

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatitis B virus (HBV) is a leading cause of chronic hepatitis, cirrhosis, and hepatocellular carcinoma worldwide (1). Antiviral drug use is considered for chronic HBV infection treatment to prevent its serious sequelae. HBV is a deoxyribonucleic acid (DNA) virus. HBV replication relies on reverse transcription, which is similar to that of the human immunodeficiency virus (HIV) (1). Because of these characteristics, the majority of antiviral drugs are nucleoside and nucleotide analogs that interfere with viral replication by inhibiting viral DNA polymerase (1). However, their therapeutic effects are limited owing to drug resistance, relapse after treatment cessation, and possible toxicity (2). Mitochondrial cytotoxicity is a well-known side effect of nucleoside analogs. Thus, newer L-nucleoside analogs with no significant mitochondrial toxicity were introduced.
Clevudine (Revovir, 1-[2-deoxy-2-fluoro-b-Larabinofuranosyl] thyminine, L-FMAU) which is an L-nucleoside analog for HBV was approved in Korea after a 24-week clinical trial with safety on mitochondrial structure, DNA content, or function (34). The advantage of clevudine is prolonged viral replication suppression even after withdrawal of treatment (34). Clevudine was approved in the Philippines and Korea, with incomplete licensing in Indonesia, Thailand, India, and Malaysia for the treatment of hepatitis B treatment (5).
In contrast to the clinical trial, several recent studies have reported myopathy associated with mitochondrial toxicity during clevudine therapy (678). We also experienced seven patients with myopathy during clevudine therapy. Therefore, we collected and summarized the reported cases, including our cases, to characterize the clinical features and laboratory findings of clevudine-induced myopathy for early detection.
Go to : 
MATERIALS AND METHODS
We conducted a PubMed and KoreaMed database search. Nighty-five cases of patients with clevudine myopathy, including our seven cases, were collected for the analysis (678910111213). Our seven patients were recruited from January 2006 to June 2015 at two university hospitals. This retrospective study was approved by the local Human Research Protection Office/Institutional Review.
We assessed age, sex, clinical features, clevudine therapy duration before symptom onset, daily clevudine dose, and recovery time. Recovery time was defined as the duration between discontinuation of clevudine and improvement to normal muscle power. Muscle power was graded using the Medical Research Council (MRC) scale. Bulbar symptoms or neck muscle weakness was also evaluated. Laboratory tests, including liver and renal function tests and creatine kinase (CK) levels, and available results of electrophysiological studies and muscle biopsies were analyzed.
Data were analyzed using the SPSS 20.0 (SPSS Inc., Chicago, IL, USA). Results were expressed as the mean with standard error or median with ranges. Univariate analysis was performed using Student's t-test for continuous variables, and χ2 and Fisher exact tests were used for categorical variables and correlation analysis. P < 0.05 was considered as significant.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Dongguk University Ilsan Hospital (registration No. 2016-116). Informed consent was submitted by all subjects when they were enrolled.
Go to :
RESULTS
The clinical characteristics of 95 patients are presented in Table 1. The patients comprised 52 women and 43 men, aged 48.9 ± 9.1 years (range: 27–76 years). All patients were administered clevudine therapy (30 mg/day) for the treatment of chronic hepatitis B. The concurrently prescribed medications in the patients previously reported were not identified but all of our seven patients did not use drugs such as statins that could cause myopathy. The patients were treated with clevudine for 14.2 ± 3.9 months (range: 5–24 months) before the development of symptoms. Weakness gradually progressing to nadir took 8.6 ± 7.5 months in our seven patients. The common presenting symptom was extremity weakness. Weakness involved the lower and upper extremities in 98.9% and 75.9% of the patients, respectively. In addition, lower extremity weakness was more severe in the proximal part (mean MRC grade: 3.7) than the distal part (mean MRC grade: 4.3, P < 0.001). Upper extremity weakness was also more severe in the proximal part (mean MRC grade: 4.5) than the distal part (mean MRC grade: 4.8, P < 0.001). Bulbar and neck weakness were found in 13 patients (13.7%), with no ocular muscle involvement. Myalgia was sometimes accompanied with progressive weakness (Table 1).
