

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
As human life expectancy increases, the proportion of elderly population also increases. In parallel, the prevalence of chronic kidney disease is increasing worldwide, and initiation of dialysis in the elderly is not uncommon (1). In the United States, the peak incidence of treated end-stage renal disease (ESRD) has increased in the 80–85-year-old age group (1). In Korea, one of the most rapidly aging countries, the proportion of those aged ≥ 65 years among patients with incident ESRD was 39.5% (2).
However, it is controversial whether the initiation of dialysis is beneficial in all elderly patients. In some studies, elderly patients who underwent dialysis showed better survival (34). However, the survival advantage of dialysis was diminished in subgroups of patients with high comorbidities, particularly those with ischemic heart disease (4). Similarly, dialysis initiation in frail elderly patients residing in nursing home facilities did not seem beneficial. Kurella et al. (5) analyzed 3,072 nursing home residents in the United States who started dialysis during June 1998 to October 2000. They reported that the 1 year mortality reached 58% and the functional status of patients was abruptly decreased after dialysis initiation.
Frailty is a distinct multidimensional clinical syndrome (678). About 30% of patients with ESRD were frail (9), and frailty with ESRD was associated with increased risks of fall, fractures, and mortality (9101112). However, most of the previous studies included patients from all age groups. Only a few of the participants were Asian. Moreover, a few studies have evaluated the change of frailty after dialysis initiation. Therefore, we performed the current study to identify the association between frailty and adverse outcomes, and the change of frailty before and after dialysis initiation in the elderly Asian ESRD population, by using data from a prospective observational cohort.
MATERIALS AND METHODS
Study patients
This was a prospective study of patients with incident dialysis from a single dialysis center at Seoul National University Bundang Hospital (SNUBH), a tertiary care hospital, recruited between May 2013 and March 2015. The inclusion criteria were age ≥ 65 years with estimated glomerular filtration rate (eGFR) just before dialysis initiation < 15 mL/min/1.73 m2 and evidence of uremic symptoms or laboratory abnormalities. The exclusion criteria were as follows: 1) diagnosis of malignancy within 3 months before dialysis initiation and 2) dialysis initiation because of acute kidney injury. At the dialysis center in SNUBH, about 150 patients were initiated on dialysis in a year, and half of them were aged ≥ 65 years. The target number of cohort participants was 49. Of the 49 patients, 3 withdrew from joining the study. Finally, we started to follow the clinical course of the remaining 46 patients until June 2016, by interviewing them at the outpatient clinic or through regular telephone interviews performed by a trained research nurse. The maximum observational period for the development of adverse outcomes was 24 months after dialysis initiation.
Frailty
For frailty assessment, we used the comprehensive geriatric assessment (CGA) protocol (7813). Using the scores of nine items in CGA protocol: diagnosis of malignancy, Charlson comorbidity index (14), serum albumin levels, activities of daily living (ADL) based on the modified Barthel index (15), instrumental ADL (IADL) based on the Lawton and Brody index (16), dementia according to the Korean Mini-Mental State Examination score (17), risk of delirium according to the Nursing Delirium Screening scale (18), malnutrition based on the Mini Nutritional Assessment (MNA) score (19), and mid-arm circumference, we can calculate the multidimensional frailty score, which was developed to predict all-cause mortality rates in geriatric patients undergoing surgery (7). The multidimensional frailty score was also validated in other conditions (2021). We defined frailty as a multidimensional frailty score of ≥ 10, the highest quartile of the whole participants.
Measurements and definitions
At enrollment, a trained research nurse collected baseline information including date of birth, sex, date of dialysis initiation, vascular access type, weight (kg), height (cm), alcohol drinking and smoking status, comorbidities (hypertension, diabetes, cerebrovascular disease, and cancer), systolic and diastolic blood pressure, and routine laboratory test results of blood and urine samples from participant interviews and medical record review. Blood pressure was measured before hemodialysis. Body mass index (BMI) was calculated as weight (kg) per square of height (m2). The eGFR was calculated by using the Chronic Kidney Disease Epidemiology Collaboration equation (22). The outcome was the composite of all-cause death or cardiovascular hospitalization. Cardiovascular hospitalization included admission due to cardiac events such as cardiac arrest and ventricular tachycardia and vascular events such as peripheral vascular ischemia and aortic aneurysm.
