

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Solid pseudopapillary tumor (SPT) is an uncommon, low-grade malignant neoplasm that almost exclusively occurs in the pancreas, constituting 1%–2% of exocrine pancreatic tumors. It has a favorable prognosis after complete resection and more than 95% of patients are curable (1). SPT of extrapancreatic origin is extremely rare, with only 19 cases have been reported in the English literature so far. However most of these cases exhibited benign tumor behaviors and focused mainly on microscopic and immunohistochemistry findings. Therefore, we reported a case of extrapancreatic SPT with peritoneal dissemination focusing on radiologic findings.
CASE DESCRIPTION
In December 2015, a 61-year-old woman with a 4-month history of abdominal pain was admitted to our institute. She had no medical history except diabetes mellitus. On physical examination, she showed abdominal distension and whole abdominal tenderness. Laboratory data revealed increased white blood cell (WBC) counts (107,980 cells/μL), C-reactive protein level (216.3 mg/L), cancer antigen (CA)-125 (2,441 U/mL), and CA 19-9 (67.13 U/mL). Carcinoembryonic antigen (CEA) and alpha-fetoprotein (AFP) were within normal range.
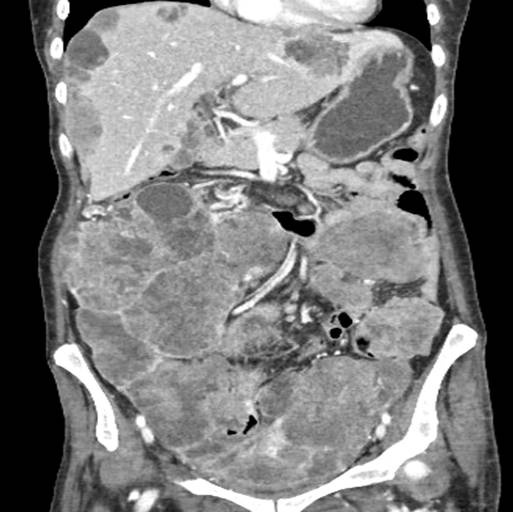
Dynamic contrast-enhanced abdominal computed tomography (CT) revealed huge masses with solid and cystic components replacing the whole abdomen, measuring about 22.7 × 8.9 ×18.7 cm3 (Figs. 1 and 2). The mass was well-encapsulated and showed a mainly smoothly lobulated margin, but a small portion of the mass showed ill-defined margin with invasion into adjacent abdominal wall and small bowel. Despite invasion, the small bowel loops were not obstructed. The solid portion showed persistent and gradual enhancement pattern. A necrotic, hemorrhagic component and amorphous, scattered calcifications were observed within the tumor (Figs. 1 and 3). Not only were there multiple seeding masses scalloping liver surfaces, but there also were metastatic lesions in the liver and spleen. The peritoneum showed mild thickening without nodularity. Lymphadenopathy, ascites, and extra-abdominal metastases were not found. The pancreas, both kidneys, and the adrenal glands were normal. Both ovaries could not be identified. Based on clinical and imaging findings, our preferred diagnosis was peritoneal carcinomatosis of an unknown origin or that of which originated from the ovary. Malignant peritoneal mesothelioma or primary peritoneal serous carcinoma was also a considerable diagnosis.
Fig. 1
CT images in mid-abdomen level. (A) Precontrast, (B) portal venous phase, (C) 3-minute delayed phase. The tumor shows heterogeneously persistent enhancement, which replaces entire abdomen. Amorphous calcifications (black arrows) and internal necrotic foci (asterisks) are also identified. Despite of bowel invasion (white arrows), bowel obstruction does not occur.
CT = computed tomography.
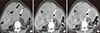
Fig. 2
CT images of SPT on portal venous phase with adjacent organ invasions. (A) Axial image, (B) coronal image. Heterogeneously enhanced seeding masses (asterisks) scallop the liver surface. The masses are separated from pancreatic head. Pancreas (black arrows) is normal. Focally ill-defined margin of the mass reveals direct invasion to right abdominal wall (white arrows).
CT = computed tomography, SPT = solid pseudopapillary tumor.
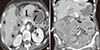
Fig. 3
CT images in the pelvic cavity level. (A) Precontrast, (B) portal venous phase. The tumor shows intralesional hemorrhage (black arrows), scattered calcification (white arrow) and internal necrotic foci (asterisks). Both ovaries are not visible.
CT = computed tomography.

