

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
The incidence of multifetal pregnancy has increased with the use of assisted reproductive technologies. Multifetal pregnancies increase the rate of preterm births, which compromise neonatal survival and increase the risk of lifelong disability. The infant mortality rate for multiple births is five times the rate as that for a singleton (1). These risks are magnified further with triplet or quadruplet births.
The determination of chorionicity antenatally in twin pregnancy is important for predicting pregnancy complications (2). It is well known that monochorionic (MC) twin pregnancies are associated with higher mortality and morbidity than dichorionic twin pregnancies due to hemodynamic imbalance (3). Monoamniotic (MA) twin pregnancies account for only 1% of all monozygotic twins and are associated with high fetal death rates from cord entanglement, congenital anomalies, and preterm birth (4). Therefore, accurate determination of amnionicity is an important first step for establishing a clinical management plan and counseling women with MC multifetal pregnancies and their family members about pregnancy outcomes.
Determination of amnionicity in MC multifetal pregnancies is typically done around 8 weeks of gestation by visualization of the dividing amniotic membrane (5). The amniotic membrane develops concurrently with the yolk sac, but it is difficult to visualize early in the first trimester because the membrane is closely applied to the developing embryo without amniotic fluid between the embryo and the amnion. The amnion only becomes visible once there is enough fluid separating the embryo from the membrane. Therefore, the number of yolk sacs may be used to diagnose amnionicity initially (6).
Recently, the accuracy of the relationship between the number of yolk sacs and amnionicity has been called into question (789). In addition, we have experienced several cases of MC multifetal gestations with discrepancies between the number of yolk sacs and amnionicity. To the best of our knowledge, previous reports have been case reports or very small studies. Therefore, we evaluated the accuracy of the number of yolk sacs for predicting amnionicity in MC multifetal pregnancies during early first trimester ultrasound examination.
MATERIALS AND METHODS
This was a retrospective analysis of prospectively collected data from patients with MC multifetal gestations from October 2004 to December 2014 at Cheil General Hospital and Women's Healthcare Center. During the study period, a total of 97 viable MC multifetal pregnancies were identified via ultrasound between 7 + 0 and 9 + 6 weeks of gestation. Ultrasonography was performed using transvaginal and transabdominal transducers with one of the following ultrasound models (Voluson E8, Voluson 730; GE Healthcare, Milwaukee, WI, USA) by five obstetricians, each with more than five years of experience performing first trimester scans. In our center, all pregnant women with multifetal pregnancies were advised to receive fetal ultrasonography between 7 + 0 and 9 + 6 gestational weeks for determination of chorionicity and amnionicity. When determination of chorionicity or amnionicity was uncertain, the patient underwent sonography again by another senior staff. Follow-up fetal sonography was performed, usually two weeks later at 9–11 weeks of gestation by two examiners. In each scan, the number of gestational sacs, number of yolk sacs within each gestational sac, presence or absence of a dividing membrane, number of fetuses, crown-rump length (CRL), fetal heart rate, and presence or absence of associated fetal anomaly were documented.
Chorionicity and amnionicity were documented by serial ultrasound assessment of the dividing membrane and/or confirmed by postpartum pathologic examination of the placenta. Chorionicity was determined by assessing the number of gestational sacs and a dividing membrane within the gestational sac was considered adequate evidence of diamnionicity. When two dividing membranes were identified within a single gestational sac, we determined the case to be a MC triamniotic (TA) triplet pregnancy. We reviewed the all images in each case for the purpose of the study.
Gestational age (GA) was calculated from the first day of the last menstrual period and was confirmed by CRL measurement in the first trimester of pregnancy. When estimated GA by menstrual date varied from ultrasound date by more than 5 days, we used the ultrasound performed between 7 + 0 and 9 + 6 weeks of pregnancy to estimate GA. In cases of in vitro fertilization (IVF), the ovum pick-up day was defined as intrauterine pregnancy (IUP) 2 + 0 gestational weeks.