Statistical analysis
Values are expressed as median (interquartile range [IQR]) for continuous variables and percentage for categorical variables. The difference was analyzed by using the Mann-Whitney U-test for continuous variables and the χ2 or Fisher's exact test for categorical variables. We considered P < 0.05 to be statistically significant. Event-free survival was estimated by the Kaplan-Meier method and compared with the log-rank test. The hazard ratio (HR) and its 95% confidence interval (CI) were analyzed by using Cox proportional hazards analysis, and the odds ratio (OR) was calculated by using logistic regression analysis. The assumption of proportional hazards of frailty was tested by using the log minus log plot. In multivariate analysis, variables with minimal missing rates (< 5%) and P < 0.100 in univariate analysis were chosen as covariates along with age and sex. The difference of CGA results before and 12 months after dialysis initiation was evaluated by using the Wilcoxon signed ranks test for continuous variables and the McNemar test for categorical variables. All analyses were performed with SPSS statistics (version 22; IBM Corporation, Armonk, NY, USA).
RESULTS
The median (IQR) age of the 46 participants was 71.5 (67.8–76.3) years, and 63.0% of them were men. All patients started hemodialysis. None of the patients resided in a nursing home facility. During the median (IQR) follow-up of 17.7 (12.4–21.1) months, four patients died (one of sepsis, one of lung cancer, one of liver cirrhosis, and one of an unidentified cause). Moreover, four patients were admitted to the hospital owing to a cardiovascular cause. The rate of composite outcome was 17.4% (8 of 46). Detailed description of multidimensional frailty score was summarized in Supplementary Table 1. At baseline, the median (IQR) multidimensional frailty score was 8.0 (7.0–10.0), and 32.6% of patients were classified into the frailty group (Fig. 1). Of the patients, 93.5% showed a high comorbidity burden with dependence in IADL. Most of the patients exhibited poor nutrition at baseline showing 63.0% of albumin score 2 (< 3.5 g/dL), 17.4% of malnutrition score 2 (< 17 MNA score), and 82.6% in mid-arm circumference score 2 (< 24.6 cm). Nonetheless, only 19.6% of the patients were fully dependent in ADL, in parallel to the low proportions of patients with dementia and delirium (Fig. 2).

 | Fig. 2Components of multidimensional frailty score. Higher scores of multidimensional frailty score and its components indicate more frail conditions.
CCI = Charlson comorbidity index, IADL = instrumental activities of daily living, ADL = activities of daily living.
|
The comparison results according to frailty status were shown in Table 1. There were more women in the frailty group than in the no frailty group. Patients with frailty showed significantly lower BMI than those without frailty. There were no definite differences in other baseline characteristics. In multivariate logistic regression analysis, female sex and increased BMI were associated with increased and decreased odds of frailty, respectively (Table 2). In the Kaplan-Meier curve, the frailty group showed significantly poorer event-free survival compared to the no frailty group (P = 0.040; Fig. 3). In multivariate Cox proportional hazards analysis (Table 3), after adjusting for age, sex, diabetes, BMI, and time of predialytic nephrologic care, frailty group showed 23.58-times higher hazard of composite outcome development (95% CI, 1.61–346.03; P = 0.021) than non-frailty group. Every 1 score increase of the multidimensional frailty score was associated with 1.63-times higher hazard of composite outcome development (95% CI, 1.01–2.65; P = 0.047).
Table 1
Baseline characteristics of the study patients according to frailty

Values are expressed as median (IQR) for continuous variables and percentage for categorical variables. Differences were evaluated by using Mann-Whitney U-test for continuous variables, and χ2 or Fisher's exact test for categorical variables.
ARB = angiotensin II receptor blocker, ACEI = angiotensin converting enzyme inhibitor, BB = beta blocker, CCB = calcium channel blocker, BMI = body mass index, BP = blood pressure, BUN = blood urea nitrogen, eGFR = estimated glomerular filtration rate, MNA = Mini Nutritional Assessment, IQR = interquartile range.
*V.0350ariable with missing values.
