio-synangiosis (EDAS) with frontal burr hole encephalo-galeo-periosteal-synangiosis (EGPS) was performed in November 2014.
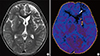 | Fig. 3Third presentation: moyamoya syndrome. T2-weighted axial image shows chronic change of infarction at the left frontal lobe (arrows) and bilateral basal ganglia (A). Perfusion MRI demonstrates delayed time to peak in the both middle cerebral artery territories and aggravated perfusion in the left anterior cerebral artery territory (arrows) (B).
MRI = magnetic resonance imaging.
|
On postoperative day 1, the patient developed right side weakness, right facial palsy, and decreased verbal output. Brain computed tomography (CT) images showed epidural hemorrhage under parietal bone flap and parenchymal swelling in left parietal lobe. There was no sign of acute infarction on diffusion weighted MRI. After conservative therapy, he fully regained pre-operative performance status and was discharged. The severity of headache gradually decreased after the bypass surgery. He has been free from headaches since one month after surgery.
Two months after the surgery for moyamoya syndrome, the patient presented with a wound dehiscence resulting in exposure of the skull. His physical, laboratory examination, and culture from wound tissue revealed no signs of local or systemic infection. Wound was irrigated with normal saline solution and sutured primarily. Five days after, the patient was discharged without complication.
Pathologic findings
The first cerebellar tumor was composed of sheets of small round cells with high nucleo-cytoplasmic ratio and prominent nucleoli. There were numerous apoptotic nuclei. Light microscopy features were consistent with large cell type medulloblastoma. Immunohistochemically, the tumor cells were positive for CD56, synpatophysin and p53, and the Ki-67 labeling index was high (positive in 40%).
The second tumor at the falx cerebri had completely different pathologic features. It showed sheets of ovoid to elongated neoplastic cells with long cytoplasmic processes. It expressed E-cadherin, but not epithelial membrane antigen. Mitosis was scarce (< 1/10 HPF), and the Ki-67 labeling index was 4.26%. The second tumor was diagnosed as a transitional type meningioma, which is World Health Organization (WHO) grade I. Electron microscopy of the second tumor revealed sheets of oval to elongated tumor cells with Jigsaw puzzle-like interlocking cytoplasmic processes. The cytoplasm had abundant wavy intermediate filaments, and the cytoplasmic processes were joined by well-developed desmosomes; these findings were also consistent with meningioma. There was no evidence of recurrence of medulloblastoma.
DISCUSSION
Radiation-induced tumors are among the most fatal long-term complications of radiotherapy against brain tumors. Cahan et al. (5) suggested four criteria for defining a radiation-induced tumor. First, the tumor must be located in the previously irradiated region where there was no evidence of tumor prior to irradiation. Second, there must be sufficient latency time, generally several years, from irradiation to induction of tumor. Third, the tumor must have distinct histologic characteristics from the primary tumor. Forth, a patient must have no genetic predisposing factor that could contribute to tumor occurrence. In our case, meningioma occurring after radiotherapy against medulloblastoma fulfills all of these criteria.
Meningioma induced by cranial irradiation has clinically unique characteristics from primary meningioma. Compared to primary meningioma, it occurs at a younger age, is more aggressive and has a higher rate of recurrence and multiplicity (4). The latency period tends to be shorter when exposed to higher doses of radiation at a younger age (6). In the present case, the patient was exposed to a high dose of radiation (>10 Gy) at the young age of 3 years.
Radiation-induced cerebral vasculopathy, such as arterial occlusion, moyamoya syndrome, aneurysm formation, cerebral hemorrhage, necrosis, and stroke, is also a well-known late adverse effect of cranial irradiation (3). The effect of ionizing radiation on cerebral vessels has been widely studied. The vascular changes in response to radiation have characteristic pathologic features, including myointimal proliferation, intimal accumulation of foam cells, and luminal occlusion by connective tissue (7). In the present case, the vascular changes occurred 83 months after completion of radiation. However, the latency interval between radiation and vasculopathy may vary from several months to years compared to radiation-induced tumor development.