RESULTS
During the study period, a total of 97 cases of MC multifetal pregnancy were identified, including 83 cases of diamniotic (DA) twins, 11 cases of MA twins, and 3 cases of TA triplets. The mean maternal age of the study group was 32.2 ± 3.9 years old and 71 (66.0%) of the women were nulliparous. The median GA at the first ultrasound scan was 8.0 ± 1.3 weeks of gestation. The most common method of conception was natural (69%), and other maternal characteristics are shown in Table 1.
Table 1
Clinical characteristics of the study population
| Characteristic | Value |
|---|---|
| Maternal age, yr | 32.2 ± 3.9 |
| Nulliparity | 71 (66.0) |
| GA at initial US scan, wk | 8.0 ± 1.3 |
| Method of conception | |
| Natural | 67 (69.1) |
| IVF | 26 (26.8) |
| Ovulation-induction | 4 (4.1) |
Nine cases (9.3%) showed discrepancies between the number of yolk sacs determined on initial ultrasound examination and the amnionicity confirmed by the presence and number of dividing membranes in serial follow-up sonography and/or gross postpartum evaluation of the membrane (Table 2). In the 76 cases delivered after 20 weeks gestation, amnionicity and chorionicity was confirmed by placental pathology. Among 11 confirmed cases of MA twins, 7 (63.6%) had a single yolk sac and 4 (36.4%) showed two yolk sacs. The 4 cases of monochorionic monoamniotic (MCMA) twins with two yolk sacs underwent transabdominal and transvaginal ultrasonography at 7–9 weeks of gestation (Fig. 1). Two viable embryos were identified within a single gestational sac, but a dividing membrane was not found in the initial scan or serial follow-up sonography.
Table 2
Discrepancy rates between confirmed amnionicity and the number of yolk sacs on ultrasonography
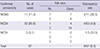
Fig. 1
Transvaginal ultrasound at 9 weeks of gestation demonstrates two yolk sacs in a MCMA pregnancy.
MCMA = monochorionic monoamniotic.

Among the studied cases, monochorionic diamniotic (MCDA) twins were most common (85.6%, 83/97). The number of yolks sac (two yolk sacs) corresponded with amnionicity (diamnionicity) in 79 pregnant women (95.2%, 79/83). However, four cases (4.8%) of confirmed DA twins showed only a single yolk sac and a distinct dividing intertwine membrane in initial and serial follow-up scans (Fig. 2). In three cases of TA triplets, one showed a discrepancy between confirmed amnionicity and the number of yolk sacs visualized by ultrasonography examination. In a single gestational sac, three viable embryos with two yolk sacs were identified at 7 + 1 weeks of gestation by initial ultrasound. Serial sonograms showed a distinct dividing membrane as epsilon sign.
Fig. 2
Transvaginal ultrasound at 9 weeks of gestation demonstrates a single yolk sac in a MCDA pregnancy.
MCDA = monochorionic diamniotic.

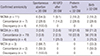
As described in Table 3, pregnancy outcomes differed according to the difference between the number of the yolk sacs and the amnionicity. The spontaneous abortion rates before 20 weeks of gestation were more common in discrepancy cases in the MCMA and the monochorionic triamniotic (MCTA) group (concordance vs. discrepancy; MCMA: 28.6% vs. 100%, MCTA: 50.0% vs. 100%). Both fetal demise occurred before 16 weeks of gestation in all four MCMA cases with two yolk sacs. In the MCTA case with two yolk sacs, absence of cardiac activity of all three fetuses were found at the GA of 14 weeks and 2 days. Among the aborted cases with shown discrepancy between the numbers of amnion and yolk sacs in study group, all four cases of MCMA twins showed cord entanglement. Therefore, monoamnionicity was confirmed. However, other abnormal fetal sonographic findings were not seen. In one aborted MCTA case, abnormal sonographic findings were not found. Intrauterine fetal death (IUFD) after 20 weeks of gestation did not occur in the MCMA and MCTA groups in this study. However, sudden intrauterine death of both twins at 23 + 3 gestational weeks was found in a MCDA case with discrepancy between the number of yolk sacs and amnionicity. Only 2 cases of IUFD occurred in concordance cases in the MCDA group therefore the IUFD rate was more frequent in discrepancy cases (concordance vs. discrepancy; 2.5% vs. 25.0%). However, three women with discrepancy in the MCDA group delivered after 32 weeks of gestation.