On hospital day (HD) 2, US-guided biopsy was done. On ultrasonography (US), the mass showed relatively well-encapsulation and heterogeneous echogenicity with cystic or necrotic components. The posterior capsule of the mass had an echogenic rim with good through transmission of sound. Internal echogenic spots and septations were also noted. On color Doppler imaging, vascularity was increased at the inner solid portion (Fig. 4).
Fig. 4
Transverse ultrasonographic images of the SPT. (A, B) Gray scalses, (C) color Doppler image. The tumor shows well-encapsulated, heterogeneous echogenicity in gray-scale images (A, B). Cystic or necrotic components (asterisks), internal echogenic spots (white arrows), and septations (short black arrows) are identified. The posterior capsule of the mass (black arrows) shows an echogenic rim with good through-transmission of sound. Color Doppler image (C) shows increased vascularity at the solid portion of the tumor. Curved arrow indicates biopsy needle.
SPT = solid pseudopapillary tumor.

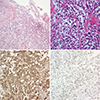
A histological examination of biopsy revealed that the tumor had a heterogeneous growth with predominantly solid pattern (Fig. 5). Pseudopapillary structures, consisting of detached tumor cell around the vessel, and punctate necrosis were present. The stroma of the tumor was sclerotic. Tumor cells had a relatively monotonous nucleus and clear cytoplasm. The tumor nuclei were fine chromatin with indistinct nucleoli and focal pleomorphism. Mitosis was frequently seen in the tumor. The tumor cells were immunoreactive for vimentin and CD10, while they were negative for pan-cytokeratin, synaptophysin, chromogranin, and CD117. β-catenin nuclear translocation and loss of E-cadherin were observed in the tumor by immunohistochemical staining. Based on the evidence uncovered, she was diagnosed with extrapancreatic SPT.
Fig. 5
Histological features of the tumor. (A) H & E stained, × 100, (B) H & E stained, × 400. (C) Immunohistochemical staining for β-catenin nucleus, (D) Immunohistochemical staining for E-cadherin. The tumor (A, B) shows solid and pseudopapillary growth with a monotonous round to oval nucleus, fine chromatin and abundant mitosis. Translocation of β-catenin nucleus (C) and loss of E-cadherin (D) are observed on immunohistochemical staining.
H & E = hematoxylin and eosin.
On HD 10, the patient developed fever up to 40°C and Candida tropicalis was cultured in the patient's serum. Although antibiotics and anti-fungal agents were administered, she died from severe sepsis on HD 14.
DISCUSSION
SPT is a benign or low grade malignant tumor, exclusively occurs in the pancreas. It usually affects young women in the second or third decade of life. Treatment of choice of SPT is surgery and more than 95% of the patients are curable after complete resection. Although most lesions exhibit benign behaviors, about 15% of SPT show metastasis or invasion to adjacent structures. Liver is the most common site of metastasis. However, metastasis or invasion to adjacent organ is not a contraindication of surgery and in that case, debulking surgery can be considered. The patients with SPTs have a long survival period even in the presence of residual tumor after treatment and prognosis of SPTs with treated liver metastases usually surpasses 5 years (12).
Extrapancreatic SPT is extremely rare. Only 20 cases, including the present case, have been reported in the English literature so far. Primary sites were the mesocolon, omentum, ovary, retroperitoneum, liver, stomach, and our case is considered an extrapancreatic SPT probably occurring in the mesocolon, omentum, or ovary. In terms of prognosis of extrapancreatic SPTs, like pancreas SPT, most of the tumors showed good prognosis after surgical resection as a primary treatment regardless of tumor recurrence or metastasis (134567891011). On the basis of previous literatures reviews, four cases (20%) showed metastasis or tumor recurrence and half of them showed more than eight years survival period by repeating treatments for recurrence (17). Although there is limitation due to small patient numbers, it seems that in older patients, extrapancreatic SPT with malignant behaviors seems to have a poor prognosis (7).
In immunohistochemical staining, SPT shows some specific features. In our case, the tumor revealed translocation of β-catenin nuclear and loss of E-cadherin. About 90% of SPTs have carried mutation of β-catenin gene. Mutation of exon 3 in β-catenin gene leads to an abnormal accumulation of β-catenin in the nucleus. Meanwhile, E-cadherin has a role of cell adhesion intimately linked to β-catenin. Although the exact mechanism is unknown, loss of E-cadherin and cytoplasmic nuclear expression of β-catenin occurring simultaneously is a distinctive immunophenotype of SPT (12).
