

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pain is often associated with a more rapid progression of cognitive and functional decline, and behavioral disturbance in dementia (1234). Sometimes behavioral disturbance in patients with dementia due to pain can be interpreted as a psychiatric condition, resulting in increased use of psychotropic medications which can often hasten death in elderly patients with dementia (1567). Therefore, it is essential to accurately assess pain for proper intervention in patients with dementia.
Methods of assessing pain include self-reports, physiological measures, and behavioral scales. Self-reported pain intensity may not be reliable for patients with dementia due to their declined cortical cognitive abilities including language function. Physiological measure of pain through heart rate and/or respiration rate is also inappropriate for patients with dementia because most of the patients with dementia are elderly and have diverse variation of physiological ability for each individual independent of the pain (89). A behavioural scale, which assesses the intensity of pain by the medical staff through observing the patients, is usually considered more reliable for patients with dementia. While some behavioural measures of pain intensity have been widely used; Numeric Rating Scale (NRS) (10), Face Pain Scale (FPS) (11), and the Face, Legs, Activity, Cry, and Consolability (FLACC) scale (12). Many observational pain assessment tools have been also developed for patients with dementia; the Abbey Pain scale (13), the Mobilization Observation Behaviour Intensity Dementia (MOBID-2) (14), the Doloplus-2 scale (15), the Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC) (16), Pain Assessment in Noncommunicative Elderly Persons (PAINE) (17), the Pain Assessment in Advanced Dementia (PAINAD) scale (18), et cetera. Among these, the PAINAD tool was developed from categories and behaviours used in the Discomfort Scale for Dementia of the Alzheimer Type (DS-DAT) (19) and the FLACC scale. Therefore, it is a sensitive tool for detecting pain in people with advanced dementia. However, there is a disadvantage in that it is developed only for advanced patients with dementia, has no Korean version or validity study, has a high false positive rate, and frequently detects psychosocial distress rather than pain (20).
The FLACC scale, which was originally designed to measure post-operative pain of pediatric patients, has been identified as a recommended measurement tool for assessing pain of children. It has previously been shown to be a valid and reliable tool for assessing pain of children who have underdeveloped cognitive and language abilities (2122).
Although it is not previously developed for patients with dementia, it included most of the domains that are recommended by the American Geriatrics Society (AGS) to evaluate when assessing pain in patients with dementia; vocalizations/verbalizations, facial expressions, body movements, changes in interpersonal interactions, changes in activity patterns/routines, and mental status changes (23). As there are similarities between demented elderly and children with respect to limited language ability and pain perception, the application of FLACC may be beneficial to patients with dementia.
Therefore, the purpose of this study was to develop the Korean version of the FLACC (K-FLACC) and to verify its reliability and validity in assessing pain of elderly patients with dementia.
MATERIALS AND METHODS
Development of K-FLACC
The forward translation of the original FLACC was made by investigators without affecting the concept originality of the items. Back translation was provided by 1 translator who was not aware of any information of the study. The committee of the development of K-FLACC was established and the members have consisted of medical personnel who have a good command of Korean and English. The translation was reviewed by the committee and this pre-final version of the items was modified by 2 neurologists and 1 advanced practice nurse. The second translation committee reviewed the pre-test results and consolidated the final version of K-FLACC.
The methods of scoring of the K-FLACC were similar to procedures used for the original FLACC. The researchers were provided with information about the K-FLACC behavioral observational pain scale and estimated the degree of pain. The scale consists of the five domains (face, legs, activity, cry, and consolability) with scores of 0, 1, and 2 for each domain and a total score ranging from 0 to 10 (12).
Participants
The evaluation was based on 98 patients with dementia drawn from the Konkuk University Medical Center in the Seoul, Korea. Information about age, sex, the Mini-Mental State Examination (MMSE) score and the global cognitive assessment (Clinical Dementia Rating [CDR] scores) were obtained to analyse response differences by their cognitive state.
Among the patients who were diagnosed with dementia based on the Diagnostic and Statistical Manual of Mental Disorders (4th edition) at the Neurology Department of Konkuk University Medical Center from 24 November to 16 December, 2016, patients whose legal guardian (usually their spouse or offspring) agreed to the informed consents were included. As we considered that most of the participants would not have the capacity to consent, legal guardians' views about their patients participating in the research were sought. Without both the patient's and their legal guardian's approval, the patient was excluded.
Since one of the scales used for validity is a tool that uses numbers, we excluded patients with dementia who did not know the concept of numbers enough to be able to distinguish between large and small. Moreover, the other scale used for validity requires the ability to distinguish facial expressions, so we excluded those who had decreased visual acuity to such extent that they could not identify facial expressions. Patients of CDR 3 were also excluded because that degree of patients with dementia cannot judge or solve a problem at all. After excluding 10 unsuitable patients, a total of 88 patients with dementia were evaluated.