Table 3
Pregnancy outcomes according to the concordance or the discrepancy between the number of the yolk sacs and the confirmed amnionicity
DISCUSSION
Compared with dichorionic pregnancies, MC multiple pregnancies have different and unique complications including sudden fetal death, fetal anomalies, selective intrauterine growth restriction, premature birth, twin-to-twin transfusion syndrome, and twin anemia polycythemia sequence (1011). Therefore, chorionicity impacts obstetric management as well as the risk for complications and adverse perinatal outcomes. Correct assignment of chorionicity rates are close to 100% when performed in the early first trimester by counting the number of gestational sacs (12).
Establishing amnionicity is also of paramount importance in MC twin pregnancies because MA twins have the highest fetal mortality rate due to umbilical cord entanglement. Therefore, early diagnosis of amnionicity is crucial for planning management strategies and treatment options, which can result in improved fetal outcomes. Amnionicity in MC multifetal pregnancies can accurately be determined around 8 weeks of gestation by visualization of the dividing amniotic membrane (5). However, in cases of MC twins, visualization of intervening membrane is difficult early in the first trimester because the membrane is so closely applied to the developing embryo without amniotic fluid between the embryo and the amnion. It leads to an incorrect diagnosis of monoamnionicity. Counting the number of yolk sacs has been considered an important alternative method for predicting amnionicity in MC multifetal pregnancies (5).
Recently, this concept has been challenged by several reports (781314). However, these studies focused on a single yolk sac in MC twin pregnancies, which tend to be associated with monoamnionicity, and were limited by a relatively small number of MC pregnancies or by case reports (9). In our study of 97 MC multifetal pregnancies, 9 cases (9.3%) showed discrepancies between the number of yolk sacs visualized by initial ultrasound examination and amnionicity confirmed by the presence and number of dividing membranes in serial follow-up sonography and/or gross postpartum membrane evaluation. Discrepancy rates seem to be more common in cases of MA twins (36.3%) and TA triplets (33.3%) than in DA twins (4.8%). In cases of DA twins and TA triplets showing discrepant results, the number of yolk sacs was smaller than the order of amnionicity. This finding corresponds with a previous study correlating yolk sacs with amnionicity by Shen et al. (7), which analyzed 20 MCDA pregnancies. They suggested that yolk sac differentiation occurs after that of the chorion and before that of the amnion. The number of yolk sacs depends on the timing of cleavage of monozygotic twinning, before or after yolk sac differentiation. This could explain the smaller number of yolk sacs in DA twins and TA triplets. That is, when cleavage of monozygotic twinning occurs after yolk sac differentiation and before amnion differentiation, a smaller number of yolk sacs result. Because yolk sac differentiation occurs shortly before that of the amnion, the majority of cases of DA twins have two yolk sacs. In our study, 79 of 83 cases of DA twins (95.2%) showed 2 yolks sacs.
On the other hand, 4 of 11 cases of MA twins (36.4%) had two yolk sacs. Possible explanations for the presence of two yolks sac in MCMA twins were suggested by Murakoshi et al. (9). In their case report, they proposed that spontaneous rupture of the dividing membrane or the creation of an incomplete dividing membrane may be the cause of two yolk sacs.
We analyzed 97 cases of MC multifetal pregnancy, including 83 cases of MCDA twins, 11 cases of MCMA twins, and 3 cases of MCTA triplet pregnancies. Statistically, there is no difference in discrepancy rate between assisted reproductive technology (ART) pregnancy (10.0%, 3/30) and spontaneous conception group (8.96%, 6/67). Therefore, the discrepancy between the number of yolk sacs and amnionicity seems not to be affected by ART. This study reviews the largest number of cases in a single center for determining amnionicity in the early first trimester period. Compared to all deliveries of our center, the incidence of MC multifetal pregnancy is less than estimated incidence. We have included only viable cases with confirmed presence of fetal heartbeat. Absence of fetal heartbeat was excluded from this study.