Moyamoya syndrome is characterized by the stenosis of the terminal portion of bilateral internal carotid arteries and the formation of abnormal vascular-net structure at the base of brain (8). It is referred to as a moyamoya disease when these features occur without known cause, and it is referred to as moyamoya syndrome when there are predisposing factors, such as neurofibromatosis type 1, cranial therapeutic radiation, Down's syndrome, and hemoglobinopathy (8). Desai et al. (9) reviewed 54 cases of radiation-induced moyamoya syndrome from 1967 to 2002. In the review, the majority of primary tumors was located in the parasellar region and were classified as optic glioma, craniopharyngioma, and pituitary adenoma. The occurrence of moyamoya syndrome after treatment of medulloblastoma is very rare because medulloblastoma is usually located in the infratentorial region, far from the circle of Willis, where moyamoya syndrome occurs. Including the present patient, there are 4 reported cases (101112) of radiation-induced moyamoya syndrome that developed after radiotherapy against medulloblastoma (Table 1).
Table 1
Reported cases of radiation-induced moyamoya syndrome developed after radiation therapy for medulloblastoma

| Author | Year | Age, sex | Dose of radiation | Latency | Occluded vessel | Symptoms |
|---|---|---|---|---|---|---|
| al-Amro and Schultz (10) | 1995 | 7, M | 34 Gy whole brain | 4 mon | Bilateral distal ICA and VA | Hemiparesis |
| 20 Gy posterior fossa | ||||||
| 25.5 Gy spine | ||||||
| Ullrich et al. (11) | 2007 | 2, M | 39.6 Gy* | 55 mon | Not described | Hemiparesis |
| Kim et al. (12) | 2011 | 5, F | 36 Gy craniospinal axis | 2 yr | Right supraclinoid ICA and left ICA | Hemiparesis |
| 18 Gy posterior fossa | ||||||
| Present case | 3, M | 30.6 Gy craniospinal axis | 10 yr | Bilateral distal ICA | Hemiparesis | |
| 19.8 Gy posterior fossa |
M = male, F = female, ICA = internal carotid artery, VA = vertebral artery.
*Calculated dose of radiation on the circle of Willis.
![]()
The coexistence of radiation-induced tumor and vasculopathy has been rarely reported (131415161718). Eight cases, including the present case, are summarized in Table 2. In most cases, the secondary tumors were meningiomas, except for one case of high-grade glioma, and the associated vasculopathy was predominantly cavernoma and occlusive vasculopathy. The radiation doses ranged from 18 to 54 Gy, and all patients received radiotherapy during childhood (2–12 years). Except for one case of symptomatic hemorrhage of carvernoma, radiation induced vasculopathy coexisting with secondary tumor was asymptomatic and detected during pre- or post-operative workup for secondary tumor. Therefore, we should consider the possibility of radiation induced vasculopathy when we face secondary tumor.