![]()
Table 2
Risk factors associated with frailty
Adjusted OR was calculated by using multivariate logistic regression analysis, and the adjusted covariates were age and variables with P < 0.100 in univariate analysis.
OR = odds ratio, CI = confidence interval, BMI = body mass index.
![]()
Table 3
HR of frailty for composite adverse outcomes

HR was calculated by Cox proportional hazards regression analysis. In multivariate analysis, the covariates were age and variables with P < 0.100 in univariate analysis for either frailty or composite adverse outcome.
HR = hazard ratio, CI = confidence interval, BMI = body mass index.
![]()
The result of changes of the multidimensional frailty score before and after dialysis initiation was shown in Table 4. Of the total of 46 patients, 29 patients (60.4%) underwent follow-up CGA for 12 months. When we compared the baseline characteristics depending on the availability of 12 months follow-up CGA data, patients with 12 months follow-up CGA did not show significant differences from those without 12 months follow-up CGA (Supplementary Table 2). In 29 patients for whom 12 months follow-up CGA data were available, the median multidimensional frailty score was significantly decreased (P < 0.001). This improvement largely relied on improved nutrition: increased serum albumin levels (P < 0.001), increased MNA scores (P = 0.008), and increased mid-arm circumference (P = 0.015). Other components of the multidimensional frailty score were not affected by dialysis initiation.
Table 4
Changes of multidimensional frailty score before and after dialysis initiation (n = 29)
Values are expressed as median (IQR) for continuous variables and percentage for categorical variables. Differences were evaluated by using Wilcoxon signed ranks test for continuous variables and the McNemar test for categorical variables.
MNA = Mini Nutritional Assessment, ADL = activities of daily living, IADL = instrumental activities of daily living, K-MMSE = Korean Mini-Mental State Examination, NDS = Nursing Delirium Screening, CCI = Charlson comorbidity index, IQR = interquartile range.
*Markers that suggest improvement when the scores increase. If not specified, a decreased score signifies an improved condition.
![]()
DISCUSSION
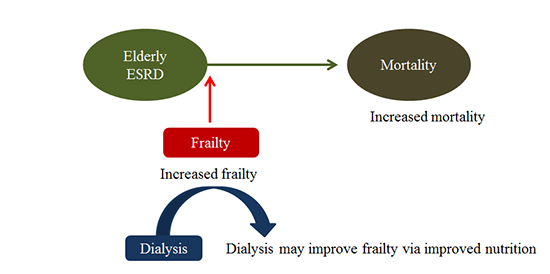
As human life expectancy increases, dialysis initiation in elderly people has become prevalent (12). However, when to start dialysis in elderly patients and whether the practice is beneficial are largely controversial among clinicians. In general, dialysis has been shown to prolong the life span of the elderly population (34). However, recent data suggested that dialysis initiation did not improve the risk of death and quality of life of patients, and the functional status decreased abruptly after dialysis initiation among frail elder patients with incident ESRD who resided in nursing home facility (5). In the meantime, frailty has been highlighted as a key feature of elderly people, and suggested as a risk factor of falls, disabilities, and mortality (6). However, prospective studies that explored the effect of frailty on adverse outcomes in elderly patients with ESRD are sparse, particularly in the Asian population. Moreover, whether frailty is improved by dialysis in elderly patients with ESRD is still inconclusive. In this study, we identified that frail elderly patients with ESRD were at a higher risk of developing adverse clinical outcomes than their nonfrail counterparts. Fortunately, however, frail conditions in elderly patients with ESRD may be improved by dialysis initiation, particularly owing to improved nutrition.