Procedures
The MMSE and CDR scores of the participants were taken from the medical records in the last 6 months. A general practitioner who was educated for administering the K-FLACC estimated the participants' degree of pain according to the five domains before the visiting doctor at the outpatient clinic. After the scoring, the NRS and FPS were assessed to obtain the validity of the K-FLACC. The NRS and FPS are the scales designed to measure the pain of all kinds of subjects and one of the most widely used pain assessment scales. The NRS is a numeric version of the visual analog scale (VAS), which is segmented by 11 numbers. Patients can select a number from 0 to 10 integers that can reflect the intensity of their pain appropriately (10). The NRS needs minimal language translation across cultures and languages and is widely used in Korea (24). The FPS is a pain scale that shows a series of faces ranging from a happy face at 0, “No hurt” to a crying face at 10 “Hurts worst” (11). The patient has to choose the face that best describes how they are feeling. The FPS has demonstrated the Korean version of reliability and validity with other instruments (25).
Another practiced nurse once again administered K-FLACC to measure inter-rater reliability after meeting with a doctor.
Statistical methods
Reliability was assessed by internal consistency and inter-rater reliability. For internal consistency, the Cronbach α reliability coefficient was used. Coefficients needed to achieve excellent and good internal consistency were α > 0.9 and 0.7 < α < 0.9, respectively. For inter-rater reliability, intra-class correlation coefficients (ICC) were calculated. An ICC between 0.6 and 0.8 is considered a good clinical correlation, and an ICC greater than 0.8 is regarded an excellent correlation (26). The concurrent validity of the K-FLACC was evaluated by comparing with the NRS and FPS using Pearson's correlation coefficient.
Age, sex, and current cognitive state were used as factors that could affect the assessment of participant's pain status. The current cognitive state was evaluated by MMSE and CDR scores. The relation of K-FLACC and continuous variables (age, and MMSE scores) was assessed by the Pearson's correlation analysis. Between-group comparisons were performed using the Student's t-test (sex) or one-way analysis of variance (CDR scores). Means, standard deviations, and percentages were used to describe the demographic and cognitive characteristics. Statistical analyses were performed with SPSS 18.0 (IBM Corporation, Armonk, NY, USA), and the level of statistical significance was set at P < 0.05.
RESULTS
Demographics and clinical characteristics
The mean age of the participants was 77.3 (range, 65 to 97) years and females were dominant (n = 60, 68.2%). Almost all participants had mild to moderate cognitive deficit. The additional sociodemographic data are presented in Table 1.
Table 1
Demographic and cognitive characteristics
SD = standard deviation, MMSE = Mini-Mental State Examination, NRS = Numeric Rating Scale, FPS = Face Pain Scale, K-FLACC = Korean version of the Face, Legs, Activity, Cry, and Consolability, CDR = Clinical Dementia Rating.
![]()
Reliability and validity
The internal consistency was good. The Cronbach α for the K-FLACC was 0.75. The internal consistency for each of the five items of the K-FLACC was 0.64, 0.70, 0.61, 0.75, and 0.75.
Test-retest reliability was good, as the ICC comparing the retest to test was 0.73 (95% confidence interval [CI], 0.59–0.82).
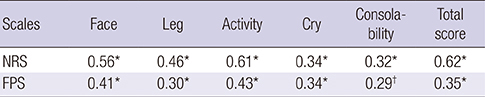
Concurrent validity was good, as the correlations between the K-FLACC and NRS (Pearson correlation coefficient [r] = 0.617, P < 0.001), the K-FLACC and FPS (r = 0.350, P = 0.001) were all significant. The correlation between each item of K-FLACC and NRS and FPS was described in Table 2, and all items showed a significant correlation with a P value of less than 0.05.
Table 2
Pearson correlation coefficient value of each item of K-FLACC with NRS and FPS
| Scales | Face | Leg | Activity | Cry | Consolability | Total score |
|---|---|---|---|---|---|---|
| NRS | 0.56* | 0.46* | 0.61* | 0.34* | 0.32* | 0.62* |
| FPS | 0.41* | 0.30* | 0.43* | 0.34* | 0.29† | 0.35* |
K-FLACC = Korean version of the Face, Legs, Activity, Cry, and Consolability, NRS = Numeric Rating Scale, FPS = Face Pain Scale.
*P < 0.001 level of significance; †
P = 0.010 level of significance.
![]()
Group responses
Age and the MMSE scores had positive (r = 0.22, P = 0.040) and negative (r = −0.26, P = 0.020) correlation with the K-FLACC, respectively. There was no difference of the K-FLACC between groups defined by sex (P = 0.613), and CDR (P = 0.086) (Table 3).
