

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Recurrent pregnancy loss (RPL) is defined as 2 or more consecutive spontaneous miscarriages that occur usually before 20 weeks of gestation. RPL is a common, heterogeneous condition, with an estimated prevalence of 0.5%–3.0% in women of reproductive age (1). The cause of RPL is not apparent and clarification of the cause is difficult due to the heterogeneity of the condition. Suspected causes of RPL are parental chromosomal anomalies, anatomic, thrombophilic state, endocrinological disorders, immunological factors and nutrition/environmental factors, but the causes of RPL are suspected in only 50% of patients, and the remaining 50% remain unexplained (123).
The balance between coagulation and fibrinolysis is an essential part in early pregnancy, and thrombophilia has been postulated to be a contributor to the pathophysiology of RPL. Pregnancy is a hypercoagulable state with an increase in procoagulant factors and a decrease in the levels of anticoagulants (4). Inherited thrombophilia is associated with various obstetric complications such as RPL, stillbirth, fetal growth restriction, preeclampsia, and placental abruption (567). Methylenetetrahydrofolate reductase (MTHFR; GeneID: 4524) is a major regulatory enzyme in the metabolism of homocysteine (Hcy) that catalyses the reduction of 5, 10-methylenetetrahydrofolate to 5-methyltetrahydrofolate (8). Mutations in MTHFR gene lead to decreased activity of the enzyme and hyperhomocysteinemia, which then induces platelet aggregation by promoting endothelial oxidative damage (9). C677T and A1298C mutations are the two most common mutations within the MTHFR gene (10). C677T transition is a missense mutation in exon 4 of this gene, which converts an alanine to a valine residue in the N-terminal catalytic domain of the protein, resulting in decreased enzymatic activity (1112). Homozygous C677T mutations have been associated with elevated levels of Hcy and are identified as risk factors for thrombosis (13). Also, the MTHFR 677T allele was closely correlated with decreased MTHFR activity, resulting in a folate deficiency and increased plasma Hcy levels (14). A1298C is a point mutation in exon 7 of MTHFR gene and is characterized by a glutamate to alanine substitution within the C-terminal regulatory domain of the protein. A1298C polymorphism is also associated with decreased activity of the enzyme, but not to the same extent as the C677T polymorphism (1415).
Though the role of MTHFR C677T and A1298C mutations in RPL is not fully established, several studies have reported on the incidence of MTHFR C677T and A1298C mutations in women with RPL. Some of these studies have associated these mutations with the occurrence of RPL (911161718192021), while other studies have yielded diverse results (4222324252627). Therefore, we investigated the role of MTHFR polymorphisms in 302 patients with RPL and 315 controls in Korean population.
MATERIALS AND METHODS
Human subjects
As described in detail previously study (28), Korean women with or without RPL were recruited at five reproductive clinics from March 2012 to October 2014. A total of 302 RPL patients who had experienced at least 2 unexplained consecutive spontaneous miscarriages before 20 weeks of gestation were enrolled. They had no RPL which was defined by the American Society for Reproductive Medicine (ASRM) (1). Women with a confirmed reason for miscarriage, such as an anatomic cause, a parental chromosome abnormality, an autoimmune cause (including antiphospholipid antibody syndrome and systemic lupus erythematosus), an alloimmune cause (such as the presence of high natural killer cells), or endocrine abnormalities (such as hypothyroidism, hyperprolactinemia or diabetes) were excluded. Three hundred fifteen women served as controls who have visited the health-care center in Seoul National University Hospital for annual comprehensive medical checkup with no specific health problems. They had 2 or more normal term deliveries after uneventful pregnancies and no history of spontaneous miscarriage and underwent their menopause at an age older than 45 years. We recruited controls from this general population to rule out the probability that these subjects were affected by RPL.
