

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Coronary artery bypass grafting (CABG) has demonstrated improvement of left ventricular (LV) function and shown excellent long-term results in patients with ischemic LV dysfunction (12). However, a wide variety of patient populations were reported in the studies that examined patients who showed LV function improvement after CABG (345). Gadolinium-enhanced cardiac magnetic resonance (CMR) imaging has been suggested as a superior modality for predicting lack of functional recovery in chronic ischemic cardiomyopathy and is currently accepted as the standard of reference to determine ventricular function (67). Previous gadolinium-enhanced CMR studies demonstrated an association between the degree of late gadolinium enhancement (LGE) and myocardial viability after revascularization (89). However, CMR parameters that predicted improvement of global LV function after CABG have not been determined. The aims of this study were to evaluate the echocardiographic changes in LV ejection fraction (LVEF) in CABG patients with LV dysfunction, and to examine CMR parameters as predictors of postoperative LVEF improvement.
MATERIALS AND METHODS
Patient characteristics
Of 667 consecutive patients who underwent first-time isolated CABG (663 off-pump CABGs and 4 on-pump CABGs) between January 2010 and June 2014, 102 patients (100 off-pump CABGs + 2 on-pump CABGs) had LV dysfunction (LVEF ≤ 35% by preoperative transthoracic echocardiogram). Among the 102 patients, 78 patients underwent preoperative gadolinium-enhanced CMR to assess myocardial viability and 77 of those patients (76 off-pump CABGs + 1 on-pump CABG) were included in the present study. One patient whose CMR quality was inadequate to analyze was excluded (Fig. 1). One patient who underwent off-pump revascularization was converted to on-pump due to a left atrial fibroelastoma that was detected incidentally on intraoperative transesophageal echocardiography. Gadolinium-enhanced CMR was performed at median 4 days (1–63) preoperatively. Mean age at operation was 64 ± 11 years, and LVEF measured by preoperative transthoracic echocardiography was 28.5% ± 5.5% (range, 12.0%–35.0%). Thirty-six patients had mitral regurgitation (mild, moderate, and moderate to severe in 28, 7, and 1 patients, respectively) (Table 1). Twenty-five excluded patients more frequently had worse preoperative conditions prohibiting CMR with LGE such as preoperative intra-aortic balloon pump (IABP) therapy, urgent or emergency operation, and chronic renal failure (Table 1). During the study period, 7 patients who underwent combined cardiac surgery requiring cardiopulmonary bypass and aortic cross clamp were excluded; 5 patients underwent Dor procedure due to LV aneurysm, and 2 patients with moderate mitral regurgitation underwent concomitant mitral annuloplasty.
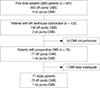 | Fig. 1Summary flow diagram showing patient enrollment.
CABG = coronary artery bypass grafting, CMR = cardiac magnetic resonance.
|
Table 1
Preoperative characteristics and risk factors of the 77 study patients

Values are mean ± standard deviation, median (ranges), or number (%).
EUroSCORE = European System for Cardiac Operative Risk Evaluation, BMI = body mass index, PCI = percutaneous coronary intervention, MI = myocardial infarction, IABP = intra-aortic balloon pump, LVEF = left ventricular ejection fraction.
![]()
Revascularization strategies
Basic principles and surgical procedures of CABG have been previously described (10). Anaortic off-pump CABG was performed in all study patients except one patient who underwent on-pump conversion after off-pump revascularization. Seventy-five patients underwent revascularization using a composite graft based on the left internal thoracic artery (ITA), and two patients were revascularized using a composite graft based on the in situ right ITA due to an unusable left ITA. Second conduits created for the ITA composite graft used the saphenous vein (SV; n = 72), right ITA (n = 4), and right gastroepiploic artery (n = 1). Arterial conduits were harvested using a skeletonization technique and the SV was harvested using a minimal manipulation technique after systemic heparinization. The second conduit was anastomosed to the side or end of the ITA in either a Y or I fashion. All the diseased vessels with significant (≥ 70% diameter) stenoses were revascularized whenever possible, regardless of the grade of LGE. Complete revascularization, defined as at least 1 graft to each of the diseased 3 major coronary artery territories, was achieved in 69 patients (89.6%) except in the following 8 patients: 5 patients had too small target vessel (< 1 mm diameter), 2 patients had intramyocardial obtuse marginal branch, and 1 patient had a heavily calcified posterior descending coronary artery. The number of distal anastomoses per patient was 3.6 ± 0.9. An IABP was inserted in 15 patients in whom off-pump revascularization of inferolateral coronary artery territory was expected to be difficult because of severe LV dysfunction and an enlarged LV. All patients took aspirin (200 mg/day) until the day of surgery and resumed taking it as soon as possible after surgery, usually 1 day postoperatively.
