

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Kawasaki disease (KD) is a systemic vasculitis first described by Kawasaki in 1967 (1). KD is the leading cause of acquired heart diseases in childhood. Coronary arteriopathy is the most important complications of KD, ranging from no invasion to multiple giant coronary aneurysms (2). The Japanese Ministry of Health criteria defines coronary arteriopathy as a maximum internal diameter > 3 mm in children < 5 years of age and > 4 mm in children > 5 years, or a segment of > 1.5 times greater than the adjacent segments, or the presence of luminal irregularity. Coronary aneurysms occur in 15%–25% of untreated patients; and 2%–3% of untreated patients die from coronary arteriopathy (3). The American Heart Association proposed that patients with KD receive the therapeutic and follow-up managements according to the degree of coronary involvement (24). The American Heart Association's proposal classifies the therapeutic managements into the five risk levels depending on the degree of coronary involvement: 1) risk level I, no coronary abnormalities at any time of KD; 2) risk level II, transient coronary artery ectasia or dilatation; 3) risk level III, solitary small-to-medium-sized (3–6 mm) coronary artery aneurysm in one or more coronary arteries; 4) risk level IV, one or more large (> 6 mm) or giant (> 8 mm) coronary artery aneurysm and/or multiple or complex coronary aneurysms without obstruction; and 5) risk level V, coronary artery obstruction and/or myocardial ischemia.
Moreover, other cardiac complications may occur in KD. Myocarditis and valvulitis may occur, resulting in abnormal function of myocardium and cardiac valves. Myocarditis may occur in up to 50% of patients with KD. Myocardial injury can be devided into two types: inflammatory and ischemic lesions. Interstitial myocarditis and pericarditis are the inflammatory lesion with neutrophilic predominance. Coronary aneurysms and microcirculatory disorders may cause ischemic myocardial damage, and the patients with ischemic myocardial damage may have cardiac wall motion abnormalities that can be confirmed by echocardiography (2).
There are previous studies on the systolic or diastolic dysfunction in acute KD. However, the long-term outcome of myocardial function has not been fully known in KD. The purpose of this study is to evaluate myocardial function in school-aged children who had the past history of KD.
MATERIALS AND METHODS
Patient characteristics
This is a retrospective study on the children who visited the pediatric cardiac outpatient clinic of Gangnam Severance Hospital from January 2013 to December 2015, and had the past history of KD. Sixty-seven patients in the second grade of elementary schools were included in this study. Echocardiographic measurements of each coronary artery and myocardial function were obtained as the long-term follow-up data, and compared with the baseline data at the time of initial presentation of KD.
Echocardiography and coronary artery measurement
All patients were diagnosed with cardiac lesions based on findings from two-dimensional echocardiography with spectral Doppler and tissue Doppler examination. We used the diagnostic criteria for cardiac lesions in KD defined by the Japanese Ministry of Health (5). The internal diameters of coronary arterial segments were measured from inner edge to inner edge. The right coronary artery (RCA) and left anterior descending coronary artery were measured 3 to 5 mm distal to their origins in the parasternal short-axis view (6). Routinely examined cardiac structures, including valves, left ventricular (LV) internal diameters at end-diastole (LVIDd), LV internal diameters at end-systole (LVIDs), LV ejection fraction (LVEF), LV fraction shortening (LVFS), interventricular septum thickness (IVS) and LV posterior wall thickness (LVPW), were also measured according to the guidelines and standards for performance of pediatric echocardiogram by the Amedican Society of Echocardiography (7).
Equation of coronary artery Z-score
Coronary arterial diameters were normalized for the body surface area (BSA) as Z-scores (standard deviations [SDs] from a predicted normal mean) based on non-linear regression equations derived from a normal non-febrile population. The BSA was computed by the equation of Haycock et al. (8).
