

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Initial management of trauma patients who require massive transfusion is important (1). Above all, packed red blood cell (pRBC) transfusion is essential for the treatment of hemorrhagic shock because it improves not only blood pressure but also oxygen debt (2). Because fast transfusion may improve clinical outcomes (34), the time for transfusion is important. Uncross-matched ABO type-specific pRBC (ABO RBC) is usually utilized in hemorrhagic shock patients but requires time for blood sampling, ABO typing, and pRBC delivery. Therefore, uncross-matched type O pRBCs (UORBCs) can be utilized in urgent situations for faster transfusions.
In developed countries, UORBCs have been utilized since the 1980s (5), and their safety has been reported (6). Moreover, even type O whole blood has been utilized in the United States Army (7). Nevertheless, UORBC transfusion is uncommon in Korea because of the transfusion system and the fear of adverse effects. However, a new blood storage system was established at our trauma center in March 2016 and 4–6 UORBCs were always prepared in the trauma bay (Fig. 1). Before that, the blood bank was located on another floor of the hospital. It took significant amounts of time to deliver blood samples and product; however, after the bank was established in the trauma bay, UORBCs could be administered immediately.

A preliminary study suggested the safety and efficacy of UORBC transfusion system in our center (8). We expected that faster transfusion would improve the clinical outcomes of traumatic shock patients compared with those of the ABO RBC transfusion system.
MATERIALS AND METHODS
Patients and study design
In March 2016, a new blood bank was installed at the trauma bay and 4 to 6 UORBCs were prepared according to blood storage amount in hospital. UORBCs were stored for about 2 months and re-filled by the main blood bank in hospital when UORBC was utilized. The blood bank was strictly managed by nurses and trauma surgeons who participated in the committee of transfusion in hospital. From when the bank was established to February 2017, data from trauma patients who received UORBCs in the trauma bay and trauma patients who received ABO RBCs in the emergency room (ER) or trauma bay from January 2013 to December 2015 were retrospectively reviewed. To detect urgent transfusion, patients who received ABO RBCs within 90 minutes from admission to the ER or trauma bay were included. The ABO RBC transfusions followed the clinical guidelines for transfusion from the Centers for Disease Control and Prevention in Korea (9). UORBCs were administered if the patient presented unstable vital signs (more than three of the following: heart rate > 110 beats/min, systolic blood pressure < 100 mmHg, body temperature < 35°C, pH < 7.25 in arterial blood gas analysis, and lactate concentration > 4.0 mmol/L), with no response after the administration of 1–2 L of crystalloid fluid, required a massive transfusion, or had evidence of massive bleeding. However, not all cases followed these specific indications and transfusion was decided by the trauma team leader who was certificated by the Advanced Trauma Life Support program. Before the transfusion, blood type sampling must be done. After the transfusion of 2–4 units of UORBCs, ABO RBCs were administered, if available. The exclusion criteria were as follows: age under 19 years, uncertain trauma history, pulseless on arrival, and transferred from another hospital.
Because this study was a retrospective review and the indications for UORBC and ABO RBC administration could differ, the clinical outcomes were compared using propensity score matching utilized using a 1:1 matching technique without replacement.
Data collection and outcome measurement
The data collected included demographic variables, vital signs, lactic acid concentration, Glasgow Coma Scale (GCS) score, Injury Severity Score (ISS), Abbreviated Injury Score (AIS), transfusion time, amount of transfusion in 24 hours after admission, injury mechanism, emergency operation, mortality, and intensive care unit (ICU) length of stay (LOS). The primary outcome was mortality in 24 hours, while the secondary outcomes were in-hospital mortality and ICU LOS. ICU LOS was calculated among the survivors.
The transfusion time was calculated from hospital arrival to the start of transfusion. Data on lactic acid levels were obtained from initial laboratory data before transfusion. An emergency operation was defined as any emergency surgery in the operating room performed under general anesthesia. Massive transfusion was defined as the transfusion of more than 10 units of pRBCs in 24 hours.
Statistical analysis
The propensity scores were estimated using variables including age, sex, vital signs, lactic acid concentration, GCS score, ISS, AIS, emergency operation, and injury mechanism. Continuous data were expressed as median values and interquartile ranges (IQRs) because they were not followed a normal distribution, while categorical data were presented as frequencies and percentages. After propensity matching, variables and outcomes between the two groups were compared by Mann-Whitney U and χ2 tests for continuous and categorical variables, respectively. All analyses were performed using IBM SPSS statistics for Windows, version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
Data from 586 patients were included; after exclusion, data from 252 patients were reviewed (Fig. 2). UORBCs and ABO RBCs were administered to 64 and 188 patients, respectively. The median age was 47 years and men were dominant in both groups. The UORBC group was older and the vital signs differed significantly from those of the ABO RBC group. Transfusion time was much shorter in the UORBC group, about 11 minutes from admission to the ER. A total of 24 patients from UORBCs and 59 patients from ABO RBCs were deceased by as follow; UORBC (bleeding 6, central nervous system 13, multi-organ failure/sepsis 5), ABO RBC (bleeding 14, central nervous system 25, multi-organ failure/sepsis 19, cardiogenic 1). Although mortality did not differ significantly between groups, but the ICU LOS was significantly longer in the UORBC group (Table 1).
Fig. 2
Diagram of the study population.
UORBC = uncross-matched type O packed red blood cell, ABO RBC = ABO type-specific packed red blood cell.