Acquisition and analysis of CMR data
The CMR was performed using a 1.5-T scanner (Sonata Magnetom; Siemens, Erlangen, Germany) at median 4 (1–63) days preoperatively. Cine images were acquired with a steady-state free precession technique (TrueFISP, repetition time/echo time of 2.2/1.1 ms; flip angle of 80 degrees; typical pixel size of 1.5 × 1.5 mm; slice thickness of 6 mm; slice gap of 4 mm; and temporal resolution of 20 phases per each cardiac cycle) (11). Ten to twelve short-axis slices were planned in the 4- and 2-chamber views to cover the entire ventricle. The LGE images were acquired 10 minutes after an injection of gadopentetate dimeglumine (0.2 mmol/kg; Magnevist; Schering, Berlin, Germany) and a flush of saline (20 mL). The LGE images were acquired in the same planes as the cine images by using inversion recovery segmented spoiled-gradient echo and phase-sensitive inversion recovery methods. Two board certified cardiovascular radiologists blinded to clinical data independently reviewed the CMR data and consensus was reached after review. The LV volumes were analyzed on a computer using dedicated software (QMASS MR; Medis, Leiden, the Netherlands). Cine loops were reviewed, and end-diastolic and end-systolic frames were identified. Epicardial and endocardial contours were manually traced from the most basal to the most apical slices. The LV end-diastolic volume index (LVEDVI), LV end-systolic volume index (LVESVI), and LVEF were measured. Contiguous short-axis images were split from base to apex of the LV and divided into 17 segments. A 16-segment model, after subtracting the apical cap of the 17-segment model, was used for analysis because the apical cap was too thin to be evaluated (12). The transmural extent of LGE was visually graded on a 5-point scale (absence of LGE, grade 0; transmural LGE 0%–25%, grade 1; transmural LGE 26%–50%, grade 2; transmural LGE 51%–75%, grade 3; transmural LGE 76%–100%, grade 4). A viable myocardial segment was defined as a myocardial segment with a transmural extent of LGE ≤ 50% (grades 0 to 2), including both normal and dysfunctional segments. Segmental wall motion also was visually graded on a 5-point scale (normokinesia, 0; hypokinesia, 1; akinesia, 2; dyskinesia, 3; and aneurysm, 4) (13). A dysfunctional viable myocardial segment was defined as a viable myocardial segment showing abnormal wall motion (grades 1 to 4).
Serial follow-up of LV function
Transthoracic echocardiography was performed preoperatively and prior to discharge (median 6 [range, 1–12] days postoperatively) in all the study patients (n = 77), and during the 1st postoperative year (median 11 [3–12] months) in 70 of 77 study patients. The LVEF was considered to be improved if there was an absolute increase of LVEF value ≥ 5% (314). The proportional changes in LVEF based on the preoperative value (follow-up LVEF minus preoperative LVEF and divided by preoperative LVEF) also were calculated and expressed as percent value.
Statistical analysis
Statistical analysis was performed using the SPSS software package (version 12.0; SPSS Inc., Chicago, IL, USA). Data were expressed as mean ± standard deviation, median with ranges, or proportions. Comparisons between the 2 groups were performed with the χ2 test for categorical variables and Student's t-test for continuous variables. The survival rates were estimated using the Kaplan-Meier method. Predictors of LVEF improvement (LVEF ≥ 5%, categorical variable) and proportional changes in LVEF (continuous variable) were analyzed using multivariable logistic regression and linear regression models, respectively. A cut-off value of number of viable myocardial segment was determined by a minimal P value approach where the cut-off value was selected at the point showing the lowest P value, and number of viable myocardial segments was entered in these analyses as a categorical variable (15). Variables with a P value < 0.1 in univariate analyses were entered into multivariable models. Factors with a P value < 0.05 were considered as statistically significant.