In this study, we identified that female sex and decreased BMI were risk factors of frailty among elderly patients with incident ESRD. In many previous studies, female sex was recognized as a risk factor of frailty, regardless of the method of frailty measurement (10232425262728). However, BMI showed different results. Many previous studies reported that BMI was not associated with frailty (1011232728). In contrast, Delgado et al. (25) analyzed 80 patients undergoing hemodialysis (58% black) and reported that frail patients showed higher BMI than nonfrail patients (28.8 vs. 24.9 kg/m2, P = 0.010). McAdams-DeMarco et al. (29) also reported that frail patients showed a higher rate of obesity than nonfrail patients (51.8% vs. 23.9%, P < 0.001). We believe this different association of BMI with frailty derives from the use of different frailty measurement tools (23). For example, Salter et al. (30) reported that obesity was associated with decreased odds of nephrologist-perceived frailty (OR, 0.21) or nurse practitioner-perceived frailty (OR, 0.44), whereas it was not associated with measured frailty. The result of the hazardous impact of increased BMI on adverse outcome also needs cautious interpretation since there is a reverse epidemiology between BMI and mortality in ESRD patients (31). As with previous studies (10112324), frailty defined by the multidimensional frailty score was also associated with an increased risk of death or cardiovascular hospitalization. Up until recently, the reason why frailty was associated with adverse clinical outcomes has been unclear. Subjects with frailty tended to have endothelial dysfunction (32) and inflammation (33). These subclinical pathophysiologic disturbances may explain the intimate association between frailty and various comorbidities, such as diabetes and cardiovascular diseases (10112324272830). Subsequent studies are needed to find out a pathophysiologic link between frailty and adverse outcome in elderly ESRD patients.
Our study has several strengths. This was the first study to suggest that frailty can be improved by dialysis in elderly patients. In the current study, the multidimensional frailty score significantly improved 12 months after dialysis initiation. During the study period, only 8.7% of the patients died, and their functional and cognitive capacities were not deteriorated by dialysis. To our best knowledge, only one study evaluated the change of frailty in patients with ESRD (34). McAdams-DeMarco et al. (34) reported that frailty ultimately improves after renal replacement therapy (RRT) in patients with ESRD. However, the study by McAdams-DeMarco et al. (34) was not comparable with the current study because the RRT in their study was kidney transplantation, not dialysis, and they included patients with ESRD of all ages. Kurella et al. (5) reported that most of the participants in their study died, and the functional status of patients sharply declined 1 year after dialysis initiation. Unlike the current study, they did not use the concept of frailty, thus making a direct comparison with the current study impossible. Nonetheless, the higher death rate with functional deterioration after dialysis initiation in the study by Kurella et al. (5) was rather different from the results of the current study. We assume that the participants in the study of Kurella et al. (5) may be more frail than those in the current study; all of the participants in the study of Kurella et al. (5) resided in nursing home facilities, and the serum albumin level was lower than that in the current study. On the basis of the aforementioned study results, we hypothesized that dialysis may have a beneficial effect on clinical outcomes even for elderly patients with ESRD, if the patients are not severely frail. Second, there have been several studies which suggested that poor nutrition was a risk factor of adverse outcome in ESRD patients (353637). Malnutrition is a key feature of frailty (38). In this study, the improved frailty was largely attributed to improved nutrition. Therefore, the current study may provide the link between nutrition, frailty and adverse outcome, particularly in elderly ESRD patients. Third, the study population was solely composed of patients with Asian ethnicity, the proportion of which was very low in previous studies (51011), and we only included elderly patients with ESRD.
Our study also has several limitations. First, frailty defined by the multidimensional frailty score in elderly patients with ESRD was used for the first time in the current study. However, this limitation may be acceptable as the CGA protocol for calculating multidimensional frailty score is well validated in various conditions (7813), and the study results were concordant with those of previous studies (10112324). Moreover, unlike previous frailty definitions that mainly focused on physical weakness (6), our frailty definition was more “multidimensional” as it emphasized nutrition and mental weakness, along with physical weakness. Future studies to validate our study results need to follow. Second, not all participants repeated the CGA protocol 12 months after the dialysis. However, the baseline characteristics depending on the availability of 12 months follow-up CGA data were not different between participants with and those without follow-up CGA (Supplementary Table 2). Third, the study sample was small, and the observational period was short. Therefore, the studied cohort may not be representative of elderly ESRD patients, and the event rate was erroneously low. Some controversial results including the association between BMI and adverse outcome should be confirmed in subsequent large prospective studies. Finally, the generalizability might be limited because this was a single-nation and single-center study.
In conclusion, frailty is associated with an increased risk of adverse outcomes in elderly patients with incident ESRD. According to our study results, frailty may be improved by dialysis, even when applied to elderly patients with ESRD. A future large study needs to be conducted to confirm our study results.
 XML Download
XML Download