

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dextrocardia is a rare congenital anomaly in which the apex of the heart is located in the right hemithorax with its base-to-apex axis directed to the right and caudad (1). A population-based cohort study showed that the incidence of dextrocardia was estimated to be 1 in 12,019 pregnancies (2). Persistent left superior vena cava (SVC) is a venous development anomaly usually draining into the right atrium through a dilated coronary sinus, occurring in approximately 0.3% to 0.5% of the general population (3). Therefore, the patients with left SVC may have an increased risk of developing cardiac arrhythmias. Pulmonary artery (PA) sling is also a rare congenital anomaly in which the left PA originates from the right PA and encircles the distal trachea. The PA sling is often associated with congenital tracheal anomalies such as tracheal stenosis and tracheal bronchus.
These anomalies can occur alone, but may be associated with other congenital cardiovascular or tracheobronchial malformations. Most of the cases were detected in their infancy or childhood because signs and symptoms frequently present early in life. However, it is possible for some congenital anomalies to go undetected for a long time. Symptoms can also vary from non to life-threatening, and on rare occasion, may lead to hemodynamically unstable tachyarrhythmias. We report a rare case of coexisting dextrocardia with situs solitus, persistent left SVC, PA sling and right tracheal bronchus firstly presented with paroxysmal supraventricular tachycardia (PSVT) associated with Wolff-Parkinson-White (WPW) syndrome in adult age.
CASE DESCRIPTION
A 56-year-old man was admitted on August 30, 2011 with a 6-month history of increasing chest discomfort. He had experienced short duration of chest discomfort once or twice a year for the last several years. The chest discomfort occurred more frequently about six months prior, and he felt repetitive chest discomfort and rapid heartbeat sensation since the day before admission. A chest radiograph revealed dextrocardia (Fig. 1). He said it was firstly detected in 2008 at another institute by chance, but no further evaluation was done. No other remarkable medical history was found.

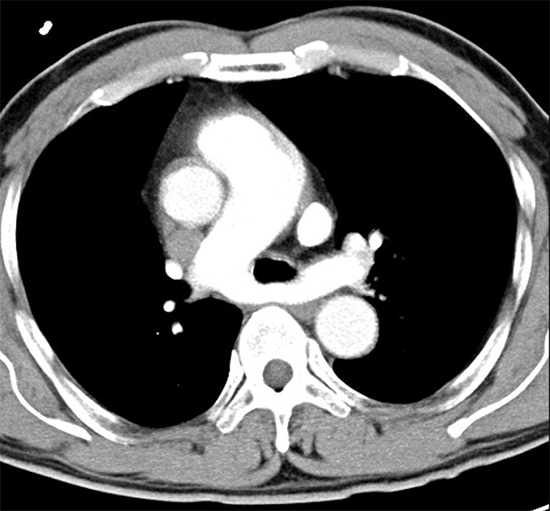
A 12-lead electrocardiogram showed a heart rate of 190 bpm and wide QRS complex tachycardia (Fig. 2A). Intravenous adenosine was administered initially at 6 mg and then 12 mg in an effort to convert the rhythm. A follow-up electrocardiogram revealed a shortened PR interval (112 ms), a slurring and slow rise of the initial upstroke of the QRS complex (delta wave), and secondary ST segment and T wave changes (Fig. 2B). Transthoracic echocardiogram demonstrated no clinically significant abnormalities. A 24-hour Holter revealed baseline sinus rhythm with rare premature ventricular complexes and short-runs of paroxysmal atrial tachycardia. To rule out coronary artery disease and find out other congenital cardiovascular malformations, a computed tomography (CT) angiography was performed. There was no significant intracoronary abnormality except myocardial bridging in a diagonal branch. However, persistent left SVC draining into the right atrium via the coronary sinus was observed (Fig. 3A). The PA sling, in which the left PA arose from the right PA, was constricting the distal trachea (Fig. 3A). A right tracheal bronchus was also detected (Fig. 3B and 3C). However, this narrowing of the distal trachea did not cause symptoms and did not significantly affect his pulmonary function. In a few days, wide QRS complex tachycardia with a heart rate of 185 bpm recurred in spite of medical treatment. Because the patient became hypotensive, he underwent urgent synchronized cardioversion with 100 J, which successfully converted his tachyarrhythmia to sinus rhythm. He was diagnosed with WPW syndrome with PSVT, and referred to a cardiac electrophysiology clinic to undergo radiofrequency ablation. The accessory pathway was located in the left lateral wall, and radiofrequency ablation was successfully performed without significant complications. Until now, he has remained stable and comfortable without recurrence of chest discomfort or palpitation.
 | Fig. 2Electrocardiograms. (A) An initial 12-lead electrocardiogram showed a heart rate of 190 bpm and wide QRS complex tachycardia. (B) After administration of intravenous adenosine, a follow-up electrocardiogram revealed bradycardia with a shortened PR interval and a slurring and slow rise of the initial upstroke of the QRS complex (black arrows).
|

DISCUSSION
Dextrocardia is a rare congenital anomaly in which the apex of the heart is located in the right hemithorax. It is generally known that there are three types of dextrocardia. In case of situs solitus, the right lung has three lobes and an eparterial bronchus (bronchus above the PA), whereas the left lung has two lobes with a hyparterial bronchus (bronchus below the PA) (1). As in the present case, situs solitus dextrocardia is often complicated by various cardiac malformations (2).
Persistent left SVC is a relatively rare congenital venous development anomaly, but the incidence is ten-fold higher in patients with congenital heart malformation (3). Persistent left SVC is characterized by a left-side SVC usually draining into the right atrium through a dilated coronary sinus (4). Therefore, besides being associated with other congenital heart malformations, the most relevant clinical implication of left SVC is the association with disturbances of cardiac impulse formation and conduction such as atrioventricular nodal reentrant tachycardia, atrioventricular reentrant tachycardia, atrial fibrillation, and atrioventricular conduction blocks (35). As in the present case, a few reports have also described the coexistence of left SVC with WPW syndrome (67).
Furthermore, the PA sling is also a rare congenital anomaly in which the left PA originates from the right PA and encircles the distal trachea (8). The PA sling is frequently associated with congenital tracheal and cardiac anomalies. In a retrospective review of 18 children with PA sling, right tracheal bronchus was found in about 20 percent of patients. Persistent left SVC was co-occurred in about 20% as well (9). Most cases reported presented respiratory symptoms in their early ages because of the compression of the lower trachea, and as in the present case, a few patients with PA sling diagnosed incidentally in their adolescence or adulthood were asymptomatic (10).
The embryology of the PA sling has not been completely delineated. A report suggested a hypothesis that PA sling complex might result from the spatial coexistence of PA sling with right tracheal bronchus or left SVC in the embryonic foregut mesoderm (9). However, no clear evidence of an embryologic or genetic relationship among these multiple congenital cardiac and tracheal anomalies has been documented.
Congenital anomalies do not always cause symptoms or medical problems even until adulthood (1112). To the best of our knowledge, there was no reported case of situs solitus dextrocardia coexisting with persistent left SVC, PA sling and right tracheal bronchus, which was initially presented with PSVT due to WPW syndrome in a middle-aged adult. Although asymptomatic, in patients with a cardiovascular anomaly we should consider radiographic evaluation of possibly combined cardiovascular and airway malformations, and electrocardiography or echocardiography if clinically indicated. Further genetic and embryonic studies are needed to detect a possible relationship among these congenital anomalies.
 XML Download
XML Download