Ethics statement
The study protocol was reviewed by the Institutional Review Board of Seoul National University Hospital and approved as a minimal risk retrospective study (approval number: H-1607-050-773) that did not require individual consent based on the institutional guidelines for waiving consent.
RESULTS
Preoperative CMR data
Mean preoperative LVEF by CMR was 27.6% ± 7.9%, and preoperative LVEDVI and LVESVI were 156.4 ± 38.5 mL/m2 and 115.9 ± 34.5 mL/m2, respectively. Of 1,232 total segments seen in the preoperative CMR, there were 662, 240, 153, 95, and 82 segments in LGE grades 0, 1, 2, 3, and 4, respectively. The median numbers of viable myocardial segments and dysfunctional viable myocardial segments were 14 (9–16) and 9 (0–16), respectively, in the 16-segment model. Mean wall motion score index was 31.7 ± 5.9.
Early clinical outcomes
Operative mortality (any death within 30 days, including deaths after hospital discharge and any death occurring during the hospitalization in which the operation was performed, even if after 30 days) was 0%. Postoperative complications included atrial fibrillation (n = 21, 27.3%), acute renal failure (n = 5, 6.5%), bleeding reoperation (n = 1, 1.3%), and mediastinitis (n = 1, 1.3%). No patient suffered from stroke after surgery. In the 25 excluded patients, 2 patients died after surgery: one patients died 11 days after surgery due to lower leg ischemia related with pre-existing arteriosclerosis obliterans, and the other patient died 36 days after operation due to ischemic bowel infarction.
Improvement of LV function evaluated by echocardiography
Mean LVEF values preoperatively, prior to discharge, and during the 1st postoperative year were 28.5% ± 5.5%, 31.6% ± 7.7%, and 41.1% ± 11.6%, respectively. Improvement of LVEF (absolute increase ≥ 5%) was found in 73% (51 of 70) of the patients; 27 patients at postoperative median 6 days and the remaining 24 patients at postoperative median 11 months (Fig. 2). In 27 patients who showed LVEF improvement prior to discharge, LVEF further improved during the 1st postoperative year (prior to discharge vs. during the 1st postoperative year, 37.1% ± 7.6% vs. 43.3% ± 11.6%; P = 0.006). Proportional changes of LVEF prior to discharge and during the 1st postoperative year compared with the preoperative value were 14% ± 28% and 57% ± 45%, respectively (P < 0.001).
 | Fig. 2Serial changes in LVEF at Pre and Post periods, and during the first year postoperative FU.
(A) LVEF changes in 51 patients who showed absolute increase of LVEF. (B) LVEF changes in 19 patients in whom LVEF was not improved.
LVEF = left ventricular ejection fraction, Pre = preoperative, Post = early postoperative, FU = follow-up.
|
Predictors of LV function improvement
After univariate analyses, the number of viable myocardial segments (median ≥ 14), LVEDVI, and age were associated with an absolute increase of LVEF (≥ 5%). The number of dysfunctional but viable myocardial segments was not related to increased LVEF (≥ 5%). Multivariable analyses revealed that the number of viable myocardial segments (median ≥ 14) was the only statistically significant factor for absolute increase of LVEF (odds ratio = 4.399; P = 0.046) (Table 2). Factors for proportional changes in LVEF improvement were also analyzed using linear regression analyses. After univariate analyses, the number of viable myocardial segments (median ≥ 14), LVEDVI, and acute coronary syndrome were associated with proportional changes in LVEF. Multivariable analyses revealed that the number of viable myocardial segments (median ≥ 14 with LGE ≤ 50%) was the most statistically significant factor for proportional changes in LVEF during the 1st postoperative year (β ± standard error = 28.749 ± 10.476; P = 0.008; R2 = 0.137; Table 2).
Table 2
Multivariable analyses for factors associated with absolute increase (≥5%) and proportional changes in LVEF

LVEF = left ventricular ejection fraction, OR = odds ratio, CI = confidence interval, LVEDVI = left ventricular end-diastolic volume index.
*Number of viable (transmurality of infarct scar on late gadolinium enhancement ≤ 50%) myocardial segments ≥ 14.
