

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary pericardial malignant mesothelioma (PPM) has an extremely low incidence about 0.002% in the literatures (1). Malignant mesothelioma is a malignancy arising mesothelial surface of pleural cavity, or rarely pericardium (2). The diagnosis and the novel treatment of PPM are usually delayed, due to its nonspecific clinical manifestations such as fatigue, general weakness and dyspnea. The treatment options are limited, and the standard treatment has not been well established yet. So the prognosis is naturally poor with a short overall survival below six months. We report a case of old woman who diagnosed PPM with cardiac tamponade and provide a literature review of 23 cases from 2009 through April 2016.
CASE DESCRIPTION
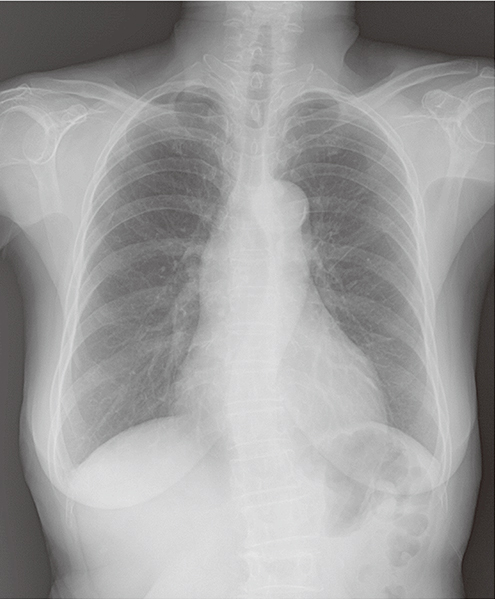
A 71-year-old woman who suffered from dyspnea and dizziness for one year and a 3-kilogram weight loss, about 6% of body weight, during a month was admitted via outpatient clinic of familial medicine in September 2014. Chest radiography showed no pathologic finding (Fig. 1A). But, her chest computed tomography (CT) revealed a pericardial effusion without definite pericardial thickening (Fig. 1B). An echocardiography showed mild to moderate pleural effusion (posterior depth = 5.7 mm and anterior depth = 10.2 mm in the subcostal window) (Fig. 1C). She had never smoked, and no history of occupational or incidental exposure to asbestos. There was not an indirect exposure of asbestos from her husband. Unfortunately, no further invasive evaluation was done such as pericardiocentesis at that time. There was a little change of these symptoms during the follow-up period. In August 2015, the patient was referred to cardiology for managing pericardial effusion. The physical examination on admission showed signs of pericardial tamponade. Initial vital signs were a blood pressure of 95/80 mmHg, a heart rate of 116 beats per minute, a respiratory rate of 22 breaths per minute, a body temperature of 36.7°C, and an oxygen saturation of 98% in room air. In electrocardiogram, low voltage QRS was observed. Chest radiography showed marked cardiomegaly (Fig. 2A). Echocardiography demonstrated a large amount pericardial effusion (posterior depth = 22.5 mm and anterior depth = 46.6 mm in the subcostal window) (Fig. 2C). Emergency pericardiocentesis was done. The total amount of removed pericardial fluid was over 2,300 mL. This fluid was bloody and exudate. Protein of pericardial fluid was 2.3 g/dL and lactate dehydrogenase (LDH) was 165 IU/L. The acid-fast bacilli (AFB) stain of pericardial fluid showed no AFB. Pericardial fluid cytology was negative for malignancy. Chest CT and F-18 fluorodeoxyglucose positron emission tomography (FDG-PET) showed a huge hypermetabolic mass which sized about 8 × 5 cm in pericardium (Fig. 2B and 2D). The patient underwent excisional biopsy of pericardium for diagnosis. Histopathological evaluation of the pericardial tissue revealed malignant mesothelioma. Immunohistochemical stains were positive for calretinin, cytokeratin (CK 5/6, CK 7) and vimentin (Fig. 3) but, negative for thyroid transcription factor 1 (TTF-1). Based on the results, PPM was diagnosed. The consultation to cardiothoracic surgeon concluded that, the tumor was inoperable because of its location and size. Despite her advanced age, she decided to receive palliative chemotherapy. After 7 cycles of palliative chemotherapy with pemetrexed and cisplatin during 6 months, the disease has maintained stable disease status. However, her performance status deteriorated gradually, and she was unable to receive more palliative chemotherapy. Finally, we decided to discontinue the chemotherapy and keep supportive care only. Until now, she is still alive with best supportive care, 20 months after first clinical manifestation.
 | Fig.1Initial imaging studies of first admission. (A) Chest radiography showed no cardiomegaly. (B) Chest CT showed a moderate amount of pericardial effusion. (C) TTE demonstrated a normal cardiac contractile force (60%–65%) and a moderate amount of pericardial effusion.
CT = computed tomography, TTE = transthoracic echocardiography.
|
 | Fig. 2Follow-up imaging studies of second admission diagnosed with PPM. (A) Chest radiography showed a severe cardiomegaly. (B) Chest CT showed a huge mediastinal mass that bordered by ascending aorta, SVC and right pulmonary artery. (C) TTE demonstrated a normal cardiac contractile force (55%–60%) and a large amount of pericardial effusion. (D) PET revealed a mass showing an abnormal hypermetabolism in the mediastinum.
PPM = primary pericarcial malignant mesothelioma, SVC = superior vena cava, CT = computed tomography, TTE = transthoracic echocardiography, PET = positron emission tomography.
|

