

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypogonadism is one of the most common endocrine disorders. Clinical characteristics of patients demonstrating hypogonadism include elevated gonadotropin levels and other hormonal and physical abnormalities. Testosterone deficiency, a hormonal abnormality observed in patients diagnosed with hypogonadism, is associated with central obesity, dyslipidemia, osteoporosis, muscle weakness, and fatigue (1). Recent studies have found that testosterone deficiency occurs as a possible complication in men with type II diabetes and may contribute to impaired performance, mood, and libido (23).
Klinefelter's syndrome (KS) is the most common sex chromosome disorder showing a prevalence of 1 in 660 newborn males (45). Clinical characteristics of KS include elevated gonadotropin levels and hypogonadism, and it can be associated with various physical states such as a tall stature, slender figure with small testes, gynecomastia, narrow shoulders, and sparse body hair. Recent studies have examined the epidemiology of morbidity and mortality associated with KS and found that both are increased due to a variety of factors in KS patients. Increased morbidity and mortality may be caused by hormonal and genetic imbalances (6). KS patients show decreased bone mineral density (BMD) (7), increased glucose intolerance, (8) and an increased risk of cerebrovascular disease (9).
Body composition of KS patients was significantly different compared to normal males. Although their body mass index (BMI) was not different, truncal fat, and waist circumference were significantly increased compared to normal males (4). Unfavorable body composition changes, increased truncal obesity, and decreased body muscle mass may decrease insulin sensitivity (10), which can increase the prevalence of metabolic syndrome. Therefore, we aimed to determine the association between KS and dyslipidemia, which is an important component of metabolic syndrome.
MATERIALS AND METHODS
The KS group included patients who visited the infertility clinic for an infertility evaluation and were confirmed as having a diagnosis of KS and no other chromosomal abnormality, based on chromosome analysis. Patients who visited the clinic for health screening between January 2011 and December 2011 and related no relevant medical and/or surgical history were enrolled in the control group. We retrospectively reviewed medical records of all patients. Clinical history, physical examination, as well as height and weight were evaluated in all enrolled patients, in addition to measurement of serum testosterone, total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, and triglyceride (TG) levels. All blood samples were obtained before 10:00 am after overnight fasting.
Patient characteristics are reported as mean ± standard deviation unless otherwise indicated. Statistical analysis was performed using a paired t-test for normally distributed data and a Mann-Whitney U test for skewed data to evaluate baseline characteristics. A value of P < 0.05 was considered statistically significant. IBM SPSS ver. 18.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
RESULTS
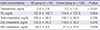
Our study included 55 KS patients and 120 controls. The mean age of patients was 35 years (range, 27–44 years). Mean ages of patients belonging to the KS and control groups did not significantly differ. KS patients were heavier and taller compared to controls; however, BMI values did not significantly differ between the groups (Table 1). Serum testosterone levels were lower in those belonging to the KS group. Evaluation of the lipid profile indicated that TG levels were found to be higher in KS patients while HDL cholesterol was higher in the control group. Serum cholesterol and LDL cholesterol levels were higher in patients belonging to the KS group, but these levels were not significantly different when compared to control levels (Table 2).
Table 1
Baseline characteristics of patients belonging to the KSvs. control groups
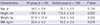
Table 2
Comparison between the KS and control groups with respect to lipid profile
DISCUSSION
During adolescence and after puberty, clinical characteristics of KS include small testes and varying symptoms of androgen deficiency (11). After 25 years of age, 70% of KS patients complain of decreasing libido and erectile dysfunction. The most commonly reported sexual problem in KS patients is hypoactive sexual desire (12), which is seen to improve following testosterone replacement therapy (13). General characteristics observed in KS patients include small testes, gynecomastia, hypogonadism, azoospermia, and low BMD (14). Early diagnosis and treatment of KS significantly improves the patient's quality of life. Testosterone replacement therapy results in increased strength, and virility, as well as improvement in libido, and BMD (115).
Most clinicians examining patients in outpatient departments routinely perform karyotyping and measure hormone levels in those presenting with small testes, hypergonadotrophic hypogonadism, and azoospermia. When testosterone levels are low in symptomatic KS patients, lifelong therapy is planned and initiated to avoid symptoms and sequelae of androgen deficiency.
Life expectancy in patients diagnosed with KS is found to be reduced by 1.5–2 years (8). An important factor associated with the increased mortality risk could be a smaller diameter of arteries that has been recently identified in patients with KS, which can lead to reduced organ perfusion (16). Cardiovascular disease accounts for a significant number of deaths in individuals with low testosterone levels. Testosterone deficiency is also associated with central obesity, hypertension, muscle weakness, reduced insulin sensitivity, and fatigue.
When treating KS patients, physicians should consider multifactorial aspects of patient physiology. Early testosterone replacement improves strength, libido, BMD, and body hair (17). Recently, it has been reported that testosterone demonstrates beneficial effects in men diagnosed with chronic heart failure. Exercise capacity and symptoms were seen to significantly improve following restoration of testosterone levels in men diagnosed with chronic heart failure (18). Testosterone replacement also reduces fatigue and produces a positive effect on mood and behavior (19). However, testosterone replacement does not bring about a positive effect on patient fertility (20).
In Korea, the age-standardized prevalence of metabolic syndrome was noted to be 26.6% in men and 21.3% in women (21). In Northern Europe, the incidence of metabolic syndrome that met the National Cholesterol Education Program (NCEP)/Adult Treatment Panel (ATP) III criteria in KS patients was approximately 50% (422). Currently, no published reports have discussed the incidence of metabolic syndrome in Korean KS patients. In Japan, however, some studies have reported that the incidence of metabolic syndrome in KS patients was 33% in a study that included 60 patients (23). Several studies have explained the correlation between testosterone and metabolic syndrome. Testosterone deficiency in elderly men is associated with various conditions such as reduced insulin sensitivity, central obesity, hypertension, muscle weakness, fatigue, and sexual dysfunction (115). Metabolic syndrome in KS patients is associated with abdominal obesity, reduced insulin resistance, and hypogonadism.
Compared to a placebo group, a significant reduction in visceral adiposity has been observed in middle-aged obese men who were administered testosterone therapy over 8 months (24). Additionally, studies involving a large population of elderly men, and several placebo-controlled studies have concurrently shown that testosterone replacement treatment can increase lean body mass and decrease body fat mass (252627). However, to date, no controlled study has assessed the association between dyslipidemia and KS. Ours was the first observational study that examined dyslipidemia in KS patients compared to controls.
The limitations of our study are that ours was a retrospective study based on medical chart reviews. Most patients enrolled in this study were followed-up regularly and consistently, although all patients could not be followed-up.
Dyslipidemia indices in KS patients were found to be abnormal compared to those in patients belonging to the control group. Based on our findings, we recommend that patients diagnosed with KS who visit urology clinics for infertility counseling should be screened for dyslipidemia and receive appropriate treatment for their metabolic abnormalities.
 XML Download
XML Download