![]()
Long-term clinical outcomes
During the follow-up, late deaths occurred in 24 patients including 7 cardiac deaths. Two patients were admitted due to congestive heart failure at 4 months and 5.5 years after surgery. Overall survival rates at 5 and 7 years were 67.8% and 61.1%, respectively. Freedom from composite event of cardiac death or readmission due to congestive heart failure at 5 and 7 years were 89.2% and 83.9%, respectively. Both overall survival and freedom from composite event rates were higher in patients with viable myocardial segments ≥ 14 than those with viable myocardial segments < 14 without any statistically significant differences (P = 0.600 and P = 0.423, respectively) (Fig. 3). Cox regression analyses demonstrated that only age was associated with overall survival with statistical significance (P = 0.001) and freedom from composite event rate with a marginal significance (P = 0.057).

DISCUSSION
The present study demonstrated two main findings. First, improvement of LVEF during the 1st postoperative year was found in approximately 75% of patients with LV dysfunction, and greater proportional changes in LVEF improvement were observed at median 11 months postoperatively. Second, the number of viable myocardial segments (median ≥ 14) seen in preoperative CMR was a significant factor for both absolute increase (≥ 5%) and proportional changes in LVEF after CABG during the 1st postoperative year in patients with LV dysfunction.
Despite on-going development of percutaneous technology (16), previous studies demonstrated the salutary effect of CABG as a progressive improvement of myocardial blood flow and function (141718), resulting in favorable clinical outcomes compared to optimal medical therapy even in patients with severely depressed LV function (12). However, a wide variety of patient populations were reported in studies examining patients who showed LV function improvement after CABG (345). One previous study demonstrated that 35% of 62 study patients with ischemic LV dysfunction showed LVEF improvement 3 months after CABG (3). Another study showed that improvement of LVEF was observed in 50% of the enrolled patients median 7 days after CABG (4). In the present study, 73% of 70 patients with LV dysfunction showed an improvement of LVEF during the first year after CABG. Similar to a previous study which suggested a progressive improvement of myocardial perfusion until 1 year after CABG (18), postoperative LVEF improvement was observed in 55% of patients prior to discharge and in the remaining 45% of patients at postoperative median 11 months. In addition, greater proportional changes in LVEF improvement were observed at postoperative median 11 months than prior to discharge in the present study.
Gadolinium-enhanced CMR studies demonstrated that dysfunctional segments with LGE of greater than 50% had little chance of functional improvement, and CMR imaging has been suggested as a superior modality for predicting lack of functional recovery in ischemic cardiomyopathy (78). Later studies suggested that LGE-CMR derived myocardial viability could predict functional improvement of regional LV myocardial segments after successful revascularization (9192021). However, the relation between the LGE-CMR derived segmental myocardial viability and improvement of global LV function improvement was not studied thoroughly. One previous study demonstrated that an increasing extent of dysfunctional but viable myocardial segments (segments with LGE ≤ 25% and abnormal contractility) before revascularization correlated with LVEF improvement (7). Another study demonstrated that the number of scar segments (≤ 4 segments with LGE > 50%) predicted global LVEF improvement (≥ 5%) 6 months after CABG (22). The other study showed that the sum of viable + normal segments (≥ 10 segments with LGE < 50%) predicted LVEF improvement (≥ 3%) 6 months after CABG (23). The present study also revealed that the number of viable myocardial segments (including both normal and dysfunctional viable segments, but not the number of dysfunctional viable myocardial segments) was associated with improvement of global LVEF after CABG. The present study showed that only the sum of normal + dysfunctional viable segments predicted LVEF improvement after CABG. This may be explained by incorporation of normal + dysfunctional viable segments contributing to the end-point of LVEF improvement even though normal segments did not improve further after revascularization and made no contribution to an increase in LVEF (823). In addition, the present study analyzed factors of proportional changes in LVEF improvement because analysis of absolute LVEF improvement might be limited in patients with different preoperative LVEF. The multivariable analysis revealed that the number of viable myocardial segments (normal + dysfunctional viable segments) was the only statistically significant factor for proportional changes in LVEF during the 1st postoperative year.
There are limitations to the present study that must be recognized. First, this study was not performed in a prospective manner and the number of patients enrolled was relatively small. Second, serial echocardiographic follow-up study was not performed in all patients and follow-up echocardiography was performed in a wide range of time period up to 1 year after surgery. Third, there were no statistically significant associations between CMR parameters and long-term clinical outcomes. Further study in a larger patient cohort with longer-term follow-up might be needed to identify parameters associated with long-term clinical outcomes.
 XML Download
XML Download