Yolk sac and amnion differentiation occur around the same time, about 6–8 days after conception. By transvaginal ultrasonography, the yolk sac (specifically, the secondary yolk sac) may be visible as early as 5 gestational weeks and it is almost always seen by 5.5 weeks (15). The amniotic membrane develops concurrently with the yolk sac, but it is difficult to visualize until the end of the 6th gestational week (16), because the membrane is closely applied to the developing embryo without amniotic fluid between the embryo and the amnion. The amnion around each of the embryos cannot be imaged reliably until 8 weeks of gestation. Therefore, definite determination of amnionicity by the presence or absence of amnion around each of the embryos should be postponed until at least 8 gestational weeks in MC multifetal pregnancies. Recently, Meller et al. (14) reported their experiences about assigning amnionicity in the first trimester based on the number of yolk sacs between 2010 and 2013. In this clinical letter, there are 4 cases of MCMA in which 1/4 were discrepant in number of yolk sacs per amnion and 47 cases of DCDA in which all were concordant with yolk sac and amnion. They also suggested besides the number of yolk sacs, additional markers (the number of amniotic sacs, dividing membrane, and umbilical cord entanglement) need to be evaluated to make an accurate diagnosis of amnionicity.
In cases of discrepancy in this study, except that of a single yolk sac in DA twins, obstetric outcomes were unfavorable. All four MCMA cases with 2 yolk sacs were aborted before 16 weeks of gestation. One case of MCTA with 2 yolk sacs was aborted at 14 + 2 weeks GA. However, among the four discrepant cases in the MCDA group, 3 women delivered after 32 weeks of gestation and one case resulted in sudden intrauterine death of both twins at 23 + 3 gestational weeks. We speculate that poor prognosis in early gestation is one reason for the small number of cases in previous studies. Stampone et al. (17) have documented a high rate of pregnancy failure when the diameter of the yolk sac is more than 7 mm. Because only cases with identified embryonic heart beat are included in this study, there is no case with large size (above 7 mm) or distorted shape of yolk sac. Aborted cases shown discrepancy could be subdivided into the larger number of yolk sac (two yolk sacs in MCMA twins) and the smaller number of yolk sac groups (one yolk sac in MCDA and two yolk sacs in MCTA pregnancy). Spontaneous abortion occurred more commonly in the larger number of yolk sac group than the smaller number of yolk sac group (100%, 4/4 vs. 25%, 1/4). We speculate that the above mentioned mechanism of discrepancy between the number of yolk sacs and the number of amnion may be the reason for this different rate of abortion between the two groups. That is, some pathologic event in the early pregnancy period, such as spontaneous rupture of the dividing membrane or the creation of an incomplete dividing membrane, may be the cause of two yolk sacs in MCMA twins. Spontaneous abortion could be more commonly associated with this pathologic event. On the other hand, the mechanism of smaller number of yolk sacs is not pathologic but merely timing of cleavage of monozygotic twinning-cleavage occurs after yolk sac differentiation and before amnion differentiation. Therefore, the risk of spontaneous abortion was not higher than the larger number of yolk sac group.
The ability to accurately predict amnionicity at an early stage is important in MC twin pregnancies because the prognosis of a MCMA pregnancy is worse than that of a MCDA pregnancy due to umbilical cord entanglement. The detection of a dividing membrane within the gestational sac ensures the presence of two amnions in MC gestation. While the number of yolk sacs tend to equal the number of amnions early in gestation, the diagnosis of amnionicity using the number of yolk sacs in MC multifetal pregnancy was not reliable in our study. Therefore, the determination of amnionicity in MC multifetal pregnancies is best deferred to a later stage, no earlier than 8 weeks of gestation, when the presence or absence of an amniotic membrane within the gestational sac can be determined with certainty by serial follow-up ultrasound examinations.
In conclusion, in 9.3% of MC gestations, the number of yolk sacs did not correlate with the number of amnions in our study. To determine amnionicity in MC multifetal pregnancies, we recommend careful evaluation not of the number of yolk sacs but the presence or absence of intertwine dividing membrane after 8 gestational weeks.
 XML Download
XML Download