MTHFR genotyping
DNA was extracted from peripheral blood samples with the Wizard® DNA purification kit (Promega, Madison, WI, USA). Allelic discrimination was performed using MGB-NFQ tagged primers and a Taqman probe on the ABI Prism 7500 Real Time PCR System (Applied Biosystems, Foster City, CA, USA). The following primers and probes were used: C677T forward primer, 5'-GCACTTGAAGGAGAAGGTGTCT-3', C677T reverse primer, 5'-CCTCAAAGAAAAGCTGCGTGATG-3', C677T reporter ‘C’, 5'- (VIC)-ATGAAATCGGCTCCCGC-(NFQ)-3', C677T reporter ‘T’ 5'-(FAM)-ATGAAATCGACTCCCGC-(NFQ)-3'; A1298C forward primer, 5'-GGAGGAGCTGCTGAAGATGTG-3', A1298C reverse primer, 5'-CCCGAGAGGTAAAGAACAAAGACTT-3', A1298C reporter ‘A’ 5'-(VIC)-ACCAGTGAAGAAAGTGT-(NFQ)-3', A1298C reporter ‘C’, 5'-(FAM)-CAGTGAAGCAAGTGT-(NFQ)-3'. Ten microliters of the 2 × TaqMan Universal PCR Master Mix (Applied Biosystems), and 25 ng DNA were used per reaction. The polymerase chain reaction (PCR) cycling conditions consisted of one 2-minute cycle at 50°C, and one 10-minute cycle at 95°C, followed by 40 cycles of 95°C for 15 seconds and 60°C for 1 minute. Distilled water was used as a negative PCR control in each amplification.
Statistical analysis
Power calculations were performed using Quanto v.1.2.4 software (http://biostats.usc.edu/cgi-bin/DownloadQuanto.pl). A 5% population prevalence of RPL was assumed (2), and minor allele frequencies were obtained from Korean studies (25). Given the number of enrolled subjects (302 PRL patients and 315 controls), the power for each single nucleotide polymorphism (SNP) ranged from 0.932 (C677T) to 0.852 (A1298C) for detecting an allelic odds ratio of 1.5 at α value of 0.05. In the controls, the genotype distribution was examined for significant departures from the Hardy-Weinberg equilibrium using a χ2 goodness-of-fit test, and all of the SNPs were in Hardy-Weinberg equilibrium.
Both the case and control groups were compared for their genotypic and allele frequencies. The significance of the differences in genotype distribution was assessed using a χ2 test, and continuous variables were compared using Student's t-test. Two-sided P values < 0.0.05 were considered statistically significant. Statistical data analyses were conducted using SPSS software packages, version 20.0 (IBM SPSS Inc., Armonk, NY, USA).
RESULTS
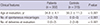
Ages of the RPL patients were significantly lower than that of the controls (34.8 ± 4.1 years vs. 50.3 ± 11.3 years, respectively, P < 0.001), and by definition, RPL patients had fewer deliveries and more miscarriages (median number of normal term delivery was 0 [range 0–2] in women with RPL and 2 [range 2–8] in controls, respectively, P < 0.001) and more miscarriages (median number of spontaneous miscarriages was 2 [range 2–10] in women with RPL and 0 [range 0–0] in controls, respectively, P < 0.001) (Table 1).
Table 1
Clinical features of RPL patients and controls
The genotype distributions of MTHFR C677T and A1298C in the RPL group did not differ from those of the controls (P = 0.142, P = 0.142, respectively) (Table 2). When the patients with three or more consecutive spontaneous miscarriages were analyzed, there was also no difference in genotype distribution between this subgroup and controls (Table 2). When the analysis was restricted to patients with no prior live birth, there was also no difference in genotype distribution between this subgroup and controls. The distribution of MTHFR genotypes followed Hardy-Weinberg equilibrium, which indicated that no selection occurred among genotypes.
Table 2
Genotype distribution of MTHFR C677T and A1298C in RPL patients and controls

DISCUSSION
In the present study, we evaluated the impact of MTHFR C677T and A1298C polymorphisms on the risk of RPL in a Korean population. According to our data, MTHFR C677T and A1298C genotype distribution in RPL patients did not differ significantly from control patients. While thrombophilia has been accepted as an etiology of recurrent miscarriage, the findings of the current study suggest that both polymorphisms are not major determinants of the development of RPL in Korean women.
Our findings are consistent with previous results in which a case-control study conducted in Japanese women showed no association of the MTHFR C677T polymorphism with RPL (22). Another study conducted in Iranian women also showed no correlation between the prevalence of homozygosis or heterozygosis for MTHFR C677T and A1298C mutations and RPL (26).