Table 1
Patient baseline characteristics
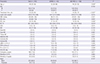
Values in parenthesis are median (quartile) or number (%).
*P <0.05
UORBC = uncross-matched type O packed red blood cell, ABO RBC = ABO type-specific packed red blood cell, SBP = systolic blood pressure, HR = heart rate, RR = respiratory rate, BT = body temperature, GCS = Glasgow Coma Scale score, ISS = Injury Severity Score, AIS = Abbreviated Injury Score, pRBC = packed red blood cell, FFP = fresh frozen plasma, Plt. = platelets, ICU LOS = intensive care unit length of stay.
Clinical outcomes after propensity matching
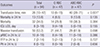
After propensity matching, 47 patients were selected from each group; of these, the selected parameters did not differ significantly between groups (Table 2). Transfusion time was still shorter in UORBC group, but mortality, ICU LOS, and the amount of transfusion were not significantly different. However, although there was no statistical difference, the 24-hour mortality in UORBC group was more than half that of the ABO RBC group (4 [8.5%] vs. 9 [13.8%], P = 0.135) and the rate of massive transfusions was less in the UORBC group (21 [44.7%] vs. 29 [61.9%], P = 0.098) (Table 3).
Table 2
Patient characteristics after propensity matching
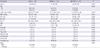
Values in parenthesis are median (quartile) or number (%).
UORBC = uncross-matched type O packed red blood cell, ABO RBC = ABO type-specific packed red blood cell, SBP = systolic blood pressure, HR = heart rate, RR = respiratory rate, BT = body temperature, GCS = Glasgow Coma Scale score, ISS = Injury Severity Score, AIS = Abbreviated Injury Score.
Table 3
Clinical outcomes after propensity score matching
DISCUSSION
The time to transfusion from arrival to the trauma bay was shorter after the establishment of the new blood bank system. Although mortality was not statistically different between groups, it assumed that the UORBC group might have lower 24-hour mortality.
Transfusion is important in hemorrhagic shock patients and is emphasized in recent Advanced Trauma Life Support (10). In addition, Powell et al. (11) suggested that time to transfusion is important and that delay in time to pRBC administration of as short as 10 minutes was associated with increased mortality. Brown et al. (12) reported that prehospital UORBC transfusion improved clinical outcomes in severe blunt trauma patients. Hence, UORBCs are essential to traumatic shock patients for fast transfusion.
Lee et al. (13) described UORBC transfusions in Korea, but it took about 35 minutes for UORBC and 170 minutes for ABO RBC. In the current study, the new blood bank system in the trauma bay reduced the time for UORBC transfusion to about 11 minutes. Moreover, the time to ABO RBC administration was 44 minutes in this study, similar to the UORBC time in Lee's report (13). Therefore, in order to more quickly utilize UORBCs, they should be prepared in the ER or trauma bay. Blood banks far from the ER or trauma bay would not be very effective compared to ABO RBCs. However, blood bank management may be difficult due to the lack of blood specialists in the trauma bay. In our center, UORBCs were managed by nurses in the trauma bay, therefore, other blood products such as fresh frozen plasma or concentrated platelets could not be prepared.
The improved clinical outcomes following early transfusion in trauma patients remain controversial. Prehospital pRBCs transfusion has been tried, but the results were inconclusive (1415). However, these studies had heterogeneous groups. In contrast, the present study used propensity score matching to make a homogenous group. The clinical outcomes were not significantly different in the current study, but all clinical outcomes were better in the UORBC group except for the ICU LOS, which was significantly longer in the UORBC group before matching. Especially, the number of 24-hour mortality, which could reflect death due to bleeding, was more than double in ABO RBC groups. Because the condition of the patients in the UORBC group was more severe than that of the patients in the ABO RBC, the group might be homogenous even after matching. It was expected that UORBC group could be more severe. Nevertheless, UORBC has potential benefits and non-inferior results at least; therefore, it seems acceptable to utilize UORBCs. Further study is required to determine the efficacy of UORBC transfusions and more specific inclusion criteria would be needed.
About half of the patients received massive transfusion after matching in this study. Unlike pRBCs, fresh frozen plasma or platelets could not be used immediately. However, early transfusion other than pRBCs was assessed (1617) because blood product ratios of 1:1:1 have been emphasized in severe trauma patients (181920). Recently, Yazer et al. (21) demonstrated the feasibility of cold-stored uncross-matched whole blood transfusion in civilian trauma patients, which resulted in faster 1:1:1 transfusions. Larger randomized trials are needed, but whole blood transfusion might be considered in the future.
In the current study, no transfusion-related critical adverse effects occurred in the UORBC group despite the fact that 75% of patients had ABO blood type mismatch. ABO mismatch is a well-known factor for alloimmunization (22), but type O pRBCs rarely result in critical reactions (23). Mulay et al. (24) reported acute hemolytic adverse reactions in 0.02% of UORBC transfusions and other adverse reaction in less than 0.3% of cases. It was less than probability of hemolytic reaction related with except ABO blood type (25). Moreover, the Rh negativity rate is about 0.1%–0.3% in Korea; thus, Rh-positive UORBCs could be safely utilized (26).
Our study had several limitations. First, there could be hidden variables in the propensity matching, which could affect the group homogeneity after matching. Second, not all cases of UORBC followed the indications. Third, this retrospective study had an insufficient number of patients.
In conclusion, the utilization of UORBCs resulted in faster transfusions, but did not improve the clinical outcomes in hemorrhagic shock patients in this study. However, there was a tendency for UORBC lower mortality and fewer massive transfusions. Larger studies are needed to assess the efficacy of UORBC transfusion.
 XML Download
XML Download