Table 2
Reported cases of coexistence of radiation-induced tumor and vasculopathy after cranial radiotherapy

| Author | Year | Age, sex | Dose of radiation | Primary tumor (location) | Secondary tumor (location) | Latency, yr* | Vasculopathy; affected vessel | Latency, yr† | Secondary symptom |
|---|---|---|---|---|---|---|---|---|---|
| Montanera et al. (13) | 1985 | 9, M | 52.5 Gy brain | Ganglioglioma (left temporal) | Meningioma (left frontoparietal) | 15 | Occlusion of the left ICA | 15 | Seizure |
| 12, F | 45 Gy brain | Astrocytoma (suprasellar) | Meningioma (left temporoparietal) | 20 | Occlusion of the left ICA at ophthalmic branch | 20 | Visual loss | ||
| Foreman et al. (14) | 1995 | 2, M | 20 Gy brain | ALL | Meningioma (right frontal) | 19 | Occlusion of left ACA, PCA (occlusion of right ICA‡) | 19 | Hemiparesis |
| Kamide et al. (15) | 2010 | 5, M | 15 Gy brain | Medulloblastoma (cerebellum) | High grade glioma (cerebellum), probable meningioma without pathology (left frontal, temporal) | 29 | Cavernoma (right temporal) | 7 | 1) Symptomatic hemorrhage (cavernoma) |
| 39 Gy posterior fossa | 2) Truncal ataxia (glioma) | ||||||||
| Baheti et al. (17) | 2010 | 9, M | 18 Gy brain | ALL | Meningioma (right frontal) | 21 | Cavernoma (pons) | 21 | Seizure |
| Paramanathan et al. (18) | 2010 | 5, F | 54 Gy brain | Ependymoma (left frontoparietal) | Meningioma (orbital) | 16 | Cavernoma (left cerebellar and bilateral basal ganglia) | 16 | Ptosis |
| Chourmouzi et al. (16) | 2013 | 10, M | ND | Medulloblastoma (cerebellum) | Meningioma (right frontal) | 19 | Cavernoma (left centrum semiovale and right temporal) | 19 | Seizure |
| Present case | 3, M | 30.6 Gy craniospinal axis | Medulloblastoma (cerebellum) | Meningioma (falx) | 10 | Moyamoya syndrome; bilateral occlusion of distal ICA | 10 | Hemiparesis | |
| 19.8 Gy posterior fossa |
M = male, F = female, ALL = acute lymphoblastic leukemia, ICA = internal carotid artery, ACA = anterior cerebral artery, PCA = posterior cerebral artery, ND = not described.
*Latency of radiation-induced tumor. †Latency of radiation-induced vasculopathy. ‡Possibly due to tumor compression.
![]()
When a secondary tumor is found after cranial irradiation at a young age, preoperative radiologic imaging examination for radiation-induced vasculopathy is recommended. Although cerebral angiography is the gold standard for diagnosis of moyamoya syndrome, MR images are good diagnostic measure for monitoring the development of moyamoya syndrome in patients who had been previously treated with ionizing radiation. If there are any MRI findings compatible with moyamoya syndrome, then cerebral angiography should be included in the pre-operative workup.
Timing for surgical intervention of moyamoya syndrome when accompanied with secondary tumor is an important issue. Due to lack of data to guide the management, decisions have been made case by case. We recommend it should be decided based on the presence of symptoms and cerebral perfusion status. When patient is asymptomatic and collateral circulation is well developed, revascularization surgery can be postponed to after the tumor removal. On the other hand, active revascularization surgery should be considered first in patients with ischemic symptoms, poor cerebral perfusion reserve or when significant injury of collateral vasculature is expected during tumor resection.
When we perform surgery on radiation-induced tumor in patients with moyamoya syndrome, special attention on cerebral hemodynamics and collateral circulation is needed to prevent cerebral ischemic injury. For example, the arterial partial pressure of carbon dioxide should be maintained at a normal level during surgery to prevent a decrease in cerebral blood flow (19). In the present case, carbon dioxide level was controlled in low level to reduce blood loss as usually done in brain tumor resection surgery and we think that vasoconstriction triggered by hypocapnea may contribute to acute cerebral infarction. Moreover, vascular structure such as collateral circulation should be carefully evaluated and not to be injured during tumor removal surgery.
Another issue which should be considered when performing EDAS for radiation induced moyamoya syndrome is wound dehiscence as shown in the present case. Surgical procedure, radiotherapy and young age, all are risk factors for postoperative wound problems in moyamoya syndrome. During EDAS, galeal aponeurosis is detached with a scalp artery and transported onto the surface of the brain so galeal defects are unavoidable. Radiotherapy reduces wound healing capability of affected tissue by damaging the fibroblasts and reducing vascularity (20). The thinness of children's scalp is also thought to increase the possibility of wound dehiscence. Careful closure of surgical wound and conditional delaying of the timing of stich out is recommended.
In conclusion, this case emphasizes on the importance of monitoring of several delayed side effects after cranial radiotherapy. Careful evaluation is recommended for cerebral vasculature along with other late complications such as secondary tumor, especially when cerebral intervention is planned.
 XML Download
XML Download