Imaging findings of extrapancreatic SPT was similar with those of pancreatic SPT (11). On CT scans, it manifests as a well-encapsulated mass with solid and cystic components due to hemorrhagic degeneration or necrosis. The solid portions are usually identified on the edge of the mass and the cystic spaces are located in the center. On dynamic enhancement images, SPT manifests heterogeneous enhancement on arterial phase and progressive, centripetal enhancement on delayed phase (13). In the present case, morphologic features and enhancement pattern at CT scan resemble those of classic SPT.
On the studies comparing CT findings between benign and malignant SPT, there are significant differences with capsule morphology, its margin, and tumor size. Malignant SPTs frequently show focal discontinuity of the capsule with ill-defined margin and relatively large size compared with benign SPT, which are consistent findings with our case. Meanwhile, Yin et al. (14) reported amorphous or scattered calcifications were less observed in the malignant SPTs. However, our case demonstrated these calcifications despite malignant transformation. Therefore, further investigations should verify the relation between intratumoral calcification and malignant transformation.
The characteristic US findings of SPT are well-circumscribed, cystic and solid mass with internal heterogeneous echogenicity. When the tumor is small, it can manifest as a solid looking mass with hypoechogenic feature. Sometimes internal septations, echogenic spots, and fibrotic tumor capsule can be identified. The septations and fibrotic capsule usually show an echogenic rim, and the capsule manifests good through-transmission of sound at the posterior margin as seen in our case (15). Internal calcifications are identified as echogenic spots, but some tumors show rim calcification. Although there are a few cases reporting US features of malignant SPT, these are not different from CT features. Being large and showing ill-defined margin with surrounding organs can suggest malignant transformation as our case. Meanwhile, for the accurate diagnosis and tissue sampling, transabdominal US (TAUS) and endoscopic US (EUS) are valuable tools. Although the imaging features in both modalities resemble, evaluation of internal echogenicity including tissue components is superior in EUS to TAUS. In addition, when the tumor is small and in a location only feasible for EUS, EUS can be applied. However, in the tumors with large size and dense rim calcification, TAUS is more suitable than EUS (16).
Our differential diagnoses were peritoneal carcinomatosis of an unknown origin and other primary malignancies such as malignant mesothelioma and primary peritoneal serous carcinoma. First, findings suggestive of peritoneal carcinomatosis include ascites, nodular thickening of peritoneum, and masses. Small bowel obstruction is the most common complication. However, because SPT is a soft tumor, it rarely causes bowel obstruction. In the present case, in spite of direct invasion of bowel loops, bowel obstruction was not present. Second, peritoneal malignant mesothelioma shows either irregular/sheet-like thickening of the peritoneum or dominant, intraperitoneal masses with peritoneal studding. It is frequently related with asbestos exposure and shows male predominance. This tumor may be excluded due to different clinical findings and peritoneal change, which is mild, even thickening of the peritoneum. Finally, primary peritoneal serous carcinoma manifests as overlapping imaging features with peritoneal carcinomatosis and malignant mesothelioma. The majority of the patients are postmenopausal women and shows elevation of serum CA-125. The diagnosis can be made according to findings of peritoneal and omental masses with ascites and without primary visceral malignancy or ovarian tumor. As both ovaries could not be identified in the present case, this disease can be considered as a differential diagnosis, but no ascites were found in this present case (17).
Our report has a limitation. We could not definitely identify the precise primary site because of extensive tumor growth replacing the whole abdominal cavity and localized tissue sampling instead of surgical confirmation. However, to the best of our knowledge, there has been no report with extrapancreatic SPT with aggressive behavior like our case. In addition, although there have been a few reports about imaging findings of pancreatic SPT on the CT or US findings, there has been no report focusing on the detail imaging findings with good image quality in the extrapancreatic SPT with malignant transformation. Therefore, we believe this case report would be valuable.
In summary, we report a very rare case of extrapancreatic SPT with aggressive tumor behavior. Although CT imaging features closely resembled those of conventional pancreatic SPTs as encapsulated solid and cystic masses, the focal discontinuity of the tumor capsule with some ill-defined margin and invasion of adjacent structures were findings suggestive of malignant transformation. With those CT findings, the presence of an echogenic fibrotic capsule surrounding the mass and internal septations with amorphous and scattered calcifications on US can be useful in considering this disease entity.
 XML Download
XML Download