Table 3
Group response to K-FLACC
| Subcategory | Mean (SD) | P value |
|---|---|---|
| Sex | 0.613 | |
| Male (n = 28) | 0.79 (1.7) | |
| Female (n = 60) | 0.97 (1.4) | |
| CDR | 0.086 | |
| 0.5 (n = 47) | 0.60 (1.0) | |
| 1 (n = 32) | 1.16 (1.8) | |
| 2 (n = 9) | 1.67 (2.1) |
K-FLACC = Korean version of the Face, Legs, Activity, Cry, and Consolability, SD = standard deviation, CDR = Clinical Dementia Rating.
![]()
DISCUSSION
The present study indicates that the K-FLACC is a reliable and valid scale to assess pain in patients with dementia. In reliability study, the K-FLACC showed good internal consistency and inter-rater reliability. In validity study, there was a good correlation between the K-FLACC and NRS/FPS. In particular, among the five items of the K-FLACC, the ‘Activity’ item showed the highest correlation with both of the NRS and FPS. Marmo and Fowler (27) reported that the ‘Activity’ was the item showing the least number of discrepancies between raters in studies measuring pain of post-open heart surgery, which indicates that the “Activity” item is the most valuable observational symptoms in the evaluation of unresponsive patients or patients who cannot appropriately express pain.
The NRS is a unidimensional measure for the pain of adults including those with chronic pain due to rheumatic diseases (28) and minimal language translation is needed for using the NRS across countries. It only takes less than 1 minute to complete (10). The FPS was originally created for children to help them communicate about their pain. Now the scale is used around the world with people ages 3 and older (including older adults), facilitating communication and improving assessment of pain (1125). Both NRS and FPS are on a good scale, however, both are anchored by terms describing pain severity extremes (29) like VAS. Those scales cannot assess emotional responses or limitations of activity due to pain. Moreover, these are self-assessment scales, so patients who are unresponsive or incompetent cannot report their level of pain using the scale
K-FLACC is a scale that complements these shortcomings, so it can 1) assess not only the severity of pain but also emotional response and activity limitations due to pain; 2) be applied to all patients with dementia from mild to severe degree as an observational evaluation tool.
The analysis of group responses of the K-FLACC showed interesting results in which age and MMSE, not gender or CDR, are related to pain symptoms. In elderly, several conditions increase the risk of developing pain, including physical and cognitive impairment increases with aging (30). The present study shows that the influence of age-related pain risk factors increases even in patients with dementia.
There are very few studies that report the stronger response to pain as severity progresses in patients with dementia, however, there is a study which shows that pain severity was significantly correlated with dementia severity, neuropsychiatric symptoms, depression, agitation, and quality of life at both time points (31). There are four reasons why patients with advanced dementia are more likely to suffer from pain (32). The first cause is the impact of dementia neuropathology on pain perception and processing including cortical atrophy and white matter lesions. Second is that the assessment of pain in dementia is challenging, particularly because of patients with dementia have limited capacity of self-report by themselves. As dementia gets worse, the language ability and judgment decrease and the asomatognosia progresses. Therefore, there is a high possibility that the pain cannot be solved early. The limited evidence of efficient treatment with analgesics could be another reason explaining the relationship of dementia severity and pain. Dementia is accompanied by aging, so it is difficult to precisely reveal and treat the cause of the pain. Therefore, it is often the case that the pain persists because treating the cause of the pain becomes more difficult. The last reason is the lack of sufficient training for health care practitioners. Patients with dementia are significantly less expressive, so they express pain in a different way than “language.” Health care practitioners need to find it early, however, and often lack training.
The CDR, representing the severity of dementia in our study, did not show a positive correlation with pain which is likely due to 1) small numbers of severe patients with dementia over CDR 2; 2) difference of statistical analysis; 3) difference in severity assessment methods; or 4) difference in the place where the patient was evaluated.
We find that there was no difference in pain between males and females. Previous studies that investigated the prevalence of pain in patients with dementia revealed that gender, obesity, and infection are the risk factors of pain (333435). It is known that females are more vulnerable to pain, but the reason has not yet been revealed. In studies with fibromyalgia, the authors reported that women had a lower pain threshold and more tender points than men, regardless of fibromyalgia (35). However, in the elderly, and especially in the elderly with dementia, the pain is more complex due to multiple comorbidities. Thus, it is necessary to have a well-designed and detailed investigation of whether females are more susceptible to pain and why. A limitation of the study is a lack of analysis according to the etiology or type of dementia, which needs additional study investigating the pain response rate by dementia type. Another limitation is a relatively small number of patients with pain. This seems to be due to the large distribution of patients with dementia of mild severity.
In conclusion, pain in patients with dementia is important but has been under-estimated for a number of biological, social, and clinical reasons. This validation study suggests that the K-FLACC is an efficient tool to evaluate pain in patients with dementia more quickly and accurately and to evaluate easily with constant quality regardless of the raters. It is expected that the pain in patients with dementia will be properly evaluated and treated by using the K-FLACC.
 XML Download
XML Download