The coronary arterial Z-score was computed by the McCrindle's equation and Dallaire Z-scoring Calculator (910). The Z-score (left main artery [LMA], left anterior descending [LAD], and RCA) was obtained by dividing the difference between the actual measurement and the predicted measurement by the SD:
Statistical analysis
Statical analyses were performed using SAS version 9 (SAS Institute, Cary, NC, USA). The statistically significant level was set at P < 0.05. Data were expressed as mean ± SD. The Pearson correlation and paired t-test were used to compare the mean values of echocardiographic indices between the baseline and long-term measurements.
RESULTS
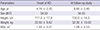
A total of 67 KD patients were analysed. The mean age at the diagnosis of KD was 4.74 ± 2.35 years and the mean age at the follow-up study was 8.6 ± 2.4 years. At the time of diagnosis, the average height was 117.0 ± 17.0 cm and the weight was 22.0 ± 8.0 kg. The average height and weight at the follow-up study was 135.0 ± 14.3 cm and 32.3 ± 10.5 kg (Table 1).
Table 1
Patient characteristic and laboratory findings
![]()
We performed blood tests two times during the acute phase of KD (before the diagnosis of KD and 3 days after immunoglobulin administration). The mean white blood cell count was 9,910.51 ± 4,667.57, hemoglobin was 11.94 ± 1.05, and the platelet count was 381,670 ± 112,090. The mean erythrocyte sedimentation rate was 57.8 ± 33.42 mm/hr and the mean C-reactive protein was 31.26 ± 41.08 mg/dL (Table 2).
Table 2
The laboratory findings at diagnosis of KD
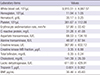
Data are shown as mean ± standard deviation.
KD = Kawasaki disease, BNP = brain natriuretic peptide.
![]()
Table 3 shows echocardiographic findings of KD patients. Interventricular septum thickness at end-diastole (IVSd; 6.17 ± 1.08 mm at baseline vs. 6.55 ± 1.31 mm at follow-up, P = 0.005), LVIDs (23.4 ± 3.08 mm at baseline vs. 25.4 ± 3.20 mm at follow-up, P = 0.003), maximal velocity of late diastolic filling across mitral valve (mitral A) flow (0.53 ± 0.18 m/s at baseline vs. 0.47 ± 0.10 m/s at follow-up, P = 0.006), maximal velocity of early diastolic filling across mitral valve (mitral E)/A ratio (2.07 ± 0.51 at base line vs. 2.27 ± 0.53 at follow-up, P = 0.008), mitral E wave to peak early diastolic tissue wave (E/E') ratio (7.14 ± 1.63 at base line vs. 6.93 ± 1.41 at follow-up, P = 0.013) showed significant differences in the follow-up study. LVEF, LVFS, interventricular septum thickness at end-systole (IVSs), LVIDd, LV posterior wall thickness at end-diastole (LVPWd), LV posterior wall thickness at end-systole (LVPWs), mitral E flow, mean value theorem for derivatives (MVTD), peak early diastolic tissue (E'), peak late diastolic tissue (A'), peak systolic tissue (S') showed no significant differences. Table 4 shows coronary Z-scores of KD patients. The LMA, LAD, and RCA showed no statistically significant differences. But delta value of LMA, LAD, and RCA showed significant differences in the follow-up study.
Table 3
Echocardiographic indices in the KD patients with diastolic data
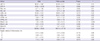
Data are shown as mean ± standard deviation.
KD = Kawasaki disease, LVEF = left ventricular ejection fraction, LVFS = left ventricular fraction shortening, IVSd = interventricular septum thickness at end-diastole, IVSs = interventricular septum thickness at end-systole, LVIDd = left ventricular internal diameters at end-diastolic, LVIDs = left ventricular internal diameters at end-systolic, LVPWd = left ventricular posterior wall thickness at end-diastole, LVPWs = left ventricular posterior wall thickness at end-systole, mitral E = maximal velocity of early diastolic filling across mitral valve, mitral A = maximal velocity of late diastolic filling across mitral valve, mitral E/A = ratio of mitral E to A waves, DT = mitral valvular deceleration time, E' = peak early diastolic tissue, A' = peak late diastolic tissue, S' = peak systolic tissue, E/E' = ratio of mitral E to E' waves.