DISCUSSION
Malignant mesothelioma arises from the mesothelial cells in cavities as pleural cavity, peritoneum, pericardium and the testicles (3). PPM is a rare type of mesothelioma which approximately 1% of all mesotheliomas (14). The pericardial and peritoneal malignant mesothelioma (median, 5–7 months) have worse prognosis than pleural malignant mesothelioma (median, 8–10 months) (5). One cause of poor prognosis is late diagnosis due to long latent period between onset and symptoms and nonspecific clinical manifestation. Only 25% of 200 cases of PPM have been diagnosed antemortem. Moreover, the cause of PPM remains uncertain, unlike that of pleural mesothelioma which has strong association with asbestos exposure (6). Other cause of poor prognosis of pericardial mesothelioma is a few treatment options including surgery, radiation, and chemotherapy. None of these approaches can bring a survival benefit (7).
In the present case, she did not receive a diagnosis of PPM until cardiac tamponade was developed. Although pericardial effusion was discovered one year ago, PPM has not been considered as a diagnosis due to no pericardial thickening. However, we carefully suggest that pericardiocentesis and close observation if it cannot aspirate, must be considered for the patients with an unexplained pericardial effusion to prevent delay in diagnosis. Furthermore, the diagnostic sensitivity of cytology is low as only 20% (8). The best choice of treatment was palliative chemotherapy with pemetrexed and cisplatin that mainstay of chemotherapy in malignant pleural mesothelioma (9). Although the standard treatment option of PPM is not established yet, randomized trials have now confirmed that combining pemetrexed with platinum-based chemotherapy confers a survival benefit comparing platinum monotherapy in pleural malignant mesothelioma (10). In this case, despite of her age and performance, she still alive with stable disease beyond expectation.
In order to update the available knowledge concerning its clinical, pathological features, especially treatment outcomes, we reviewed 22 literature citations of 24 cases in which a diagnosis of PPM was made. This review includes the citations published from 2009 to April 2016, because the last extensive review of the entity was undertaken in 2009 when pemetrexed just started being used in pleural mesothelioma (8). The findings of this review, combined with our case, are summarized in Table 1. The sex distribution is even (male:female = 14:10) and the median age is 60.5 (range, 27–85). Only 3 cases with known exposure to asbestos are reported (12.5% in total 24 cases) that imply no obvious relationship between asbestos exposure and the development of PPM. The results of cytological study have a decisive effect in only 5 cases with low sensitivity of 20.8% that corresponds to previous reviews (8). Epithelial, biphasic, and sarcomatoid patterns were reported in 12, 5, and 6 cases, respectively. Eleven patients were given any treatment option, 8 received with pemetrexed containing regimen among them. Survival distribution of the patients, except 2 cases without survival information, from the time when the first symptoms appeared is illustrated in Fig. 4. Four patients were alive when the article was published. Although some patients with sarcomatoid disease had dismal prognosis, the median survival time from symptoms in whole cases of this review is 8 months that is longer than many earlier studies prior to introducing pemetrexed-cisplatin chemotherapy (1). Especially, most of whom had a chance receiving chemotherapy lived much longer than others (median, 27 vs. 1.5 months; P = 0.003). Most of them were pemetrexed-containing regimens. As malignant pleural mesothelioma, pemetrexed, and cisplatin chemotherapy might also bring a clinical benefit to PPM.
Table 1
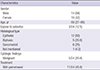
Values are presented as median (range) or number (%).
PPM = primary pericarcial malignant mesothelioma.
![]()

In conclusion, PPM is a very rare disease but it must be considered in patients who have unexplained massive pericardial effusion. Furthermore, chemotherapy with pemetrexed and platinum could be considered as a PPM treatment option.
 XML Download
XML Download