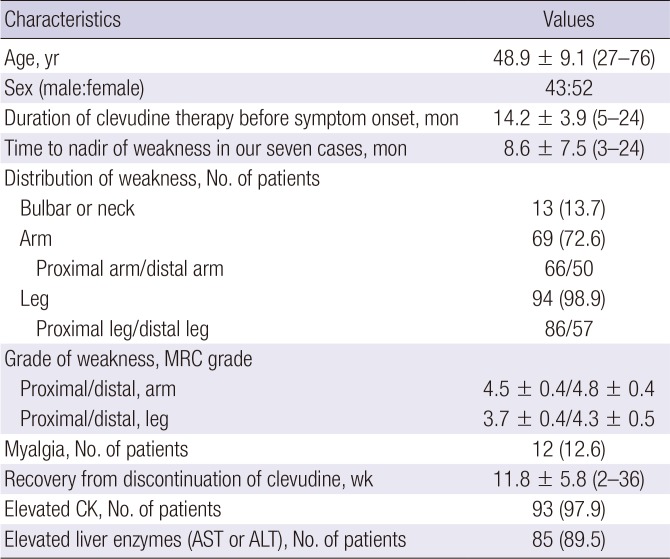
Table 1
Summary of demographic, clinical features, and laboratory findings of the patients
Values are presented as mean ± standard deviation (range) or number (%).
MRC = Medical Research Council, CK = creatine kinase, AST = aspartate aminotransferase, ALT = alanine aminotransferase.
![]()
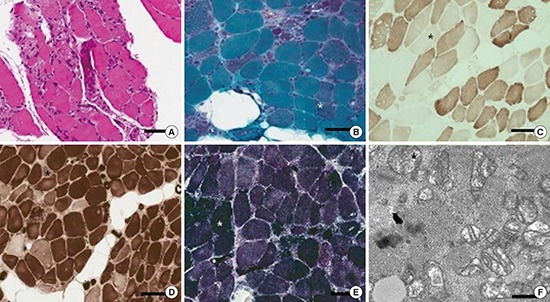
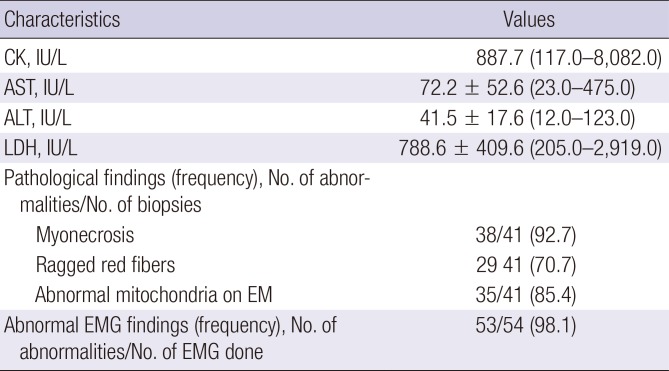
Laboratory findings are summarized in Table 2. Serum CK level was elevated (median: 887.7 IU/L, range: 117.0–8,082.0 IU/L) in the majority of patients (97.9%). The mean lactate dehydrogenase level was also elevated (788.6 ± 409.6, range: 205.0–2,919.0 IU/L). The mean aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were 72.2 ± 52.6 IU/L and 41.5 ± 17.6 IU/L, respectively. The ratio of serum AST to ALT levels (1.76 ± 0.80) was disproportionally high in 97%. Eighty-five patients (89.5%) showed elevation in one of these two liver function tests. Myopathic patterns on electromyography (EMG) were observed in 53 patients (98.1%) among 54 patients who underwent EMG with normal nerve conduction studies. Muscle biopsies from 41 patients, including two in our seven patients, showed characteristic findings of myonecrosis, ragged red fibers, cytochrome-c-oxidase-negative fibers, type 2 fiber atrophy, or abnormal mitochondria in most cases (90%), except four patients with only inflammatory changes (Fig. 1) (56789).
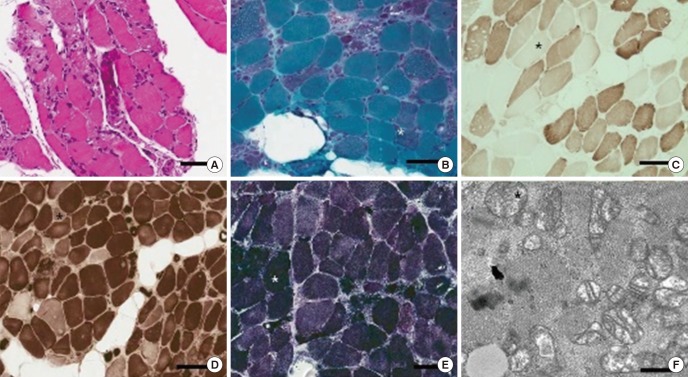 | Fig. 1Typical findings of mitochondrial myopathy from one of clevudine-induced mitochondrial myopathy. (A) Marked muscle fiber necrosis with degenerative muscle fibers (white asterisk) in hematoxylin and eosin stain. (B) Ragged-red fibers with red rim and speckled sarcoplasm (white asterisk) in modified Gomori trichrome stain. (C) Many cytochrome c oxidase-negative fibers (black asterisk) in cytochrome c oxidase stain. (D) Darkly stained type 1 fiber predominance and light stained type 2 fiber atrophy (black asterisk) in adenosine triphosphatase stain at pH 4.3. (E) Darkly stained muscle fibers with mitochondrial proliferation (white asterisk) in succinic dehydrogenase stain. (F) Enlarged mitochondria with blunting and focal clumping of cristae (black asterisk) in electron microscopic examination. Bar: (A-E) 100 μm and (F) 0.5 nm.