![]()
Table 4
Echocardiographic findings of coronary arteries

LMA = left main artery, LAD = left anterior descending, RCA = right coronary artery, SD = standard deviation.
*Delta value: mean differences between initial and follow-up data.
![]()
DISCUSSION
The long-term cardiovascular outcome of KD is an important concern. Coronary artery aneurysm can be developed in 20%–25% of untreated patients, and 5% of treated patients. Giant aneurysms can cause coronary artery stenosis and increase the risk of myocardial infarction or death (11). Severe coronary artery disease can develop into coronary stenosis, which can lead to acute myocardial infarction. Coronary aneurysms, greater than 6 mm, are highly likely to cause myocardial ischemia. Other inflammatory heart diseases, such as myocarditis, endocarditis, valvulitis and pericarditis are also common during the acute phase of KD. The characteristics of myocarditis in KD are 1) mild decrease in LV systolic function, 2) transient pericardial effusion, 3) transient inflammatory changes in cardiac valves, and 4) mild or no symptoms. The severity of myocardial dysfunction is associated with myocardial inflammation. More than 50% of patients with KD have myocarditis showing symptoms, electrocardiogram changes, and echocardiographic changes within the first 3 weeks. Inflammatory myocardial changes can be detected with gallium-67 cardiac scan or Tc-99m labeled cardiac scan (12).
Deteriorated LV contractility can be improved after administration of intravenous immunoglobulin (131415). Kurotobi et al. (16) reported LV diastolic dysfunction in children with acute KD, which may be associated with increased brain natriuretic peptide (BNP) levels. Arnold et al. (17) examined asymptomatic children with persistent coronary artery lesions after KD, and revealed diastolic dysfunction in the segments supplied by stenotic coronary arteries under conditions of exercise. Takeuchi et al. (18) reported decreased E' and increased E/E' ratio in the tissue Doppler study in the acute phase of KD, which were normalized in the convalescent phase. The BNP levels were significantly associated with velocity of circumferential fiber shortening and S' at the lateral mitral annulus in the tissue Doppler study, but not significantly associated with E′ lateral, E/E′, and E/A ratios. Selamet Tierney et al. (19) demonstrated decreased E' and impaired diastolic function in patients with coronary artery aneurysms. Decreased diastolic function may result in the increased BNP level. Most of previous studies on myocardial dysfunction in KD were performed in the acute phase of KD. The long-term follow-up study on myocardial function in KD had rarely been reported.
We performed a long-term follow-up study on the second-grade elementary school children who had been treated due to KD, including investigation of myocardial function. In the result of our study, the diastolic function was within reasonable ranges both in the acute phase and long-term follow-up period. However, there were significant differences in diastolic parameters, such as mitral A flow, mitral E/A, and E/E' ratios. The decreased E/A ratio is an expected finding in the presence of impaired relaxation, which slows diastolic tissue velocity (20). As a result, the blood flow from the atrium to the ventricle is delayed and the duration of diastole is prolonged. Defects in the diastolic phase in these patients may create small changes in the myocardial blood flow and reflect inflammatory changes in myocardium and coronary arteries (21).
The mean LMA Z-score in the acute phase was 3.1 and decreased to 0.6 at the time of study, but it was not statistically significant. However, the delta values of individual coronary artery Z-score changes were statistically significant. Some of echocardiographic measurements, such as IVSd, LVIDs, mitral A flow, mitral E/A, and E/E' ratios, showed statistically significant differences in the follow-up period. Therefore, the follow-up echocardiography should be performed to ensure that the relaxation function be improved again. Currently, the follow-up guidelines of KD are mainly based on the presence of coronary artery aneurysms. Children without coronary artery aneurysms have been followed up for less than 2 years in many hospitals. However, we think that even though the follow-up echocardiography is normal, significant alteration or reductions in myocardial function may be present. We intend to follow-up these patients after three and five years and see if functional abnormalities will be recovered. We think that the follow-up guidelines of KD need to be elaborated with respect to the diastolic function and the follow-up period.
 XML Download
XML Download