Results from several meta-analyses that have examined the possibility of an association between MTHFR polymorphisms and the risk of RPL are variable (293031323334353637). Data from a recent, large meta-analysis indicated that maternal and paternal MTHFR C677T and A1298C polymorphisms were associated with RPL. Moreover, a significant association was observed between fetal MTHFR A1298C mutation and RPL but not with the C677T mutation (35). Although subgroup analysis stratified by ethnicity was performed, no publication bias was detected. Nevertheless, there were limitations related to the clinical heterogeneity between the subjects in the included studies. For example, many studies included in the meta-analyses were inconsistent in defining RPL. Also, large differences in RSA definition in the number of miscarriages and broad gestational age criteria for RPL patients could be a reason for the discrepancy between studies. Furthermore, a large number of Chinese studies were included in these meta-analyses that may lead to potential ethnic variation; therefore, selection bias and publication bias may have occurred. When a recent meta-analysis of all available studies published from Asian population relating the C677T polymorphism to the risk of RPL was conducted, there was a strong association between the MTHFR C677T variant and RPL in Asian population and raising the importance of the use of folate in its treatment and prevention (37).
In a previous Korean study, there was no difference in genotype distribution of C677T and A1298C polymorphisms between the RPL group and the control group (25). Although our data is consistent with these results, the control subjects in our study had two or more normal term pregnancies and the mean age of controls was significantly higher than the mean age of RPL patients (50.3 ± 11.3 years vs. 34.8 ± 4.1 years; P < 0.001). For genetic association study, we tried to collect controls that are most unlikely to be affected by the disease. Recruiting controls who are older and have nearly gone through their reproductive periods maximizes the probability that these subjects are unaffected by RPL, which may favorably influence the results. In our current study, the frequency of the C677T allele in the control group was 20.5%, which was not different from the control groups used in the MTHFR polymorphism association studies of other diseases in Korea that had a range of 16.2% to 18.0% (383940).
Although our study did not find an association between MTHFR genotypes and RPL, our results need to be interpreted in context with the following drawbacks. First, Coulam et al. (23) analyzed 10 thrombophilic genes in women with recurrent miscarriages as well as in controls and found no differences in the frequencies of specific gene polymorphisms between the patients and controls. However, the prevalence of homozygotes and total gene mutations in patients was significantly higher than in controls, and the authors concluded that the association was manifested by the total number of mutations rather than by the specific genes involved. Second, we did not evaluate plasma Hcy or folate levels in our patients and therefore, it is possible that plasma Hcy levels in our patients may confound the association between MTHFR polymorphism and the risk of RPL. Finally, we cannot exclude the plausible involvement of MTHFR genotypes with other variables like life-style and hence provide inaccurate result. The effect of gene-environmental interactions or epigenetic modification was difficult to address in this study. Whether PRL patients and controls share similar environmental exposures such as endocrine disruptors, smoking, heavy metals, and indoor and outdoor pollutants were not evaluated in our study, but they come from a common ethnic — they were all Koreans — background. Our study has merits at this point.
We further analyzed the distribution of the variant genotypes in relation to disease severity, as indicated by the number of previous abortions. However, there was also no difference in genotype distribution between this subgroup and controls. We suggest that these results should be further elucidated in future research involving a higher number of severe cases of unexplained RPL and maternal-fetal interactions, gene to gene interactions, and environmental factors such as living habits and dietary folate intake should be taken into consideration.
Because an increased mean number of pregnancy losses may indicate that women are at an increased risk of recurrent miscarriage, the analysis was limited to patients with three or more consecutive spontaneous miscarriages. Nevertheless, there was no difference in genotype distribution between this subgroup and controls.
In conclusion, we did not observe significant differences in the genotype distribution of MTHFR C677T and A1298C polymorphisms between RPL patients and controls. Our study adds to existing data in the literature regarding MTHFR polymorphism and RPL in an Asian population. Although no association between these polymorphisms and RPL was found, the role of MTHFR in RPL demands further investigation given that thrombophilia has been postulated to be an important contributor in the pathogenesis of RPL.
 XML Download
XML Download