|
Table 2
Laboratory, EMG, and pathological findings
Values are presented as median (range) or mean ± standard deviation (range), or number (%).
EMG = electromyography, CK = creatine kinase, AST = aspartate aminotransferase, ALT = alanine aminotransferase, LDH = lactate dehydrogenase, EM = electron microscopy.
![]()
Weakness gradually improved within 11.8 ± 5.8 weeks (range: 2–36 weeks) after discontinuation of clevudine without significant sequelae in all patients (Table 1).
Correlation analysis demonstrated that age, sex, CK, muscle weakness severity, or clevudine therapy duration was not associated with the recovery time from clevudine-induced myopathy.
Go to :
DISCUSSION
Previous clinical trials have evaluated the safety and efficacy of clevudine for 6 months in patients with chronic hepatitis B and reported no adverse effects on muscle. However, 95 patients, including our seven patients, showed that long-term clevudine therapy could cause a reversible mitochondrial myopathy with progressive weakness in the proximal lower extremities. From January 2006 to June 2015, five cases of clevudine myopathy developed among 177 patients who were treated with clevudine in our university hospital. It could be estimated as an incidence rate of 2.8% for clevudine-induced myopathy. In the literature, the incidence rate of myopathy was estimated to be 3.9%–14.4% in patients who were administered clevudine (811121314).
No in vitro and in vivo studies demonstrate the possible mechanism of clevudine-induced myopathy. The mechanism of myopathy induced by zidovudine for HIV, which is also a nucleoside analog reverse-transcriptase inhibitor similar to clevudine, would be similar to that of clevudine myopathy. The use of zidovudine has indicated that apoptosis of skeletal muscle cells can be caused by direct mitochondrial DNA depletion, mitochondrial dysfunction, oxidative stress, and L-carnitine depletion (15). Zidovudine causes damage to mitochondria by impairment of respiratory chain and mitochondrial protein synthesis (16). Recently, telbivudine, another L-nucleoside analogue for HBV infection, has been reported to show evidence of mitochondrial toxicity with a clinical pattern similar to that of fifteen patients (17).
The clinical symptoms of myopathy developed after approximately 14.2 months of clevudine treatment. Clevudine-associated myopathy was characterized by clinical features of subacute progressive weakness in the proximal lower extremities with elevated CK levels. These clinical features might be misdiagnosed as polymyositis. In fact, two of 95 patients, one reported case (8) and one of our seven cases were initially diagnosed with polymyositis. Thus, they were treated with steroid for a few weeks. Steroid had no effect on these two patients with clevudine myopathy. These cases have shown that it is important to know the drugs that cause myopathy such as clevudine to prevent unnecessary workup and treatments.
Decreased motor function in the proximal lower extremity was the most common clinical manifestation in our study. However, bulbar dysfunction or neck weakness also could appear in clevudine myopathy. Clinical symptoms of myopathy improved within 11.8 weeks after clevudine discontinuation. Clevudine therapy discontinuation seems to be an appropriate management for the recovery from myopathy (318).
Although we summarized the typical characteristics of clevudine-induced myopathy by analyzing all the previous cases of clevudine myopathy, including our seven cases, this study has some limitations, such as not assessing the risks or predisposing factors for clevudine myopathy. Further studies are needed to identify the risk or predisposing factors for the occurrence of myopathy during clevudine medication through the comparative analysis between the myopathy group and non-myopathy group.
We should be assured by monitoring motor weakness and serum muscle enzyme levels under the medication of clevudine to detect clevudine-induced myopathy. In addition, in the case of acute or subacute myopathies, a detailed history of medications including nucleoside analogs such as clevudine should be carefully checked so as not to miss the diagnosis of drug-induced myopathy.
Go to :
 XML Download
XML Download